Download as pdf or txt
You might also like
- Wound Assessment Chart PDFDocument4 pagesWound Assessment Chart PDFFivendra100% (1)
- By Mike Bayer: Best SelfDocument6 pagesBy Mike Bayer: Best SelfLîk ÍšläNo ratings yet
- Brain SyncDocument46 pagesBrain SyncPriox BangetzNo ratings yet
- Performance and Diagnostic Accuracy of A Urine-Based Human Papillomavirus Assay in A Referral PopulationDocument7 pagesPerformance and Diagnostic Accuracy of A Urine-Based Human Papillomavirus Assay in A Referral PopulationJose de PapadopoulosNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofIrena McLaughlinNo ratings yet
- Cervical Cancer Screening With Human Papillomavirus DNA and Cytology in JapanDocument7 pagesCervical Cancer Screening With Human Papillomavirus DNA and Cytology in Japandella kharisma putriNo ratings yet
- Roe 2018Document11 pagesRoe 2018mohamaed abbasNo ratings yet
- Pap SmearDocument8 pagesPap Smearvyvie89No ratings yet
- Abnormal Cervical Cytology in Women Eligible For IVFDocument5 pagesAbnormal Cervical Cytology in Women Eligible For IVFtavo823No ratings yet
- A5 PDFDocument15 pagesA5 PDFDr. Arvind YadavNo ratings yet
- Pap Smear Accuracy For The Diagnosis of Cervical Precancerous LesionsDocument5 pagesPap Smear Accuracy For The Diagnosis of Cervical Precancerous LesionsPahang Reforansa PutraNo ratings yet
- Analysis of The Determinants of Low Cervical CanceDocument8 pagesAnalysis of The Determinants of Low Cervical CanceMWANGINo ratings yet
- 407 PDFDocument4 pages407 PDFSrideviRaviNo ratings yet
- 12 Tobing2010Document5 pages12 Tobing2010RonaLd Jackson SinagaNo ratings yet
- Impact of Knowledge and AttituDocument23 pagesImpact of Knowledge and AttituAnis SolikahNo ratings yet
- CA CervixDocument54 pagesCA CervixsesiaNo ratings yet
- Cervical CADocument10 pagesCervical CAAby ShauNo ratings yet
- Peerj 05 3910Document13 pagesPeerj 05 3910Денис КрахоткинNo ratings yet
- Nejmoa 061760Document16 pagesNejmoa 061760nqchi180418No ratings yet
- Comparison of Anal HPV Natural History Among Men by Country of Residence Brazil, Mexico, and The United StatesDocument13 pagesComparison of Anal HPV Natural History Among Men by Country of Residence Brazil, Mexico, and The United StatesLlamencio Kolotikpilli LlamaNo ratings yet
- Jurnal Onko 2Document9 pagesJurnal Onko 2anon_118437533No ratings yet
- Cervicalcancerprevention: Immunization and Screening 2015Document9 pagesCervicalcancerprevention: Immunization and Screening 2015behanges71No ratings yet
- JWH 2008 1068Document8 pagesJWH 2008 1068Khaled Loua-M'sNo ratings yet
- HPV16 Sublineage Associations With Histology-Specific Cancer Risk Using HPV Whole-Genome Sequences in 3200 WomenDocument9 pagesHPV16 Sublineage Associations With Histology-Specific Cancer Risk Using HPV Whole-Genome Sequences in 3200 WomenQuyết Lê HữuNo ratings yet
- Understanding Female Patients' Knowledge, Attitudes, and Practices Regarding Cervical Cancer Screening at Comboni HospitalDocument11 pagesUnderstanding Female Patients' Knowledge, Attitudes, and Practices Regarding Cervical Cancer Screening at Comboni HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Pap IntroductionDocument390 pagesPap IntroductionAnish VeettiyankalNo ratings yet
