
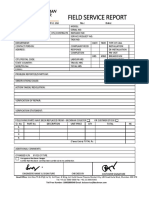
(Converge) O.T FORM - GP
(Converge) O.T FORM - GP
You might also like
- 2019 Business Credit with no Personal Guarantee: Get over 200K in Business Credit without using your SSNFrom Everand2019 Business Credit with no Personal Guarantee: Get over 200K in Business Credit without using your SSNRating: 4.5 out of 5 stars4.5/5 (3)
- Clearance Form - Employee Turn-Over ChecklistDocument2 pagesClearance Form - Employee Turn-Over Checklistjurex salomonNo ratings yet
- 57984c89bf389 (BPI CAP) Account Opening Form and Client Agreement 04-06-2016Document15 pages57984c89bf389 (BPI CAP) Account Opening Form and Client Agreement 04-06-2016Nancy Hernandez- TurlaNo ratings yet
- Application Form: Republic of The PhilippinesDocument3 pagesApplication Form: Republic of The PhilippinesAllan Diel CaranguianNo ratings yet
- 0T Form - GP ArmanDocument1 page0T Form - GP ArmanshaiNo ratings yet
- 0T Form - GP AnthonyDocument1 page0T Form - GP AnthonyshaiNo ratings yet
- Official Business Information Control Sheet: UrgentDocument3 pagesOfficial Business Information Control Sheet: UrgentnehllajacintoNo ratings yet
- Occupancy TemporaryDocument4 pagesOccupancy TemporaryVicente Ali Diaz SanchezNo ratings yet
- ZIMRA - Internal Funds Transfer FormDocument1 pageZIMRA - Internal Funds Transfer FormSimbarashe Mugoni0% (1)
- Field Service Report: Beckman Coulter India Pvt. Ltd. No.: DateDocument1 pageField Service Report: Beckman Coulter India Pvt. Ltd. No.: DateBrahmananda ChakrabortyNo ratings yet
- Clearance Form (CF)Document1 pageClearance Form (CF)kimberly magallanesNo ratings yet
- Oimb Citizens Charter 10 04 Cor 12 DealerDocument1 pageOimb Citizens Charter 10 04 Cor 12 DealerMuhammad Hasher AnjalinNo ratings yet
- Edeclaration of Source Funds FormDocument2 pagesEdeclaration of Source Funds FormRaymond WilliamsNo ratings yet
- Software Service CallDocument1 pageSoftware Service CallPawan RaiNo ratings yet
- Type of Application: New Renewal Application/Control No: Mode of Release: Pick-Up MailDocument2 pagesType of Application: New Renewal Application/Control No: Mode of Release: Pick-Up MailSheanaNo ratings yet
- Definition of TermsDocument4 pagesDefinition of TermsTopher ReyesNo ratings yet
- Ot Request FormDocument1 pageOt Request Formjoehanz.hrdNo ratings yet
- Republic of The Philippines Department of Transportation and Communications STCW OfficeDocument1 pageRepublic of The Philippines Department of Transportation and Communications STCW OfficeHeralynn BaloloyNo ratings yet
- Client Clearance Form (CCF)Document1 pageClient Clearance Form (CCF)kimberly magallanesNo ratings yet
- Reimbursement FormDocument1 pageReimbursement FormcampNo ratings yet
- Kori Engineering Credit Application FormDocument6 pagesKori Engineering Credit Application Formaj.ngadaNo ratings yet
- Type of Application: New Renewal Application/Control No: Mode of Release: Pick-Up MailDocument1 pageType of Application: New Renewal Application/Control No: Mode of Release: Pick-Up MailMuhammad Hasher AnjalinNo ratings yet
- SLF103 ApplicationRefundExcessSTLAmortization V06Document1 pageSLF103 ApplicationRefundExcessSTLAmortization V06Ina Marie BalajadiaNo ratings yet
- ClearanceDocument5 pagesClearancelouise matsuiNo ratings yet
- Business Permit FormDocument2 pagesBusiness Permit FormNicole De VillaNo ratings yet
- Company Subsidized Account/ Sole Proprietorship Company Managed AccountDocument1 pageCompany Subsidized Account/ Sole Proprietorship Company Managed AccountJhello SabinoNo ratings yet
- Al Ain Mall-Permit To Work Application: Ref: AAM/ EHSMS/ Form-12, Rev-3 Permit No (For Office Use Only)Document1 pageAl Ain Mall-Permit To Work Application: Ref: AAM/ EHSMS/ Form-12, Rev-3 Permit No (For Office Use Only)Veterano 1968No ratings yet
