
Change Control Form
Change Control Form
You might also like
- AS9100 Rev D Internal Audit ChecklistDocument3 pagesAS9100 Rev D Internal Audit ChecklistAmR El SHeNaWy67% (3)
- Concept of Entrepreneur, EntrepreneurshipDocument6 pagesConcept of Entrepreneur, EntrepreneurshipMAHENDRA SHIVAJI DHENAK93% (151)
- Quality Control ManualDocument78 pagesQuality Control ManualRajeshSekar100% (3)
- Annex K - Final Completion Inspection ReportDocument1 pageAnnex K - Final Completion Inspection ReportRo Ma SantaNo ratings yet
- APQP ChecklistDocument18 pagesAPQP ChecklistmichaelbarkovicNo ratings yet
- IQA Audit ChecklistDocument26 pagesIQA Audit Checklistnorlie100% (1)
- QualityPlan FPSO TopsideDocument36 pagesQualityPlan FPSO Topsidedndudc100% (4)
- 145 Manual ChecklistDocument4 pages145 Manual ChecklistElLoko MartinesNo ratings yet
- SOP For Change Control - Pharmaceutical GuidelinesDocument4 pagesSOP For Change Control - Pharmaceutical Guidelinesmanspa2014No ratings yet
- Centinela Flot Column Quality Plan WVendor AuditDocument15 pagesCentinela Flot Column Quality Plan WVendor AuditAndrés RodríguezNo ratings yet
- SUF PR 14 Quality AuditingDocument8 pagesSUF PR 14 Quality Auditingscriptd_ozd3nNo ratings yet
- Format 10 - Part Submission Warrant1Document2 pagesFormat 10 - Part Submission Warrant1vijayNo ratings yet
- Honour Lab Limited (Unit-V)Document6 pagesHonour Lab Limited (Unit-V)Krishna Kishore MalladiNo ratings yet
- Supplier Pre-Assessment Questionnairevendor Evaluation Form: Document No. Revision 0Document12 pagesSupplier Pre-Assessment Questionnairevendor Evaluation Form: Document No. Revision 0Priyank Srivastava100% (2)
- SampleqamanualDocument16 pagesSampleqamanualHamdiNo ratings yet
- 10 CFR 21 Potential Defect ChecklistDocument6 pages10 CFR 21 Potential Defect ChecklistCharles Bill Eldredge100% (1)
- FM-NM-014 ECN - NoticeDocument1 pageFM-NM-014 ECN - Noticephutthawongdanchai041215No ratings yet
- Construction Managers Manual - Mar2021Document183 pagesConstruction Managers Manual - Mar2021Miguel EspinosaNo ratings yet
- DE-QC-RFI-F01 (RFI or Testing Form)Document1 pageDE-QC-RFI-F01 (RFI or Testing Form)Zainarul Aswad RazaliNo ratings yet
- CBIM 2021 Form B-09 - Final Inspection Report For Flood ControlDocument2 pagesCBIM 2021 Form B-09 - Final Inspection Report For Flood ControlMessy Rose Rafales-CamachoNo ratings yet
- Gap Analysis Checklist: WWW - Iso-9001-Checklist - Co.ukDocument6 pagesGap Analysis Checklist: WWW - Iso-9001-Checklist - Co.ukKhizzar IshaqueNo ratings yet
- DE-QC-RIT-F01 (RFI or Testing Form)Document1 pageDE-QC-RIT-F01 (RFI or Testing Form)Zainarul Aswad RazaliNo ratings yet
- Manual Quality Management System en 72626Document31 pagesManual Quality Management System en 72626Stephen Koko100% (1)
- Milestone Achievement Report Guidelines and Form A. PurposeDocument3 pagesMilestone Achievement Report Guidelines and Form A. PurposeMUNAS XVI FoSSEINo ratings yet
- Filled AS9100 Sample StandardDocument30 pagesFilled AS9100 Sample Standardxq2y6j5kj5No ratings yet