- Cervical Cancer Awareness, Screening and Vaccination Among Female Nursing Students of University of GhanaDocument7 pagesCervical Cancer Awareness, Screening and Vaccination Among Female Nursing Students of University of GhanaIJAR JOURNALNo ratings yet
- Project Title High Risk HPV Genotyping in Patient With Clinically Suspected Precancerous and Cancerous Lesions of CervixDocument16 pagesProject Title High Risk HPV Genotyping in Patient With Clinically Suspected Precancerous and Cancerous Lesions of CervixEmam MursalinNo ratings yet
- Chlamydia Trachomatis Infection in Female Partners of Circumcised and Uncircumcised Adult MenDocument10 pagesChlamydia Trachomatis Infection in Female Partners of Circumcised and Uncircumcised Adult MenJuan Andre' MarquinezNo ratings yet
- Manuscript of Risk Factors For Cancer Cervix: An Analysis of 1000 CasesDocument4 pagesManuscript of Risk Factors For Cancer Cervix: An Analysis of 1000 CasesHerman FiraNo ratings yet
- P16 Expression and Recurrent Cervical Intraepithelial Neoplasia After Cryotherapy Among Women Living With HIVDocument7 pagesP16 Expression and Recurrent Cervical Intraepithelial Neoplasia After Cryotherapy Among Women Living With HIVdawam986142No ratings yet
- 1 s2.0 S0002937815014520 MainDocument6 pages1 s2.0 S0002937815014520 Mainilham wildanNo ratings yet
- Jurnal BVDocument3 pagesJurnal BVEnvhy WinaNo ratings yet
- PIIS2213398422000902Document7 pagesPIIS2213398422000902Manas BhatiaNo ratings yet
- Schiff Man 1993Document7 pagesSchiff Man 1993ema 274No ratings yet
- 2001 JLGTD. Correlating Papanicolaou Smear, Colposcopic Impression, and Biopsy Results From The Women S Interagency HIV StudyDocument7 pages2001 JLGTD. Correlating Papanicolaou Smear, Colposcopic Impression, and Biopsy Results From The Women S Interagency HIV StudyJoseTeodomiroQuispeRicciNo ratings yet
- Anal Cytology 2019Document7 pagesAnal Cytology 2019Cristina CostaNo ratings yet
- 23 FullDocument5 pages23 Fulljulio juarezNo ratings yet
- Effect of Cervicitis On Visual Inspection With Acetic AcidDocument5 pagesEffect of Cervicitis On Visual Inspection With Acetic AcidmonicamoniccNo ratings yet
- DownloadDocument11 pagesDownloadthairineNo ratings yet
- Human Papillomavirus Infection in Shenyang City, People's Republic of China: A Population-Based StudyDocument5 pagesHuman Papillomavirus Infection in Shenyang City, People's Republic of China: A Population-Based StudyyoggihermawanNo ratings yet
- High Risk HPVDocument6 pagesHigh Risk HPVjawaralopangNo ratings yet
- Articles: BackgroundDocument12 pagesArticles: BackgroundMilan JovicNo ratings yet
- Breast CA ScreeningDocument8 pagesBreast CA Screeningchristelm_1No ratings yet
- Ref 42 Principles of NIPTDocument9 pagesRef 42 Principles of NIPTKhải Nguyễn ThànhNo ratings yet
- Risk Factors For Cervical Cancer: Results From A Hospital-Based Case-Control StudyDocument7 pagesRisk Factors For Cervical Cancer: Results From A Hospital-Based Case-Control StudyIntania RosatiNo ratings yet
- RH Fs Risk FactorsDocument2 pagesRH Fs Risk FactorsfentroispNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Kanker Serviks Di Rumah Sakit Sardjito YogyakartaDocument9 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Kanker Serviks Di Rumah Sakit Sardjito Yogyakartaira hadnasariNo ratings yet