- City of Taguig: Business Permit Application FormDocument2 pagesCity of Taguig: Business Permit Application Formjane calipayNo ratings yet
- Customer Feedback FormDocument6 pagesCustomer Feedback FormSheila Marie Gil-VersozaNo ratings yet
- FSED 001 - Application Form FSECDocument1 pageFSED 001 - Application Form FSECMacabebe Fire StationNo ratings yet
- Zoning Use Registration Permit ApplicationDocument2 pagesZoning Use Registration Permit ApplicationgarbagepatchNo ratings yet
- CMS10124Document1 pageCMS10124naabNo ratings yet
- Service Request FormDocument2 pagesService Request FormPrasenjit PanditNo ratings yet
- Overtime Form: The Belt and Road Sinobridge (Philippines) International Economic and Talents Cooperation Center IncDocument1 pageOvertime Form: The Belt and Road Sinobridge (Philippines) International Economic and Talents Cooperation Center IncShiela CasayuranNo ratings yet
- Noc of BikeDocument5 pagesNoc of BikeShaikh din mohammed100% (1)
- 001 Desierto HvacDocument1 page001 Desierto Hvacjessaviernes25No ratings yet
- Extra Time Allowance FormDocument3 pagesExtra Time Allowance Form4rgfbfrgbyNo ratings yet
- Maintenance Report FormDocument1 pageMaintenance Report Formmrjfilling san luisNo ratings yet
- ENDORSEMENT ZurichDocument1 pageENDORSEMENT ZurichAmirul Zainal AbidinNo ratings yet
- Account Maintenance FormDocument1 pageAccount Maintenance FormVin CentNo ratings yet
- Limay Power Plant: San Miguel GroupDocument1 pageLimay Power Plant: San Miguel Grouppepenapao1217No ratings yet
- PGMA Employee Clearance FormDocument1 pagePGMA Employee Clearance FormChai dionesNo ratings yet
- Application Form For Business Permit: AmendmentDocument2 pagesApplication Form For Business Permit: AmendmentPatbing-sooNo ratings yet
- Fortress Iphone 11 Promax 256gbDocument1 pageFortress Iphone 11 Promax 256gbDéblocage icloud & Google 225No ratings yet
- Netcorp. TimesheetDocument4 pagesNetcorp. TimesheetRizal LeonardoNo ratings yet
- CLP Termination of Account Eng 20091022Document1 pageCLP Termination of Account Eng 20091022健康生活園Healthy Life GardenNo ratings yet
- Tax Declaration Application & Routing Form: Date Filed: Control No.Document1 pageTax Declaration Application & Routing Form: Date Filed: Control No.christina loNo ratings yet
- Credit Terms Application Full With Corrections Broken LineDocument1 pageCredit Terms Application Full With Corrections Broken LineJedidia Mae DueñasNo ratings yet
- Move in NoticeDocument1 pageMove in NoticeminaNo ratings yet
- SG Renewal FormDocument4 pagesSG Renewal FormJon SantiagoNo ratings yet
- Form XDocument2 pagesForm XKarthik75% (8)
- Cebuana FormDocument1 pageCebuana FormAshe RokimNo ratings yet
- Request Form For Change in Portfolio Information: Re-Invest Provide Cash OR OR Issue Bonus Units Encash Bonus UnitsDocument1 pageRequest Form For Change in Portfolio Information: Re-Invest Provide Cash OR OR Issue Bonus Units Encash Bonus UnitsMuhammad Noman MahmoodNo ratings yet
- GPMC Standard Form - Move in Clearance VFeb032021Document1 pageGPMC Standard Form - Move in Clearance VFeb032021Jlj ChuaNo ratings yet
- Himachal Pradesh Licensing Board Application Form For Renewal of Electrical Contractor License "Class-A"Document6 pagesHimachal Pradesh Licensing Board Application Form For Renewal of Electrical Contractor License "Class-A"Sri SabariNo ratings yet
- PDO-Locational ClearanceDocument1 pagePDO-Locational ClearanceTimothy John DicheNo ratings yet
- APP Form Mabuhay AccommodationDocument3 pagesAPP Form Mabuhay AccommodationJhelen De LeonNo ratings yet
- Warranty Claim Form: Engine BrakesDocument1 pageWarranty Claim Form: Engine BrakesJoseGarzaNo ratings yet
- Mega Project Assurance: Volume One - The Terminological DictionaryFrom EverandMega Project Assurance: Volume One - The Terminological DictionaryNo ratings yet


























