- ISO 9001:2015 and ISO 13485:2016: Quality Management Systems DocumentationDocument21 pagesISO 9001:2015 and ISO 13485:2016: Quality Management Systems Documentationisrael afolayan mayomiNo ratings yet
- Metal Detector Deviation ReportDocument1 pageMetal Detector Deviation ReportEtta JeneeNo ratings yet
- V-101946-0511-0280 Rev.1 - Pintado de Paredes y Piso PulidoDocument13 pagesV-101946-0511-0280 Rev.1 - Pintado de Paredes y Piso PulidoJoseph LizarragaNo ratings yet
- CAS090503QAQCPlan PDFDocument20 pagesCAS090503QAQCPlan PDFvyly1723No ratings yet
- Quality Manual - Ac PlasticsDocument36 pagesQuality Manual - Ac PlasticsMETAQUIMNo ratings yet
- 2016 QMS Quality Manual Sample PDFDocument3 pages2016 QMS Quality Manual Sample PDFMohini MaratheNo ratings yet
- BCB 201Document22 pagesBCB 201Rajesh Kumar100% (2)
- ISO 9001 Application FormDocument4 pagesISO 9001 Application FormchinitnNo ratings yet
- CAO - IRI Part - MDocument102 pagesCAO - IRI Part - MDariush ShNo ratings yet
- Final Commissioning PlanDocument1 pageFinal Commissioning PlanHumaid ShaikhNo ratings yet
- QM-001 QMS-Quality ManualDocument13 pagesQM-001 QMS-Quality ManualFERNANDO MORANTESNo ratings yet
- 01 - Internal Audit Report - SecurityDocument9 pages01 - Internal Audit Report - SecurityVincent OngNo ratings yet
- Bahrain Ministry of Works - Construction ProjectsDocument11 pagesBahrain Ministry of Works - Construction ProjectsMohammad YaseenNo ratings yet
- Report of Magnetic-Particle Examination of WeldsDocument1 pageReport of Magnetic-Particle Examination of WeldsSathish KumarNo ratings yet
- Screening Questionnaire Rev. 08Document11 pagesScreening Questionnaire Rev. 08emekaNo ratings yet
- Supplier Evaluation Questionnaire Rev1Document2 pagesSupplier Evaluation Questionnaire Rev1dixon stapleton100% (1)
- Assessment Readiness Review Checklist ISO/IEC 17025:2017Document3 pagesAssessment Readiness Review Checklist ISO/IEC 17025:2017Sarah Jane BroñolaNo ratings yet
- Final Commissioning ReportDocument1 pageFinal Commissioning ReportHumaid Shaikh100% (3)
- EG For Testing and Commissioning v5 FinalDocument27 pagesEG For Testing and Commissioning v5 FinalPacoNo ratings yet
- MT Report FormDocument1 pageMT Report FormAmit HasanNo ratings yet
- 000-ZA-E-02600, Project Quality Plan, Rev.EDocument44 pages000-ZA-E-02600, Project Quality Plan, Rev.Eengmaar201037No ratings yet
- Cast-In-Situ Bored Piling Works by ConventionalMethod1Document11 pagesCast-In-Situ Bored Piling Works by ConventionalMethod1jitendraNo ratings yet
- Req Change Impact AnalysisDocument1 pageReq Change Impact AnalysisVipin RanaNo ratings yet
- CAV2000 PQ ChecklistDocument2 pagesCAV2000 PQ Checklistcamtu.cao17No ratings yet
- Sample Report of Magnetic-Particle Examination of WeldsDocument1 pageSample Report of Magnetic-Particle Examination of WeldsNavanitheeshwaran SivasubramaniyamNo ratings yet
- QA QC Manual 2008Document86 pagesQA QC Manual 2008netomeller100% (2)
- Add 51 XFDocument119 pagesAdd 51 XFMagedNo ratings yet
- Contractor QC Plan Template PDFDocument31 pagesContractor QC Plan Template PDFAmit HuidromNo ratings yet
