Download as docx, pdf, or txt
You might also like
- A Dominant's PledgeDocument2 pagesA Dominant's PledgeTalon Bloodrayn100% (8)
- TLE Hairdressing Grade 8 - 9Document25 pagesTLE Hairdressing Grade 8 - 9Roswlle50% (2)
- NCP 3rd YearDocument6 pagesNCP 3rd YearTotoro AblogNo ratings yet
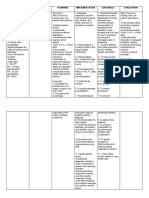
- Nursing Care Plan Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Outcome Criteria Actual EvaluationDocument4 pagesNursing Care Plan Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Outcome Criteria Actual EvaluationPabhat Kumar75% (4)
- NCP Pleural EffusionDocument7 pagesNCP Pleural EffusionKristian Karl Bautista Kiw-isNo ratings yet
- Pharmacology for Student and Pupil Nurses and Student Pharmacy TechniciansFrom EverandPharmacology for Student and Pupil Nurses and Student Pharmacy TechniciansNo ratings yet
- Neuroanatomy Through Clinical Cases, 2E PDFDocument3 pagesNeuroanatomy Through Clinical Cases, 2E PDFjwongggg55140% (6)
- HYPERTHERMIADocument3 pagesHYPERTHERMIAjacobprince0016No ratings yet
- Pae Clinical Case Week 8Document10 pagesPae Clinical Case Week 8ScribdTranslationsNo ratings yet
- Subjective: Diarrhea Related To Watery Short Term: IndependentDocument4 pagesSubjective: Diarrhea Related To Watery Short Term: IndependentEmma Lyn SantosNo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataDocument2 pagesAssessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataCheila CruzNo ratings yet
- NCP PTBDocument4 pagesNCP PTBbryan matiasNo ratings yet
- MS Soapie #1Document2 pagesMS Soapie #1Fatima KateNo ratings yet
- HydroceleDocument10 pagesHydroceleRyan ReNo ratings yet
- NPR Deficient FluidDocument4 pagesNPR Deficient FluidDj KurtNo ratings yet
- NCP Platil Picu 3Document2 pagesNCP Platil Picu 3elmer.platiljrNo ratings yet
- FHP - NCP - Kidney FailureDocument9 pagesFHP - NCP - Kidney FailureFrancis AdrianNo ratings yet
- Nursing Care Management: Assessment Diagnosis Goals and Objective Intervention and Rationale EvaluationDocument3 pagesNursing Care Management: Assessment Diagnosis Goals and Objective Intervention and Rationale EvaluationTyron ChuaNo ratings yet
- Dengue Hemorrhagic FeverDocument19 pagesDengue Hemorrhagic FeverChristian James MataNo ratings yet
- Epp Rahma Arifah PutriDocument11 pagesEpp Rahma Arifah PutriRahmaarifahputri2701No ratings yet
- NCPDocument3 pagesNCPNicole_Santos_6836No ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- NCP - Activity Intolerance & Excess Fluid VolumeDocument2 pagesNCP - Activity Intolerance & Excess Fluid VolumeCindy MariscotesNo ratings yet
- MalariaDocument3 pagesMalariasuciNo ratings yet
- Fluid Volume Deficit Related To Loose Watery Stool Diarrhea)Document2 pagesFluid Volume Deficit Related To Loose Watery Stool Diarrhea)Jesse James Advincula Edjec100% (15)
- Jade R. Dinolan BSN-4 Case Study On A Patient With Pulmonary TuberculosisDocument8 pagesJade R. Dinolan BSN-4 Case Study On A Patient With Pulmonary TuberculosisJhade RelletaNo ratings yet
- Nursing Care Plan:: Lopez, Maria Sofia B. 10/18/2020 3-BSN-B Prof. IsananDocument4 pagesNursing Care Plan:: Lopez, Maria Sofia B. 10/18/2020 3-BSN-B Prof. IsananSofia LopezNo ratings yet
- PNEUMONIADocument8 pagesPNEUMONIARica ParcasioNo ratings yet
- NCP Deficient Fluid VolumeDocument3 pagesNCP Deficient Fluid VolumeDoneva Lyn MedinaNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanAnnahNo ratings yet
- Assesment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssesment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- Nursing Care PlansDocument31 pagesNursing Care PlansCyril Jane Caanyagan AcutNo ratings yet
