Download as pdf or txt
You might also like
- A Case Presentation On Multinodular GoitreDocument27 pagesA Case Presentation On Multinodular Goitrecnsatish86% (7)
- Spare Parts Catalog: 4 WG 160 Material Number: 4656.054.039 Current Date: 10.06.2020Document70 pagesSpare Parts Catalog: 4 WG 160 Material Number: 4656.054.039 Current Date: 10.06.2020Romuald Pogorzelczyk100% (2)
- 0a27thyroid Function TestDocument35 pages0a27thyroid Function TestAshokvardhan Chowdary Nandigam67% (3)
- Mayuri Thyroid MTDocument24 pagesMayuri Thyroid MTmayuri zanwarNo ratings yet
- Thyroid Disorders (Final Draft)Document17 pagesThyroid Disorders (Final Draft)mogesie1995No ratings yet
- Thyroid Disease (Chan)Document29 pagesThyroid Disease (Chan)Sidiq AboobakerNo ratings yet
- Plenary Week 1 LO No 1Document25 pagesPlenary Week 1 LO No 1Nur Faydotus SalsabilaNo ratings yet
- Thyroid Disease: Sejal Nirban FY1Document30 pagesThyroid Disease: Sejal Nirban FY1Ahmed AbedoNo ratings yet
- Thyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistDocument30 pagesThyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistNurul HikmaNo ratings yet
- THYROIDDocument191 pagesTHYROIDTonie AbabonNo ratings yet
- ThyrotoxicosisDocument105 pagesThyrotoxicosisAli Murtaza Abbas100% (1)
- Thyroid Function Test and Adrenal Function TestsDocument64 pagesThyroid Function Test and Adrenal Function TestsDr Abhinav Manish MDNo ratings yet
- Thyroid Function Tests PPT of IMS BHUDocument74 pagesThyroid Function Tests PPT of IMS BHUPriyanshu Mandal100% (1)
- Approach To HyperthyroidismDocument58 pagesApproach To HyperthyroidismmedqehkkNo ratings yet
- Hypothalamus Pituitary Thyroid AxisDocument15 pagesHypothalamus Pituitary Thyroid AxisEdmari Joy Pojas MontilNo ratings yet
- KrishnaDocument24 pagesKrishnaimchhapriNo ratings yet
- Tutorial On Goiter GadedDocument117 pagesTutorial On Goiter GadedhindabdalgadirNo ratings yet
- Thyroid ReportDocument105 pagesThyroid ReportAARVNo ratings yet
- Zak Notes Hypothyroidism (Juma)Document34 pagesZak Notes Hypothyroidism (Juma)82cxp4n46wNo ratings yet
- Thyroid DiseaseDocument72 pagesThyroid Diseaseluna zeidNo ratings yet
- HipertiroidDocument37 pagesHipertiroidTaysqy swftNo ratings yet
- Lecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Document21 pagesLecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Ivan AditamaNo ratings yet
- Clinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmDocument73 pagesClinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmdiniNo ratings yet
- Kuliah Hyper and Hypothyroid - 2014Document66 pagesKuliah Hyper and Hypothyroid - 2014Clararida RiawanNo ratings yet
- Thyroid GlandDocument127 pagesThyroid GlandCarla Mae MoraNo ratings yet
- F1) P-Thyroid DisordersDocument9 pagesF1) P-Thyroid Disordersstella.gillesania.chenNo ratings yet
- Anesthetic Consideration in Thyroid SurgeryDocument36 pagesAnesthetic Consideration in Thyroid Surgerymaulina13No ratings yet
- Thyroid GlandDocument10 pagesThyroid GlandSheena Mae Atienza100% (2)
- Thyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsDocument7 pagesThyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsPrincess Noreen SavellanoNo ratings yet
- HipertiroidDocument62 pagesHipertiroidMiftahuljjanah BaharuddinNo ratings yet