- FINAL INSPECTION REPORT (For Buildings) : CBIM Form B-10Document4 pagesFINAL INSPECTION REPORT (For Buildings) : CBIM Form B-10Abdurauf SawadjaanNo ratings yet
- Complete Business Blueprint4Document670 pagesComplete Business Blueprint4Egwuma EfoNo ratings yet
- Part Process M FG ChangeDocument2 pagesPart Process M FG ChangeGeovanny HernándezNo ratings yet
- AS9100 Rev C - Transition Plan: Step 1Document10 pagesAS9100 Rev C - Transition Plan: Step 1Ganeshkumar Krishna ShettyNo ratings yet
- Quality Manual: Tech Circuits, IncDocument25 pagesQuality Manual: Tech Circuits, IncSiva B PositiveNo ratings yet
- V-101946-0511-0281 Rev.0 - Colocacion de Porcelanato en Piso y ZocalosDocument14 pagesV-101946-0511-0281 Rev.0 - Colocacion de Porcelanato en Piso y ZocalosJoseph LizarragaNo ratings yet
- R.C. Beam / Slab Inspection ChecklistDocument1 pageR.C. Beam / Slab Inspection Checklistctlim88No ratings yet
- Case Study-1Document2 pagesCase Study-1Youtube VideoNo ratings yet
- Case Study-2Document2 pagesCase Study-2Youtube VideoNo ratings yet
- Case Study-3Document2 pagesCase Study-3Youtube VideoNo ratings yet
- OOS FormDocument3 pagesOOS FormYoutube VideoNo ratings yet
- New Employee Induction Traininng Feedback FormDocument1 pageNew Employee Induction Traininng Feedback FormYoutube VideoNo ratings yet
- BTMM Patterns and Setups1Document12 pagesBTMM Patterns and Setups1Tafara Michael100% (1)
- Capitals Book 2 FGHIJ Instructions and WorksheetsDocument15 pagesCapitals Book 2 FGHIJ Instructions and WorksheetsMelanyNo ratings yet
- Tutorial MSDocument4 pagesTutorial MSVidhya NairNo ratings yet
- Cattleya Tent Events: Event Planning BusinessDocument8 pagesCattleya Tent Events: Event Planning BusinessRobert StefanNo ratings yet
- Aquativeplus Ac/Dc: Actuator Valve (Solenoid) Converting Electric To Hydraulic CommandDocument4 pagesAquativeplus Ac/Dc: Actuator Valve (Solenoid) Converting Electric To Hydraulic CommandErnesto Jimenez RodriguezNo ratings yet
- 395-Article Text-1362-2-10-20220720Document13 pages395-Article Text-1362-2-10-20220720PipingNo ratings yet
- © 2007 Thomson South-WesternDocument31 pages© 2007 Thomson South-WesternKatharine PrasetyoNo ratings yet
- Managerial Accounting 16th Edition Garrison Solutions Manual 1Document36 pagesManagerial Accounting 16th Edition Garrison Solutions Manual 1codyhines04081997tja100% (36)
- Ent 300Document13 pagesEnt 300Fawwaz ZawawiNo ratings yet
- Knotted Fence Tata WironDocument4 pagesKnotted Fence Tata WironvdrizzilsNo ratings yet
- Lembar Kerja AkuntansiDocument75 pagesLembar Kerja AkuntansifaiqNo ratings yet
- Swarovski Components Collection 2023 LowResDocument450 pagesSwarovski Components Collection 2023 LowResjuliabalbi01No ratings yet
- Ficha Técnica - RPS Tyco ElectronicsDocument2 pagesFicha Técnica - RPS Tyco ElectronicsGalindo FivigaorNo ratings yet
- Tutorial Exercise IIDocument2 pagesTutorial Exercise IILemma MuletaNo ratings yet
- Joe Grad Has Just Arrived at The Big U HeDocument2 pagesJoe Grad Has Just Arrived at The Big U Hetrilocksp SinghNo ratings yet
- Solutions Consolidation-FormattedDocument22 pagesSolutions Consolidation-FormattedShehrozSTNo ratings yet