Download as pdf or txt
You might also like
- 2019 Business Credit with no Personal Guarantee: Get over 200K in Business Credit without using your SSNFrom Everand2019 Business Credit with no Personal Guarantee: Get over 200K in Business Credit without using your SSNRating: 4.5 out of 5 stars4.5/5 (3)
- Clearance Form - Employee Turn-Over ChecklistDocument2 pagesClearance Form - Employee Turn-Over Checklistjurex salomonNo ratings yet
- 57984c89bf389 (BPI CAP) Account Opening Form and Client Agreement 04-06-2016Document15 pages57984c89bf389 (BPI CAP) Account Opening Form and Client Agreement 04-06-2016Nancy Hernandez- TurlaNo ratings yet
- Application Form: Republic of The PhilippinesDocument3 pagesApplication Form: Republic of The PhilippinesAllan Diel CaranguianNo ratings yet
- 0T Form - GP ArmanDocument1 page0T Form - GP ArmanshaiNo ratings yet
- 0T Form - GP AnthonyDocument1 page0T Form - GP AnthonyshaiNo ratings yet
- Official Business Information Control Sheet: UrgentDocument3 pagesOfficial Business Information Control Sheet: UrgentnehllajacintoNo ratings yet
- Occupancy TemporaryDocument4 pagesOccupancy TemporaryVicente Ali Diaz SanchezNo ratings yet
- ZIMRA - Internal Funds Transfer FormDocument1 pageZIMRA - Internal Funds Transfer FormSimbarashe Mugoni0% (1)
- Field Service Report: Beckman Coulter India Pvt. Ltd. No.: DateDocument1 pageField Service Report: Beckman Coulter India Pvt. Ltd. No.: DateBrahmananda ChakrabortyNo ratings yet
- Clearance Form (CF)Document1 pageClearance Form (CF)kimberly magallanesNo ratings yet
- Oimb Citizens Charter 10 04 Cor 12 DealerDocument1 pageOimb Citizens Charter 10 04 Cor 12 DealerMuhammad Hasher AnjalinNo ratings yet
- Edeclaration of Source Funds FormDocument2 pagesEdeclaration of Source Funds FormRaymond WilliamsNo ratings yet
- Software Service CallDocument1 pageSoftware Service CallPawan RaiNo ratings yet
- Type of Application: New Renewal Application/Control No: Mode of Release: Pick-Up MailDocument2 pagesType of Application: New Renewal Application/Control No: Mode of Release: Pick-Up MailSheanaNo ratings yet
- Definition of TermsDocument4 pagesDefinition of TermsTopher ReyesNo ratings yet
- Ot Request FormDocument1 pageOt Request Formjoehanz.hrdNo ratings yet
- Republic of The Philippines Department of Transportation and Communications STCW OfficeDocument1 pageRepublic of The Philippines Department of Transportation and Communications STCW OfficeHeralynn BaloloyNo ratings yet
- Client Clearance Form (CCF)Document1 pageClient Clearance Form (CCF)kimberly magallanesNo ratings yet
- Reimbursement FormDocument1 pageReimbursement FormcampNo ratings yet
- Kori Engineering Credit Application FormDocument6 pagesKori Engineering Credit Application Formaj.ngadaNo ratings yet
- Type of Application: New Renewal Application/Control No: Mode of Release: Pick-Up MailDocument1 pageType of Application: New Renewal Application/Control No: Mode of Release: Pick-Up MailMuhammad Hasher AnjalinNo ratings yet
- SLF103 ApplicationRefundExcessSTLAmortization V06Document1 pageSLF103 ApplicationRefundExcessSTLAmortization V06Ina Marie BalajadiaNo ratings yet
- ClearanceDocument5 pagesClearancelouise matsuiNo ratings yet
- Business Permit FormDocument2 pagesBusiness Permit FormNicole De VillaNo ratings yet
- Company Subsidized Account/ Sole Proprietorship Company Managed AccountDocument1 pageCompany Subsidized Account/ Sole Proprietorship Company Managed AccountJhello SabinoNo ratings yet
- Al Ain Mall-Permit To Work Application: Ref: AAM/ EHSMS/ Form-12, Rev-3 Permit No (For Office Use Only)Document1 pageAl Ain Mall-Permit To Work Application: Ref: AAM/ EHSMS/ Form-12, Rev-3 Permit No (For Office Use Only)Veterano 1968No ratings yet