- Thyroid Function Test: The "Hidden" Health ProblemDocument34 pagesThyroid Function Test: The "Hidden" Health Problemvjanand07100% (1)
- Thyroid Function TestDocument21 pagesThyroid Function TestPat JacintoNo ratings yet
- HyperthyroidismDocument24 pagesHyperthyroidismelaine grace arataNo ratings yet
- Thyroiddisorders PDFDocument51 pagesThyroiddisorders PDFIslam ShoukryNo ratings yet
- What Is The Thyroid?Document12 pagesWhat Is The Thyroid?Silvia ValentinaNo ratings yet
- Endocrine System - Internal MedicineDocument39 pagesEndocrine System - Internal MedicineDaanishNo ratings yet
- Thyroid Function TestsDocument29 pagesThyroid Function TestsAkwesaNo ratings yet
- Hyperthyroid 170715182805Document71 pagesHyperthyroid 170715182805Suryati HusinNo ratings yet
- Thyroid Gland An Diseases of Thyroid D Gland: Omc LectureDocument59 pagesThyroid Gland An Diseases of Thyroid D Gland: Omc LectureEdward MakemboNo ratings yet
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- Hipertiroid 2022 UnhaluDocument59 pagesHipertiroid 2022 Unhaluramadhanadlansyah7No ratings yet
- Thyroid Function Tests and Goitre SV 24-4-21Document51 pagesThyroid Function Tests and Goitre SV 24-4-21Lal KhanNo ratings yet
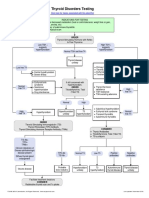
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperNo ratings yet
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmMuhamad Suriansyah100% (1)
- Thyroid Disorders TBL Pathology Learning MaterialDocument20 pagesThyroid Disorders TBL Pathology Learning MaterialIrdina SyabilNo ratings yet
- Neck Diseases: Affiliated Hospital Of Jining Medical Colledge Dep.Mammary And Thyroid Surgery Zhu Kunbing 朱坤兵Document61 pagesNeck Diseases: Affiliated Hospital Of Jining Medical Colledge Dep.Mammary And Thyroid Surgery Zhu Kunbing 朱坤兵sanjivdasNo ratings yet
- PSGS Review 2015Document230 pagesPSGS Review 2015yassercarlomanNo ratings yet
- 3.thyroid Hormones and DisordersDocument46 pages3.thyroid Hormones and DisorderssinayupeNo ratings yet
- Hypo and Hyperthyroidism 2023Document113 pagesHypo and Hyperthyroidism 2023Cristina Georgiana SerbanNo ratings yet
- Pemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKDocument16 pagesPemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKZulfan RifqiawanNo ratings yet
- Hyper and HypothyroidDocument139 pagesHyper and HypothyroidRaka ZaelaniNo ratings yet
- Thyroid Function TestDocument28 pagesThyroid Function TestDhinesh Muthusamy100% (1)
- Thyroid Function Tests: Drneha Mahajan MD PathologyDocument71 pagesThyroid Function Tests: Drneha Mahajan MD PathologyMukesh Kumar ChaudharyNo ratings yet
- Thyrotoxicosis & Hypothyroidism by Prof DR NK ChopraDocument52 pagesThyrotoxicosis & Hypothyroidism by Prof DR NK ChopraAbdulsalam DostNo ratings yet
- Thyroiddisease 190216062020Document42 pagesThyroiddisease 190216062020Manikandan Vp100% (1)
- Hiper Dan Hipotiroid (Revisi)Document76 pagesHiper Dan Hipotiroid (Revisi)AgusNo ratings yet
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmkatNo ratings yet
- Thyroid GlandDocument44 pagesThyroid GlandMuhammad MakkiNo ratings yet
- HypertyroidismDocument46 pagesHypertyroidismenriNo ratings yet
- Sophie Keyte Bvms (Hons) Mvetmed (Dist) Fhea Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkDocument24 pagesSophie Keyte Bvms (Hons) Mvetmed (Dist) Fhea Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkStefana UrsuNo ratings yet
