Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- All Mcqs of CHNDocument115 pagesAll Mcqs of CHNumar khan94% (47)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Mirizzi Syndrome - UpToDateDocument15 pagesMirizzi Syndrome - UpToDateEdgar Miguel ContrerasNo ratings yet
- Facial DivergenceDocument11 pagesFacial DivergencemelovebeingmeNo ratings yet
- Orthodontic Study Models: 5 Year Lec. No.5 بياغ نيسح لاضن ةروتكلاDocument7 pagesOrthodontic Study Models: 5 Year Lec. No.5 بياغ نيسح لاضن ةروتكلاmelovebeingmeNo ratings yet
- Unit 5: Breach of Contract and Its Remedies: Learning OutcomesDocument10 pagesUnit 5: Breach of Contract and Its Remedies: Learning Outcomesmelovebeingme100% (1)
- Strict LiabilityDocument12 pagesStrict LiabilitymelovebeingmeNo ratings yet
- Indian Contract Act 1872Document15 pagesIndian Contract Act 1872melovebeingme0% (1)
- Remedies For Breach ContractsDocument13 pagesRemedies For Breach ContractsmelovebeingmeNo ratings yet
- Summary of Workshop On Injunction PDFDocument29 pagesSummary of Workshop On Injunction PDFmelovebeingmeNo ratings yet
- Constitution of India and Judicial ReviewDocument32 pagesConstitution of India and Judicial ReviewmelovebeingmeNo ratings yet
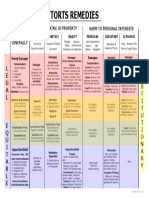
- Torts Remedies PDFDocument1 pageTorts Remedies PDFmelovebeingme100% (1)
- Right To PrivacyDocument6 pagesRight To PrivacymelovebeingmeNo ratings yet
- Applicability of Pont's Index in OrthodonticsDocument5 pagesApplicability of Pont's Index in OrthodonticsmelovebeingmeNo ratings yet
- Material Safety Data SheetDocument14 pagesMaterial Safety Data SheetmelovebeingmeNo ratings yet
- KUHS ActDocument78 pagesKUHS ActmelovebeingmeNo ratings yet
- Foodborne Diseases in Malaysia A ReviewDocument8 pagesFoodborne Diseases in Malaysia A Reviewma_e_harunNo ratings yet
- First Aid ArrangementsDocument5 pagesFirst Aid ArrangementsrjavillarNo ratings yet
- Sleep Study InterpretationDocument4 pagesSleep Study InterpretationgreenNo ratings yet
- Coronavirus (COVID-19) RecordsDocument3 pagesCoronavirus (COVID-19) Recordsrodolpho pizysieznigNo ratings yet
- Hospital Management System Project ReportDocument5 pagesHospital Management System Project Reportgagaggadedede gagagagaNo ratings yet
- Terra To GensDocument4 pagesTerra To GensKaye Niale BaleteNo ratings yet
- Diare: Arlinda Silva Prameswari 201810401011044Document28 pagesDiare: Arlinda Silva Prameswari 201810401011044Lilian Rahma AnandaNo ratings yet
- Career Paths Nursing SBDocument12 pagesCareer Paths Nursing SBAy ManNo ratings yet
- CMRF Form TelanaganaDocument1 pageCMRF Form Telanaganasrisai onlinecenter100% (3)
- HPA Maldives PDFDocument93 pagesHPA Maldives PDFshifanahmedNo ratings yet
- Cardiology 2023 FinalDocument208 pagesCardiology 2023 FinalBelinda ELISHA100% (1)
- ZYVOX - Stability of Linezolid IV Under Various ConditionsDocument2 pagesZYVOX - Stability of Linezolid IV Under Various ConditionsLauren BluhmNo ratings yet
- Evidence-Based Nursing: The 5 Steps of EBNDocument13 pagesEvidence-Based Nursing: The 5 Steps of EBNRanjith RgtNo ratings yet
- AstaReal CardioDocument2 pagesAstaReal CardioAmy HtunNo ratings yet
- Resume-Vandalyn Collins Mcgrue Msn4Document7 pagesResume-Vandalyn Collins Mcgrue Msn4Anonymous UEQPru0aNo ratings yet
- Maternal and Child Health Nursing Care of The Childbearing and Childrearing Family Pillitteri 6th Edition Test BankDocument4 pagesMaternal and Child Health Nursing Care of The Childbearing and Childrearing Family Pillitteri 6th Edition Test BankMark Bureau100% (39)
- Future Directions For NursingDocument8 pagesFuture Directions For NursingJennifer DixonNo ratings yet
- ESC - 2021 - The Growing Role of Genetics in The Understanding of Cardiovascular Diseases - Towards Personalized MedicineDocument5 pagesESC - 2021 - The Growing Role of Genetics in The Understanding of Cardiovascular Diseases - Towards Personalized MedicineDini SuhardiniNo ratings yet
- Antistax® Fresh Leg Gel: PSA Code of Ethics ReviewDocument3 pagesAntistax® Fresh Leg Gel: PSA Code of Ethics ReviewpharmacydailyNo ratings yet
- SOP For Campus Management in COVID-19Document18 pagesSOP For Campus Management in COVID-19srihari krishNo ratings yet
- Colostomy & Colostomy CareDocument56 pagesColostomy & Colostomy Careapi-3722454100% (31)
- Tally Sheet (Check Sheet) : TemplateDocument7 pagesTally Sheet (Check Sheet) : TemplateHomero NavarroNo ratings yet
- On Fetal MeasureDocument40 pagesOn Fetal MeasureHarish Labana100% (2)
- Intussusception Pedia ReportDocument13 pagesIntussusception Pedia ReportJesselyn HeruelaNo ratings yet
- Management of Cardiac Disease in PregnancyDocument10 pagesManagement of Cardiac Disease in PregnancyUtsav ShettyNo ratings yet
- Test Bank For Basic Medical Language 4th Edition Lafleur DownloadDocument13 pagesTest Bank For Basic Medical Language 4th Edition Lafleur Downloadantoniowagnercrqampebwt100% (34)
- A 5-Year-Old With Fever, Headache, Neck Stiffness, and Leg PainDocument7 pagesA 5-Year-Old With Fever, Headache, Neck Stiffness, and Leg PainKarma AkiraNo ratings yet
- CertificatesDocument12 pagesCertificatesArpana BhattaraiNo ratings yet