- NCP of Fever and HypertensionDocument2 pagesNCP of Fever and HypertensionDayan CabrigaNo ratings yet
- Gestational Diabetes - Case Study 2Document13 pagesGestational Diabetes - Case Study 2Bb RabbitNo ratings yet
- Tuberculosis Nursing Care Plan Ineffective Airway Clearance PDFDocument2 pagesTuberculosis Nursing Care Plan Ineffective Airway Clearance PDFPratiksha AmbedkarNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Short Term: Independent: Independent: Short TermDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Short Term: Independent: Independent: Short TermDYNA GISELLE ROMERONo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Planning Implementation Rationale EvaluationChloie Marie RosalejosNo ratings yet
- Herpes NCPDocument3 pagesHerpes NCPSanny L Asim Jr.No ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJobelyn TunayNo ratings yet
- Community Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientDocument4 pagesCommunity Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientKrisianne Mae Lorenzo Francisco100% (1)
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument3 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceMelinda Cariño BallonNo ratings yet
- Nursing Care Plan: Assessment: Nursing Diagnosis: Nursing Goal: Nursing Intervention: Rationale: EvaluationDocument6 pagesNursing Care Plan: Assessment: Nursing Diagnosis: Nursing Goal: Nursing Intervention: Rationale: Evaluationeliza luisNo ratings yet
- NCP PcapDocument2 pagesNCP PcapKenj Pereña100% (1)
- NCP PneumoniaDocument6 pagesNCP PneumoniaMerliah LofrancoNo ratings yet
- NCP 3Document2 pagesNCP 3FitzLucario QueNo ratings yet
- Luckkhan Nursing PlanDocument3 pagesLuckkhan Nursing PlanAsifiwe MwaikamboNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanRachelleNo ratings yet
- Viernes, Jericho NCP CimcDocument2 pagesViernes, Jericho NCP CimcJayson Respicio jr.No ratings yet
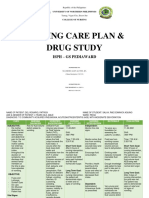
- Salva, R.D NCP & Drug Study (Isph - Gs Pediaward)Document7 pagesSalva, R.D NCP & Drug Study (Isph - Gs Pediaward)Rae Dominick Aquino SalvaNo ratings yet
- NCP Pneumonia May6 Ate KimDocument2 pagesNCP Pneumonia May6 Ate Kimiransevilla615No ratings yet
- Subjective: Short Term: Independent: - Monitored On Blood Pressure Short TermDocument1 pageSubjective: Short Term: Independent: - Monitored On Blood Pressure Short TermShane Shaira G PantaleonNo ratings yet
- Course in The Ward FinallllllllDocument6 pagesCourse in The Ward FinallllllllJisel-Apple BulanNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Planning Intervention Rationale EvaluationPam RomeroNo ratings yet
- Hypovolemic Shock Sample NCPDocument14 pagesHypovolemic Shock Sample NCPRENEROSE TORRES100% (1)
- Assessment Nursing Diagnosis Planning Interventions EvaluationsDocument3 pagesAssessment Nursing Diagnosis Planning Interventions EvaluationsAjay SupanNo ratings yet
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Subjective Short Term IndependentDocument3 pagesAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Subjective Short Term IndependentMoi Valdoz100% (1)
- Gastroenteritis NCPDocument1 pageGastroenteritis NCPVenus Bactol67% (3)
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Burns NCPDocument8 pagesBurns NCPJM AsentistaNo ratings yet
- Pulmonary HypertensionDocument10 pagesPulmonary HypertensionqingwenNo ratings yet
- NCP Ineffective Airway ClearanceDocument8 pagesNCP Ineffective Airway Clearance1adie1907No ratings yet
- Pharmacology for Student and Pupil Nurses and Students in Associated ProfessionsFrom EverandPharmacology for Student and Pupil Nurses and Students in Associated ProfessionsNo ratings yet