- Customer Request Form: Name of Fleet ManagerDocument2 pagesCustomer Request Form: Name of Fleet Managerdink flipNo ratings yet
- Helloween - Victim of FateDocument10 pagesHelloween - Victim of FateWillson Isaac Barrueta BarruetaNo ratings yet
- Ged 101 Activity 4Document2 pagesGed 101 Activity 4Ranzel CruzatNo ratings yet
- TS90 B 2009Document813 pagesTS90 B 2009Yulius PurnamaNo ratings yet
- Adoption of Digital Marketing For Start UpsDocument50 pagesAdoption of Digital Marketing For Start UpsPraveen PandeyNo ratings yet
- Quantum User ManualDocument220 pagesQuantum User ManualRoshi_11No ratings yet
- INTERCHANGE 2 - QUIZ UNITS 11 & 12 - Revisión Del IntentoDocument6 pagesINTERCHANGE 2 - QUIZ UNITS 11 & 12 - Revisión Del IntentoJOSE TANGARIFENo ratings yet
- AINES en ERC 2020Document9 pagesAINES en ERC 2020Cesar Augusto Restrepo ValenciaNo ratings yet
- Investment Centers and Transfer PricingDocument53 pagesInvestment Centers and Transfer PricingArlene DacpanoNo ratings yet
- Iphone 6S Plus Schematic - Vietmobile - VNDocument62 pagesIphone 6S Plus Schematic - Vietmobile - VNMiguel Angel Aguilar Moreira75% (4)
- DT200 Bluewave2 Operators GuideDocument8 pagesDT200 Bluewave2 Operators GuidemodatNo ratings yet
- 03711002219-Taj Mahal HotelDocument87 pages03711002219-Taj Mahal HotelPradeep PandeyNo ratings yet
- NEC - 2017-10-26 - High Frequency TradingDocument53 pagesNEC - 2017-10-26 - High Frequency TradingAlexander GloyNo ratings yet
- Ttester Eng111kDocument103 pagesTtester Eng111kVipin PurohitNo ratings yet
- Wargames Illustrated #017Document60 pagesWargames Illustrated #017Анатолий Золотухин100% (3)
- SATIP S 070 02 Irrigation PipingDocument2 pagesSATIP S 070 02 Irrigation PipingMuhammad Farukh ManzoorNo ratings yet
- The Morals of Measurement: Accuracy, Irony, and Trust in Late Victorian Electrical PracticeDocument20 pagesThe Morals of Measurement: Accuracy, Irony, and Trust in Late Victorian Electrical PracticeMAROUANE AbdelkaderNo ratings yet
- Valerie Reuben v. US Airways Inc, 3rd Cir. (2012)Document5 pagesValerie Reuben v. US Airways Inc, 3rd Cir. (2012)Scribd Government DocsNo ratings yet
- Seismic Waves AnalysisDocument6 pagesSeismic Waves Analysisbabu1434No ratings yet
- CD Unit 1Document489 pagesCD Unit 1Apoorva VHNo ratings yet
- TRIP Moving South Carolina Forward Report September 2021Document21 pagesTRIP Moving South Carolina Forward Report September 2021WMBF NewsNo ratings yet
- Fuelling Active Kids Fuelling Active Kids: Junior Soccer PlayerDocument23 pagesFuelling Active Kids Fuelling Active Kids: Junior Soccer PlayerAdhith PhysioNo ratings yet
- Appendix C: Time Value of MoneyDocument15 pagesAppendix C: Time Value of MoneyRabie HarounNo ratings yet
- Tesco Pet Insurance Claim FormDocument2 pagesTesco Pet Insurance Claim FormrosielavisNo ratings yet
- Reclaim Feeders BrochureDocument8 pagesReclaim Feeders Brochureelsieazcuna024No ratings yet
- Obstetric HemorrhageDocument104 pagesObstetric HemorrhageRanjit SharmaNo ratings yet
- Ola S1 Pro Owner'S ManualDocument58 pagesOla S1 Pro Owner'S ManualAtul Goyal100% (1)
- CDCA 2203 Ram & RomDocument11 pagesCDCA 2203 Ram & RomMUHAMAD AMMAR SYAFIQ BIN MAD ZIN STUDENTNo ratings yet
- AtrazineDocument22 pagesAtrazineapi-257409369No ratings yet