- Knowledge Regarding Cervical Cancer Among Married Women in Rural Telangana: A Cross Sectional StudyDocument5 pagesKnowledge Regarding Cervical Cancer Among Married Women in Rural Telangana: A Cross Sectional StudySrideviRaviNo ratings yet
- Cervical CancerDocument14 pagesCervical CancerAlejandra MurilloNo ratings yet
- Articulo 2 - El Microbiota Vaginal Se Asocia Con La Regresión de Neoplasia Intraepitelial CervicalDocument13 pagesArticulo 2 - El Microbiota Vaginal Se Asocia Con La Regresión de Neoplasia Intraepitelial CervicalLiliana Antonio RevueltaNo ratings yet
- 11 - Trichomonas, Candida, and Gardnerella in CervicalDocument6 pages11 - Trichomonas, Candida, and Gardnerella in CervicalRenan RodriguesNo ratings yet
- Waggoner 2003Document9 pagesWaggoner 2003behanges71No ratings yet
- DJP 367Document12 pagesDJP 367Bibup GhaziyahNo ratings yet
- Seminars in Oncology NursingDocument9 pagesSeminars in Oncology NursingangelitostorresitosNo ratings yet
- Association of High-Risk Cervical Human Papillomavirus With Demographic and Clinico - Pathological Features in Asymptomatic and Symptomatic WomenDocument4 pagesAssociation of High-Risk Cervical Human Papillomavirus With Demographic and Clinico - Pathological Features in Asymptomatic and Symptomatic WomenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Journal of Medical Virology (2013)Document9 pagesJournal of Medical Virology (2013)lorena mahechaNo ratings yet
- ACCP Cxca Screening 2011Document8 pagesACCP Cxca Screening 2011Lizeth López LeónNo ratings yet
- Condom Use Promotes Regression of Cervical Intraepithelial Neoplasia and Clearance of Human Papillomavirus: A Randomized Clinical TrialDocument6 pagesCondom Use Promotes Regression of Cervical Intraepithelial Neoplasia and Clearance of Human Papillomavirus: A Randomized Clinical TrialAdi ParamarthaNo ratings yet
- Bmjopen 2014 005828Document9 pagesBmjopen 2014 005828antidius johnNo ratings yet
- Mccarey 2011Document7 pagesMccarey 2011Ajup SafarudinNo ratings yet
- Lower Genital Tract Precancer: Colposcopy, Pathology and TreatmentFrom EverandLower Genital Tract Precancer: Colposcopy, Pathology and TreatmentNo ratings yet
- LUNGSDocument43 pagesLUNGSelliot kafumukacheNo ratings yet
- 2 DiaphragmDocument21 pages2 Diaphragmelliot kafumukacheNo ratings yet
- Infratemporal FossaDocument45 pagesInfratemporal Fossaelliot kafumukacheNo ratings yet
- GLUTEAL REGION (Autosaved)Document84 pagesGLUTEAL REGION (Autosaved)elliot kafumukacheNo ratings yet
- Bone TissueDocument41 pagesBone Tissueelliot kafumukacheNo ratings yet
- CARTILAGEDocument16 pagesCARTILAGEelliot kafumukacheNo ratings yet
- Muscle TissueDocument34 pagesMuscle Tissueelliot kafumukacheNo ratings yet
- Pons IDocument46 pagesPons Ielliot kafumukacheNo ratings yet
- BLOODDocument37 pagesBLOODelliot kafumukacheNo ratings yet
- First Summative Test in Physical EducationDocument2 pagesFirst Summative Test in Physical EducationDainielle Marie PascualNo ratings yet
- PADILLO GROUP BSN 3E CHAPTER 1 3 Sir Jes 3Document61 pagesPADILLO GROUP BSN 3E CHAPTER 1 3 Sir Jes 3juliancheryll77No ratings yet
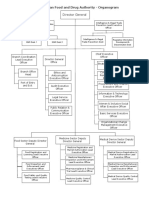