- City of Taguig: Business Permit Application FormDocument2 pagesCity of Taguig: Business Permit Application Formjane calipayNo ratings yet
- Customer Feedback FormDocument6 pagesCustomer Feedback FormSheila Marie Gil-VersozaNo ratings yet
- FSED 001 - Application Form FSECDocument1 pageFSED 001 - Application Form FSECMacabebe Fire StationNo ratings yet
- Zoning Use Registration Permit ApplicationDocument2 pagesZoning Use Registration Permit ApplicationgarbagepatchNo ratings yet
- CMS10124Document1 pageCMS10124naabNo ratings yet
- Service Request FormDocument2 pagesService Request FormPrasenjit PanditNo ratings yet
- Overtime Form: The Belt and Road Sinobridge (Philippines) International Economic and Talents Cooperation Center IncDocument1 pageOvertime Form: The Belt and Road Sinobridge (Philippines) International Economic and Talents Cooperation Center IncShiela CasayuranNo ratings yet
- Noc of BikeDocument5 pagesNoc of BikeShaikh din mohammed100% (1)
- 001 Desierto HvacDocument1 page001 Desierto Hvacjessaviernes25No ratings yet
- Extra Time Allowance FormDocument3 pagesExtra Time Allowance Form4rgfbfrgbyNo ratings yet
- Maintenance Report FormDocument1 pageMaintenance Report Formmrjfilling san luisNo ratings yet
- ENDORSEMENT ZurichDocument1 pageENDORSEMENT ZurichAmirul Zainal AbidinNo ratings yet
- Account Maintenance FormDocument1 pageAccount Maintenance FormVin CentNo ratings yet
- Limay Power Plant: San Miguel GroupDocument1 pageLimay Power Plant: San Miguel Grouppepenapao1217No ratings yet
- PGMA Employee Clearance FormDocument1 pagePGMA Employee Clearance FormChai dionesNo ratings yet
- Application Form For Business Permit: AmendmentDocument2 pagesApplication Form For Business Permit: AmendmentPatbing-sooNo ratings yet
- Fortress Iphone 11 Promax 256gbDocument1 pageFortress Iphone 11 Promax 256gbDéblocage icloud & Google 225No ratings yet
- Netcorp. TimesheetDocument4 pagesNetcorp. TimesheetRizal LeonardoNo ratings yet
- CLP Termination of Account Eng 20091022Document1 pageCLP Termination of Account Eng 20091022健康生活園Healthy Life GardenNo ratings yet
- Tax Declaration Application & Routing Form: Date Filed: Control No.Document1 pageTax Declaration Application & Routing Form: Date Filed: Control No.christina loNo ratings yet
- Credit Terms Application Full With Corrections Broken LineDocument1 pageCredit Terms Application Full With Corrections Broken LineJedidia Mae DueñasNo ratings yet
- Move in NoticeDocument1 pageMove in NoticeminaNo ratings yet
- SG Renewal FormDocument4 pagesSG Renewal FormJon SantiagoNo ratings yet
- Form XDocument2 pagesForm XKarthik75% (8)
- Cebuana FormDocument1 pageCebuana FormAshe RokimNo ratings yet
- Request Form For Change in Portfolio Information: Re-Invest Provide Cash OR OR Issue Bonus Units Encash Bonus UnitsDocument1 pageRequest Form For Change in Portfolio Information: Re-Invest Provide Cash OR OR Issue Bonus Units Encash Bonus UnitsMuhammad Noman MahmoodNo ratings yet
- GPMC Standard Form - Move in Clearance VFeb032021Document1 pageGPMC Standard Form - Move in Clearance VFeb032021Jlj ChuaNo ratings yet
- Himachal Pradesh Licensing Board Application Form For Renewal of Electrical Contractor License "Class-A"Document6 pagesHimachal Pradesh Licensing Board Application Form For Renewal of Electrical Contractor License "Class-A"Sri SabariNo ratings yet
- PDO-Locational ClearanceDocument1 pagePDO-Locational ClearanceTimothy John DicheNo ratings yet
- APP Form Mabuhay AccommodationDocument3 pagesAPP Form Mabuhay AccommodationJhelen De LeonNo ratings yet
- Warranty Claim Form: Engine BrakesDocument1 pageWarranty Claim Form: Engine BrakesJoseGarzaNo ratings yet
- Mega Project Assurance: Volume One - The Terminological DictionaryFrom EverandMega Project Assurance: Volume One - The Terminological DictionaryNo ratings yet