- Floor InletDocument2 pagesFloor Inletmauro zarateNo ratings yet
- Mirc ElectronicsDocument9 pagesMirc Electronicsanand310No ratings yet
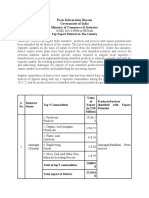
- District Wise Exports of India - 2021Document13 pagesDistrict Wise Exports of India - 2021MNo ratings yet
- CDCS Case StudyDocument4 pagesCDCS Case StudyPangoea Pangoea100% (1)
- Consumer and Producer Theory - Falvio ToxvaerdDocument188 pagesConsumer and Producer Theory - Falvio ToxvaerdNimra AhmedNo ratings yet
- As Distributor Locator Asia Pacific v7Document5 pagesAs Distributor Locator Asia Pacific v7michel trevezNo ratings yet
- An Approach To Determine The Health Index of Power TransformersDocument5 pagesAn Approach To Determine The Health Index of Power Transformersbaby MaNo ratings yet
- Optigenex v. Jeunesse Global Holdings Et. Al.Document57 pagesOptigenex v. Jeunesse Global Holdings Et. Al.PriorSmartNo ratings yet
- Mergent Residences Sample ComputationDocument1 pageMergent Residences Sample Computationrx5426.homerouterNo ratings yet
- Sol. Man. - Chapter 7 - Posting To The LedgerDocument7 pagesSol. Man. - Chapter 7 - Posting To The LedgerMae Ann Tomimbang MaglinteNo ratings yet
- HR/ Management GamesDocument39 pagesHR/ Management Gameskamdica100% (6)
- GeM Bidding 3988940Document4 pagesGeM Bidding 3988940Anmol JainNo ratings yet
- (English (Auto-Generated) ) 04 - Drilling Economics and The AFE - FLV (DownSub - Com)Document5 pages(English (Auto-Generated) ) 04 - Drilling Economics and The AFE - FLV (DownSub - Com)Nasser JNo ratings yet




























































































Download as docx, pdf, or txt
You might also like
- AS9100 Rev D Internal Audit ChecklistDocument3 pagesAS9100 Rev D Internal Audit ChecklistAmR El SHeNaWy67% (3)
- Concept of Entrepreneur, EntrepreneurshipDocument6 pagesConcept of Entrepreneur, EntrepreneurshipMAHENDRA SHIVAJI DHENAK93% (151)
- Quality Control ManualDocument78 pagesQuality Control ManualRajeshSekar100% (3)
- Annex K - Final Completion Inspection ReportDocument1 pageAnnex K - Final Completion Inspection ReportRo Ma SantaNo ratings yet
- APQP ChecklistDocument18 pagesAPQP ChecklistmichaelbarkovicNo ratings yet
- IQA Audit ChecklistDocument26 pagesIQA Audit Checklistnorlie100% (1)
- QualityPlan FPSO TopsideDocument36 pagesQualityPlan FPSO Topsidedndudc100% (4)
- 145 Manual ChecklistDocument4 pages145 Manual ChecklistElLoko MartinesNo ratings yet
- SOP For Change Control - Pharmaceutical GuidelinesDocument4 pagesSOP For Change Control - Pharmaceutical Guidelinesmanspa2014No ratings yet
- Centinela Flot Column Quality Plan WVendor AuditDocument15 pagesCentinela Flot Column Quality Plan WVendor AuditAndrés RodríguezNo ratings yet
- SUF PR 14 Quality AuditingDocument8 pagesSUF PR 14 Quality Auditingscriptd_ozd3nNo ratings yet
- Format 10 - Part Submission Warrant1Document2 pagesFormat 10 - Part Submission Warrant1vijayNo ratings yet
- Honour Lab Limited (Unit-V)Document6 pagesHonour Lab Limited (Unit-V)Krishna Kishore MalladiNo ratings yet