- EFDA Organogram English VersionDocument6 pagesEFDA Organogram English VersionRobsan YasinNo ratings yet
- Forensic Psychiatry and Prison Mental Health 2009Document32 pagesForensic Psychiatry and Prison Mental Health 2009Fiona Kumari Campbell100% (1)
- Philippine Health Insurance Corporation Circular No. 0035, S. 2013 - Implementing Guidelines On The Medical and Procedure Case RatesDocument17 pagesPhilippine Health Insurance Corporation Circular No. 0035, S. 2013 - Implementing Guidelines On The Medical and Procedure Case RatesChrysanthus HerreraNo ratings yet
- Hygienic Requirements of Food and Drink EstablishmentsDocument25 pagesHygienic Requirements of Food and Drink Establishmentssneh7335No ratings yet
- THEORIES COGNITIVE ForgetfulnessDocument4 pagesTHEORIES COGNITIVE ForgetfulnessGerÂld MuTaleNo ratings yet
- Set A: NP1 Nursing Board Exam December 2006 Answer Key 'Foundation of Professional Nursing PracticeDocument16 pagesSet A: NP1 Nursing Board Exam December 2006 Answer Key 'Foundation of Professional Nursing PracticeElizabella Henrietta TanaquilNo ratings yet
- Ot Guidelines ParkinsonDocument145 pagesOt Guidelines ParkinsonFanny100% (1)
- GHB FactsheetDocument2 pagesGHB FactsheetABC Action NewsNo ratings yet
- Case Presentation BY Dr. Prashanti Ophthalmology Ist YrDocument22 pagesCase Presentation BY Dr. Prashanti Ophthalmology Ist YrAyushman100% (3)
- PresentationDocument19 pagesPresentationSuryansh ThakkerNo ratings yet
- Utilizing The DSM-5 Anxious Distress Specifier To Develop Treatment Strategies For Patients With Major Depressive DisorderDocument12 pagesUtilizing The DSM-5 Anxious Distress Specifier To Develop Treatment Strategies For Patients With Major Depressive DisorderRosemarie FritschNo ratings yet
- Quality Standards For Urban Primary Health CentreDocument284 pagesQuality Standards For Urban Primary Health CentreGajendra TodakarNo ratings yet
- GDM Case StudyDocument5 pagesGDM Case Studydheeptha sundarNo ratings yet
- Recently Updated Trends in PsychologyDocument13 pagesRecently Updated Trends in PsychologyDulakshiNo ratings yet
- Poverty and Inequality Global Perspective (Autosaved)Document17 pagesPoverty and Inequality Global Perspective (Autosaved)Richlue GeegbaeNo ratings yet
- Dry Socket ManagementDocument7 pagesDry Socket ManagementNuzhat Noor AyeshaNo ratings yet
- Human Nutriation DraftDocument66 pagesHuman Nutriation DraftFahadNo ratings yet
- Case 1 Carilion ClinicDocument14 pagesCase 1 Carilion ClinicVikram KumarNo ratings yet
- Guidelines For Focused Bedside Nursing Care Plan Based On Nursing ProcessDocument10 pagesGuidelines For Focused Bedside Nursing Care Plan Based On Nursing Processamjad abdullah alzallalNo ratings yet
- BASC-2 Q Global Score Summary SampleDocument11 pagesBASC-2 Q Global Score Summary SamplegenacartaNo ratings yet
- NCP AnxietyDocument6 pagesNCP AnxietyRaijenne VersolaNo ratings yet
- Postpartum DepressionDocument1 pagePostpartum DepressionNirmala BhattNo ratings yet
- Midterm Psych Module 8Document10 pagesMidterm Psych Module 8Ladybelle GototosNo ratings yet
- ResumeDocument4 pagesResumeReynante C. ArellanoNo ratings yet
- NCP Sleeping PatternDocument2 pagesNCP Sleeping Patternastersisk1121No ratings yet