- Rizal-Mabuuhay-Ka Grand FinalistDocument2 pagesRizal-Mabuuhay-Ka Grand Finalistjacobprince0016No ratings yet
- Project Mark 1Document58 pagesProject Mark 1jacobprince0016No ratings yet
- Ghantt Chart Group 10Document1 pageGhantt Chart Group 10jacobprince0016No ratings yet
- Semi Finals CHAPTER IVDocument5 pagesSemi Finals CHAPTER IVjacobprince0016No ratings yet
- 4.1 The VetDocument7 pages4.1 The VetAtharva 74No ratings yet
- Dr. Ysr University of Health Sciences, Ap, Vijayawada - 08 College Wise Allotment List of MSC Nursing Courses, (Phase I), 2022-23Document6 pagesDr. Ysr University of Health Sciences, Ap, Vijayawada - 08 College Wise Allotment List of MSC Nursing Courses, (Phase I), 2022-23Pattem StellaNo ratings yet
- Early Recollections: A Humanistic Assessment in CounselingDocument7 pagesEarly Recollections: A Humanistic Assessment in CounselingDANAH MOGHRM ALSHEHRINo ratings yet
- NS Case2Document2 pagesNS Case2shivangi singhNo ratings yet
- Artículo Endo DR Johnn Benitez ValenciaDocument1 pageArtículo Endo DR Johnn Benitez ValenciaJohnnifer Benitez ValenciaNo ratings yet
- Food and Nutrition Coursework SampleDocument8 pagesFood and Nutrition Coursework Sampleydzkmgajd100% (2)
- Chapter 5-Eneman20Document5 pagesChapter 5-Eneman20Reynald John PastranaNo ratings yet
- TELEMEDICINEDocument2 pagesTELEMEDICINESILLA ELSA SOJINo ratings yet
- Dysfunctional FamiliesDocument2 pagesDysfunctional FamiliesJane JasaNo ratings yet
- Commonly Known As GuyabanoDocument2 pagesCommonly Known As Guyabanolongosalyssa930No ratings yet
- SCPX Project Line of Fire Presentation ENGDocument22 pagesSCPX Project Line of Fire Presentation ENGGiorgi KenkebashviliNo ratings yet
- Annotated Bibliography MindfulnessDocument14 pagesAnnotated Bibliography Mindfulnessapi-255289819No ratings yet
- Perdev - Module 9Document9 pagesPerdev - Module 9April Rose CortesNo ratings yet
- Lesson Plan in Science 10Document3 pagesLesson Plan in Science 10Phranxies Jean BlayaNo ratings yet
- VRV AcuDocument4 pagesVRV AcuNova CastyNo ratings yet
- Makalah Modul IV - Neuromuskular RMDocument47 pagesMakalah Modul IV - Neuromuskular RMStar WarNo ratings yet
- Continuing Medical Education Activity in Academic Emergency MedicineDocument10 pagesContinuing Medical Education Activity in Academic Emergency MedicinePacoNo ratings yet
- PE01 Handout AEROBIC EXERCISE FOR HEALTH FITNESSDocument2 pagesPE01 Handout AEROBIC EXERCISE FOR HEALTH FITNESSArthit MendozaNo ratings yet
- Parents of A Disabled ChildDocument37 pagesParents of A Disabled ChildSuman SharmaNo ratings yet
- Measuring Optimism in OrganizationsDocument23 pagesMeasuring Optimism in Organizationsmarcelocarvalhoteacher2373No ratings yet
- Drought As A Catalyst For Human Security ChallengesDocument6 pagesDrought As A Catalyst For Human Security ChallengesKrishnaveni PenkiNo ratings yet
- Philosophy StatementDocument1 pagePhilosophy Statementapi-583007789No ratings yet
- Vigan Demographic AnalysisDocument9 pagesVigan Demographic AnalysisAngel CebrerosNo ratings yet
- Spot Report 2 (DAVID)Document2 pagesSpot Report 2 (DAVID)kedtNo ratings yet
- WFHT Test Your Stress Iq Quiz Answer Key FinalDocument4 pagesWFHT Test Your Stress Iq Quiz Answer Key FinalHailey MallerieNo ratings yet
- Readworks Kinder - Take Care of Your TeethDocument4 pagesReadworks Kinder - Take Care of Your TeethPatricia Lei Agamata FamilaraNo ratings yet
- ALLEVYN GENTLE BORDER LITE Location GuideDocument2 pagesALLEVYN GENTLE BORDER LITE Location GuideKmj AvotriniainaNo ratings yet