- Supplier Pre-Assessment Questionnairevendor Evaluation Form: Document No. Revision 0Document12 pagesSupplier Pre-Assessment Questionnairevendor Evaluation Form: Document No. Revision 0Priyank Srivastava100% (2)
- SampleqamanualDocument16 pagesSampleqamanualHamdiNo ratings yet
- 10 CFR 21 Potential Defect ChecklistDocument6 pages10 CFR 21 Potential Defect ChecklistCharles Bill Eldredge100% (1)
- FM-NM-014 ECN - NoticeDocument1 pageFM-NM-014 ECN - Noticephutthawongdanchai041215No ratings yet
- Construction Managers Manual - Mar2021Document183 pagesConstruction Managers Manual - Mar2021Miguel EspinosaNo ratings yet
- DE-QC-RFI-F01 (RFI or Testing Form)Document1 pageDE-QC-RFI-F01 (RFI or Testing Form)Zainarul Aswad RazaliNo ratings yet
- CBIM 2021 Form B-09 - Final Inspection Report For Flood ControlDocument2 pagesCBIM 2021 Form B-09 - Final Inspection Report For Flood ControlMessy Rose Rafales-CamachoNo ratings yet
- Gap Analysis Checklist: WWW - Iso-9001-Checklist - Co.ukDocument6 pagesGap Analysis Checklist: WWW - Iso-9001-Checklist - Co.ukKhizzar IshaqueNo ratings yet
- DE-QC-RIT-F01 (RFI or Testing Form)Document1 pageDE-QC-RIT-F01 (RFI or Testing Form)Zainarul Aswad RazaliNo ratings yet
- Manual Quality Management System en 72626Document31 pagesManual Quality Management System en 72626Stephen Koko100% (1)
- Milestone Achievement Report Guidelines and Form A. PurposeDocument3 pagesMilestone Achievement Report Guidelines and Form A. PurposeMUNAS XVI FoSSEINo ratings yet
- Filled AS9100 Sample StandardDocument30 pagesFilled AS9100 Sample Standardxq2y6j5kj5No ratings yet
- ISO 9001:2015 and ISO 13485:2016: Quality Management Systems DocumentationDocument21 pagesISO 9001:2015 and ISO 13485:2016: Quality Management Systems Documentationisrael afolayan mayomiNo ratings yet
- Metal Detector Deviation ReportDocument1 pageMetal Detector Deviation ReportEtta JeneeNo ratings yet
- V-101946-0511-0280 Rev.1 - Pintado de Paredes y Piso PulidoDocument13 pagesV-101946-0511-0280 Rev.1 - Pintado de Paredes y Piso PulidoJoseph LizarragaNo ratings yet
- CAS090503QAQCPlan PDFDocument20 pagesCAS090503QAQCPlan PDFvyly1723No ratings yet
- Quality Manual - Ac PlasticsDocument36 pagesQuality Manual - Ac PlasticsMETAQUIMNo ratings yet
- 2016 QMS Quality Manual Sample PDFDocument3 pages2016 QMS Quality Manual Sample PDFMohini MaratheNo ratings yet
- BCB 201Document22 pagesBCB 201Rajesh Kumar100% (2)
- ISO 9001 Application FormDocument4 pagesISO 9001 Application FormchinitnNo ratings yet
- CAO - IRI Part - MDocument102 pagesCAO - IRI Part - MDariush ShNo ratings yet
- Final Commissioning PlanDocument1 pageFinal Commissioning PlanHumaid ShaikhNo ratings yet
- QM-001 QMS-Quality ManualDocument13 pagesQM-001 QMS-Quality ManualFERNANDO MORANTESNo ratings yet
- 01 - Internal Audit Report - SecurityDocument9 pages01 - Internal Audit Report - SecurityVincent OngNo ratings yet
- Bahrain Ministry of Works - Construction ProjectsDocument11 pagesBahrain Ministry of Works - Construction ProjectsMohammad YaseenNo ratings yet
- Report of Magnetic-Particle Examination of WeldsDocument1 pageReport of Magnetic-Particle Examination of WeldsSathish KumarNo ratings yet
