Download as pdf or txt
You might also like
- Science 3 DLP 1 - Sense Organs and Their FunctionsDocument16 pagesScience 3 DLP 1 - Sense Organs and Their FunctionsRussel Jane Sumonod - Maraguinot100% (3)
- Reconstruction of Defects of The Posterior Pinna.15Document4 pagesReconstruction of Defects of The Posterior Pinna.15cliffwinskyNo ratings yet
- CRANIAL Nerves - ExaminationDocument14 pagesCRANIAL Nerves - ExaminationMoussa FarhatNo ratings yet
- Le Fort III and Le Fort II OsteotomiesDocument11 pagesLe Fort III and Le Fort II OsteotomiesAndre Luis CostaNo ratings yet
- Free Flaps MaxillaDocument7 pagesFree Flaps MaxillaFahad QiamNo ratings yet
- Le Fort II Osteotomy and Modified Technique Presentation: Riginal RticleDocument6 pagesLe Fort II Osteotomy and Modified Technique Presentation: Riginal RticleSamuel SuazaNo ratings yet
- Maxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceDocument8 pagesMaxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceJuan Carlos CárcamoNo ratings yet
- Management of Firearm Facial Fractures at The Dr. José Eleuterio González'': University Hospital CaseDocument4 pagesManagement of Firearm Facial Fractures at The Dr. José Eleuterio González'': University Hospital CaseIndra D KristionoNo ratings yet
- Coronal Mentoplasty: Complementary Technique in Orthognathic Surgery: Cases ReportDocument5 pagesCoronal Mentoplasty: Complementary Technique in Orthognathic Surgery: Cases Reportmarco martinezNo ratings yet
- Class III Malocclusion SurgicaDocument9 pagesClass III Malocclusion Surgicaortodoncia 2022No ratings yet
- Modifieci R-Y-Zygoma Ti: Basis, andDocument9 pagesModifieci R-Y-Zygoma Ti: Basis, andSooraj SNo ratings yet
- +distraction Osteogenesis For The Cleftlip and PalateDocument12 pages+distraction Osteogenesis For The Cleftlip and PalategrisguzlNo ratings yet
- 2020 Article 265Document7 pages2020 Article 265Fabian BarretoNo ratings yet
- Osteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingDocument5 pagesOsteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingAnonymous Qt31LLO1lNo ratings yet
- Correction of Late Adolescent Skeletal Class III Using The Alt-RAMEC Protocol and Skeletal AnchorageDocument11 pagesCorrection of Late Adolescent Skeletal Class III Using The Alt-RAMEC Protocol and Skeletal AnchoragePorchiddioNo ratings yet
- Mixoma 9Document4 pagesMixoma 9Nicolás MedinaNo ratings yet
- Kansal 2011Document4 pagesKansal 2011Pushpraj ThakurNo ratings yet
- Bell 1977Document28 pagesBell 1977Reshma DeepakNo ratings yet
- 10 1016@j Ijom 2013 07 541Document1 page10 1016@j Ijom 2013 07 541leslie kalathilNo ratings yet
- Changes in Facial Form Relative To Progressive Atrophy of The Edentulous JawsDocument7 pagesChanges in Facial Form Relative To Progressive Atrophy of The Edentulous JawsshraddhaNo ratings yet
- HFM Free Flap Versus Fat GraftingDocument10 pagesHFM Free Flap Versus Fat GraftingNelson LowNo ratings yet
- Monobloc and Facial Bipartition OsteotomiesDocument18 pagesMonobloc and Facial Bipartition OsteotomiesKim SalahNo ratings yet
- MBCB 180031Document5 pagesMBCB 180031derkha SajNo ratings yet
- Park 2012Document6 pagesPark 2012Yassin SalahNo ratings yet
- Miniplaca para MAA en AdultoDocument10 pagesMiniplaca para MAA en AdultocdentistacesarmNo ratings yet
- Scientific Dental Journal: Bimaxillary Orthognathic Surgery in Skeletal Class III MalocclusionDocument7 pagesScientific Dental Journal: Bimaxillary Orthognathic Surgery in Skeletal Class III Malocclusionyuni madjidNo ratings yet
- Open Reduction and Internal Fixation of Palatal Fractures Using Three-Dimensional PlatesDocument5 pagesOpen Reduction and Internal Fixation of Palatal Fractures Using Three-Dimensional PlatesNachiketa parikhNo ratings yet
- Hindquarter IJOCDocument4 pagesHindquarter IJOCRyanAdnaniNo ratings yet
- Ajodo 3Document10 pagesAjodo 3ayisNo ratings yet
- Frontolateral Partial LaryngectomyDocument7 pagesFrontolateral Partial LaryngectomyJeremy HermantoNo ratings yet
- OSRM ProximalDocument9 pagesOSRM ProximalÂngelo Rosso LlantadaNo ratings yet
- Delir 2013Document7 pagesDelir 2013Karam EidNo ratings yet