- Screening Questionnaire Rev. 08Document11 pagesScreening Questionnaire Rev. 08emekaNo ratings yet
- Supplier Evaluation Questionnaire Rev1Document2 pagesSupplier Evaluation Questionnaire Rev1dixon stapleton100% (1)
- Assessment Readiness Review Checklist ISO/IEC 17025:2017Document3 pagesAssessment Readiness Review Checklist ISO/IEC 17025:2017Sarah Jane BroñolaNo ratings yet
- Final Commissioning ReportDocument1 pageFinal Commissioning ReportHumaid Shaikh100% (3)
- EG For Testing and Commissioning v5 FinalDocument27 pagesEG For Testing and Commissioning v5 FinalPacoNo ratings yet
- MT Report FormDocument1 pageMT Report FormAmit HasanNo ratings yet
- 000-ZA-E-02600, Project Quality Plan, Rev.EDocument44 pages000-ZA-E-02600, Project Quality Plan, Rev.Eengmaar201037No ratings yet
- Cast-In-Situ Bored Piling Works by ConventionalMethod1Document11 pagesCast-In-Situ Bored Piling Works by ConventionalMethod1jitendraNo ratings yet
- Req Change Impact AnalysisDocument1 pageReq Change Impact AnalysisVipin RanaNo ratings yet
- CAV2000 PQ ChecklistDocument2 pagesCAV2000 PQ Checklistcamtu.cao17No ratings yet
- Sample Report of Magnetic-Particle Examination of WeldsDocument1 pageSample Report of Magnetic-Particle Examination of WeldsNavanitheeshwaran SivasubramaniyamNo ratings yet
- QA QC Manual 2008Document86 pagesQA QC Manual 2008netomeller100% (2)
- Add 51 XFDocument119 pagesAdd 51 XFMagedNo ratings yet
- Contractor QC Plan Template PDFDocument31 pagesContractor QC Plan Template PDFAmit HuidromNo ratings yet
- FINAL INSPECTION REPORT (For Buildings) : CBIM Form B-10Document4 pagesFINAL INSPECTION REPORT (For Buildings) : CBIM Form B-10Abdurauf SawadjaanNo ratings yet
- Complete Business Blueprint4Document670 pagesComplete Business Blueprint4Egwuma EfoNo ratings yet
- Part Process M FG ChangeDocument2 pagesPart Process M FG ChangeGeovanny HernándezNo ratings yet
- AS9100 Rev C - Transition Plan: Step 1Document10 pagesAS9100 Rev C - Transition Plan: Step 1Ganeshkumar Krishna ShettyNo ratings yet
- Quality Manual: Tech Circuits, IncDocument25 pagesQuality Manual: Tech Circuits, IncSiva B PositiveNo ratings yet
- V-101946-0511-0281 Rev.0 - Colocacion de Porcelanato en Piso y ZocalosDocument14 pagesV-101946-0511-0281 Rev.0 - Colocacion de Porcelanato en Piso y ZocalosJoseph LizarragaNo ratings yet
- R.C. Beam / Slab Inspection ChecklistDocument1 pageR.C. Beam / Slab Inspection Checklistctlim88No ratings yet
- Case Study-1Document2 pagesCase Study-1Youtube VideoNo ratings yet
- Case Study-2Document2 pagesCase Study-2Youtube VideoNo ratings yet
- Case Study-3Document2 pagesCase Study-3Youtube VideoNo ratings yet
- OOS FormDocument3 pagesOOS FormYoutube VideoNo ratings yet
- New Employee Induction Traininng Feedback FormDocument1 pageNew Employee Induction Traininng Feedback FormYoutube VideoNo ratings yet
- BTMM Patterns and Setups1Document12 pagesBTMM Patterns and Setups1Tafara Michael100% (1)
- Capitals Book 2 FGHIJ Instructions and WorksheetsDocument15 pagesCapitals Book 2 FGHIJ Instructions and WorksheetsMelanyNo ratings yet