- Abordaje Intraoral Reconstruccion Mandibular Bianchi2008Document3 pagesAbordaje Intraoral Reconstruccion Mandibular Bianchi2008Marcela GNo ratings yet
- Case Report: Total Lower Eyelid Reconstruction With A Prefabricated Flap Using Auricular CartilageDocument7 pagesCase Report: Total Lower Eyelid Reconstruction With A Prefabricated Flap Using Auricular CartilageFaisal HameedNo ratings yet
- Baumann 2001Document5 pagesBaumann 2001Sowmya ManthaNo ratings yet
- Pectoralis Major Myocutaneous F Lap: Eric R. Carlson, DMD, MDDocument11 pagesPectoralis Major Myocutaneous F Lap: Eric R. Carlson, DMD, MDlaljadeff12No ratings yet
- Artigos CTBMFDocument6 pagesArtigos CTBMFpriscilavitalfialhoNo ratings yet
- Chotipanich 2018Document5 pagesChotipanich 2018abhishekjha0082No ratings yet
- 1 s2.0 S0901502709009941 MainDocument6 pages1 s2.0 S0901502709009941 MainDrGurkirpal Singh MarwahNo ratings yet
- Journal of Cranio-Maxillo-Facial Surgery: Case ReportDocument6 pagesJournal of Cranio-Maxillo-Facial Surgery: Case Reportnh7p6yctv8No ratings yet
- Orthodontic Treatmentafter High Condylectomyin Patientswith Unilateral Condylar HyperplasiaDocument9 pagesOrthodontic Treatmentafter High Condylectomyin Patientswith Unilateral Condylar HyperplasiaOrtodoncia UNAL 2020No ratings yet
- 2001 - Skeletal and Dento-Alveolar Stability After SurgicalDocument12 pages2001 - Skeletal and Dento-Alveolar Stability After SurgicalTien Li AnNo ratings yet
- FinalJ IncisionDocument3 pagesFinalJ IncisionMax FaxNo ratings yet
- Rosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanDocument10 pagesRosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanMarcela RibeiroNo ratings yet
- Cirugia de Modelos EllisDocument7 pagesCirugia de Modelos EllisMarllury PabonNo ratings yet
- Article 3Document7 pagesArticle 3Lana DbbNo ratings yet
- 14985-Article Text-29120-1-10-20210409Document6 pages14985-Article Text-29120-1-10-20210409Rakan KhtoomNo ratings yet
- Orthodontic Treatment of An Anterior Openbite With The Aid of Corticotomy Procedure Case ReportDocument12 pagesOrthodontic Treatment of An Anterior Openbite With The Aid of Corticotomy Procedure Case ReportSaile OlguinNo ratings yet
- Compartmental Surgery in Tongue Tumours: Description of A New Surgical TechniqueDocument6 pagesCompartmental Surgery in Tongue Tumours: Description of A New Surgical TechniqueDot DitNo ratings yet
- Palatal Torus: Etiology, Clinical Aspect, and Therapeutic StrategyDocument7 pagesPalatal Torus: Etiology, Clinical Aspect, and Therapeutic StrategyNauroh NaurohNo ratings yet
- Le Fort I Osteotomy: Steven M. Sullivan, DDSDocument13 pagesLe Fort I Osteotomy: Steven M. Sullivan, DDSAbdullah özelNo ratings yet
- Akira Saito Et Al. (2009)Document4 pagesAkira Saito Et Al. (2009)Janardana GedeNo ratings yet
- 9Document7 pages9Soal KoasNo ratings yet
- Surgical Ciliated Cyst of The Maxilla. Clinical Case: Jorge Cano, Julián Campo, Miguel Angel Alobera, Rafael BacaDocument4 pagesSurgical Ciliated Cyst of The Maxilla. Clinical Case: Jorge Cano, Julián Campo, Miguel Angel Alobera, Rafael BacaAhmad MustafaNo ratings yet
- Trismus-An Old Concept For Successfull Treatment in The Present Era - Case ReportsDocument6 pagesTrismus-An Old Concept For Successfull Treatment in The Present Era - Case ReportsjaslinshalinNo ratings yet
- Art CXDocument9 pagesArt CXMilena RamirezNo ratings yet
- Surgically Assisted Rapid Palatal Expansion:: An Outpatient Technique With Long-Term StabilityDocument4 pagesSurgically Assisted Rapid Palatal Expansion:: An Outpatient Technique With Long-Term StabilityemanNo ratings yet
- Modified Gap Arthroplasty and Myrhaugs Incision As A Treatment Option in Management of Temporomandibular Joint Ankylosis A Study of 10 CasesDocument6 pagesModified Gap Arthroplasty and Myrhaugs Incision As A Treatment Option in Management of Temporomandibular Joint Ankylosis A Study of 10 CasesS EllurNo ratings yet
- Using The Endoscopic Transconjunctival and Transcaruncular Approach To Repair Combined Orbital Floor and Medial Wall Blowout FracturesDocument4 pagesUsing The Endoscopic Transconjunctival and Transcaruncular Approach To Repair Combined Orbital Floor and Medial Wall Blowout Fracturesstoia_sebiNo ratings yet