- Tutorial MSDocument4 pagesTutorial MSVidhya NairNo ratings yet
- Cattleya Tent Events: Event Planning BusinessDocument8 pagesCattleya Tent Events: Event Planning BusinessRobert StefanNo ratings yet
- Aquativeplus Ac/Dc: Actuator Valve (Solenoid) Converting Electric To Hydraulic CommandDocument4 pagesAquativeplus Ac/Dc: Actuator Valve (Solenoid) Converting Electric To Hydraulic CommandErnesto Jimenez RodriguezNo ratings yet
- 395-Article Text-1362-2-10-20220720Document13 pages395-Article Text-1362-2-10-20220720PipingNo ratings yet
- © 2007 Thomson South-WesternDocument31 pages© 2007 Thomson South-WesternKatharine PrasetyoNo ratings yet
- Managerial Accounting 16th Edition Garrison Solutions Manual 1Document36 pagesManagerial Accounting 16th Edition Garrison Solutions Manual 1codyhines04081997tja100% (36)
- Ent 300Document13 pagesEnt 300Fawwaz ZawawiNo ratings yet
- Knotted Fence Tata WironDocument4 pagesKnotted Fence Tata WironvdrizzilsNo ratings yet
- Lembar Kerja AkuntansiDocument75 pagesLembar Kerja AkuntansifaiqNo ratings yet
- Swarovski Components Collection 2023 LowResDocument450 pagesSwarovski Components Collection 2023 LowResjuliabalbi01No ratings yet
- Ficha Técnica - RPS Tyco ElectronicsDocument2 pagesFicha Técnica - RPS Tyco ElectronicsGalindo FivigaorNo ratings yet
- Tutorial Exercise IIDocument2 pagesTutorial Exercise IILemma MuletaNo ratings yet
- Joe Grad Has Just Arrived at The Big U HeDocument2 pagesJoe Grad Has Just Arrived at The Big U Hetrilocksp SinghNo ratings yet
- Solutions Consolidation-FormattedDocument22 pagesSolutions Consolidation-FormattedShehrozSTNo ratings yet
- Floor InletDocument2 pagesFloor Inletmauro zarateNo ratings yet
- Mirc ElectronicsDocument9 pagesMirc Electronicsanand310No ratings yet
- District Wise Exports of India - 2021Document13 pagesDistrict Wise Exports of India - 2021MNo ratings yet
- CDCS Case StudyDocument4 pagesCDCS Case StudyPangoea Pangoea100% (1)
- Consumer and Producer Theory - Falvio ToxvaerdDocument188 pagesConsumer and Producer Theory - Falvio ToxvaerdNimra AhmedNo ratings yet
- As Distributor Locator Asia Pacific v7Document5 pagesAs Distributor Locator Asia Pacific v7michel trevezNo ratings yet
- An Approach To Determine The Health Index of Power TransformersDocument5 pagesAn Approach To Determine The Health Index of Power Transformersbaby MaNo ratings yet
- Optigenex v. Jeunesse Global Holdings Et. Al.Document57 pagesOptigenex v. Jeunesse Global Holdings Et. Al.PriorSmartNo ratings yet
- Mergent Residences Sample ComputationDocument1 pageMergent Residences Sample Computationrx5426.homerouterNo ratings yet
- Sol. Man. - Chapter 7 - Posting To The LedgerDocument7 pagesSol. Man. - Chapter 7 - Posting To The LedgerMae Ann Tomimbang MaglinteNo ratings yet
- HR/ Management GamesDocument39 pagesHR/ Management Gameskamdica100% (6)
- GeM Bidding 3988940Document4 pagesGeM Bidding 3988940Anmol JainNo ratings yet
- (English (Auto-Generated) ) 04 - Drilling Economics and The AFE - FLV (DownSub - Com)Document5 pages(English (Auto-Generated) ) 04 - Drilling Economics and The AFE - FLV (DownSub - Com)Nasser JNo ratings yet