- Successful Treatment of Intraorbital Lymphangioma With Tissue Fibrin GlueDocument3 pagesSuccessful Treatment of Intraorbital Lymphangioma With Tissue Fibrin GlueIRANo ratings yet
- Kyphectomy and Interbody Fixation Using Lag Screws in A Child With Myelomeningocele Kyphosis: A Technical Case ReportDocument4 pagesKyphectomy and Interbody Fixation Using Lag Screws in A Child With Myelomeningocele Kyphosis: A Technical Case Reportalireza arvinNo ratings yet
- The Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingFrom EverandThe Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingJanindra WarusavitarneNo ratings yet
- T3, T4, TSH Levels in HypothyroidismDocument6 pagesT3, T4, TSH Levels in HypothyroidismInternational Organization of Scientific Research (IOSR)No ratings yet
- The Brain and Cranial Nerves: Lecture Slides Prepared by Curtis Defriez, Weber State UniversityDocument81 pagesThe Brain and Cranial Nerves: Lecture Slides Prepared by Curtis Defriez, Weber State UniversityKristine SanchezNo ratings yet
- (Ent) 02 Endoscopy Applied Physiology EditedDocument5 pages(Ent) 02 Endoscopy Applied Physiology EditedKanako TakayaNo ratings yet
- The Cranial NervesDocument28 pagesThe Cranial NervestauseefNo ratings yet
- G5 Nasal CavityDocument41 pagesG5 Nasal CavityGuo YageNo ratings yet
- Block Based LearningDocument12 pagesBlock Based LearningRevathi DadamNo ratings yet
- Biological Psychology: A Brief HistoryDocument29 pagesBiological Psychology: A Brief Historymarty_martinNo ratings yet
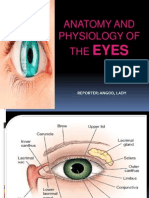
- Anatomy and Physiology of The EyesDocument20 pagesAnatomy and Physiology of The EyesLaidy Aizahlyn Indoc Angod100% (2)
- Review of Ophthlamology A K Khurana 7th EdDocument221 pagesReview of Ophthlamology A K Khurana 7th EdIvan KristenNo ratings yet
- Cunningham's Manual of Practical Anatomy (Volume 2)Document657 pagesCunningham's Manual of Practical Anatomy (Volume 2)alt.v7-aoksak4cNo ratings yet
- Presentation 1Document12 pagesPresentation 1Maryam KhanNo ratings yet
- Anatomy of PharynxDocument27 pagesAnatomy of PharynxParul Gupta100% (2)
- Cephalometric Evaluation of GrowthDocument79 pagesCephalometric Evaluation of GrowthAhmedsy Ahmedsy AhmedsyNo ratings yet
- Primary FRCA - OSCEs in Anaesthesia (PDFDrive)Document310 pagesPrimary FRCA - OSCEs in Anaesthesia (PDFDrive)Manuela CormioNo ratings yet
- Cns Neurological ExaminationDocument26 pagesCns Neurological ExaminationDr.P.NatarajanNo ratings yet
- Neuroplasticity Exercises' Influence On Adolescent StudentsDocument14 pagesNeuroplasticity Exercises' Influence On Adolescent Studentsapi-599270977No ratings yet
- A Layered Approach To Neck LiftDocument12 pagesA Layered Approach To Neck LiftenzoNo ratings yet
- Psy Frumos Ochi MiciDocument3 pagesPsy Frumos Ochi MiciDenisa MoțatuNo ratings yet
- Gen Psych - Chapter 2Document30 pagesGen Psych - Chapter 2Mhild GandawaliNo ratings yet
- Anatomy Cheat SheetDocument11 pagesAnatomy Cheat SheetVishwajeet RaneNo ratings yet
- 91637-Meninges Brain and Spain - Majda ThurnherDocument14 pages91637-Meninges Brain and Spain - Majda ThurnherFaith ManiquisNo ratings yet
- BrainstemDocument22 pagesBrainstemsammycraigNo ratings yet
- Anatomy of The NeckDocument27 pagesAnatomy of The NeckDiane ApostolNo ratings yet
- Sensory Tracts: DR Raghuveer Choudhary Associate Professor Dept. of Physiology DR S.N.Medical College, JodhpurDocument40 pagesSensory Tracts: DR Raghuveer Choudhary Associate Professor Dept. of Physiology DR S.N.Medical College, JodhpurPhysiology by Dr RaghuveerNo ratings yet
- Oral Habits 1233Document43 pagesOral Habits 1233Sayuj SureshNo ratings yet
- Sense OrgansDocument26 pagesSense OrgansArpan AdhikariNo ratings yet
- Practical Ent AbridgedDocument17 pagesPractical Ent AbridgedAishaNo ratings yet
- The Nervous System: Lecture Presentation by Patty Bostwick-Taylor Florence-Darlington Technical CollegeDocument196 pagesThe Nervous System: Lecture Presentation by Patty Bostwick-Taylor Florence-Darlington Technical CollegeTrisha100% (8)