Download as pdf or txt
You might also like
- Introduction To Health Psychology 2022Document721 pagesIntroduction To Health Psychology 2022Brain Smith100% (4)
- Test Bank For Health Psychology Biopsychosocial Interactions 8th Edition Edward P Sarafino DownloadDocument16 pagesTest Bank For Health Psychology Biopsychosocial Interactions 8th Edition Edward P Sarafino Downloadbraccatepondfish.eb2q9100% (47)
- Archer USMLE Step 3 Question BankDocument116 pagesArcher USMLE Step 3 Question Bankrolpf garri33% (3)
- Assignment 4Document8 pagesAssignment 4api-328441669100% (1)
- Dr. Berg Amazing TechniquesDocument17 pagesDr. Berg Amazing Techniqueslucaemigrante100% (6)
- Endocrine RevisonDocument21 pagesEndocrine Revisonalistair.james.clarkeNo ratings yet
- Calcium-Bone Metabolism Case DiscussionsDocument10 pagesCalcium-Bone Metabolism Case DiscussionswhooziesNo ratings yet
- A Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesFrom EverandA Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesNo ratings yet
- Name Olusegun SDocument10 pagesName Olusegun SIsrael OlusegunNo ratings yet
- Hiperparatiroid: Dr. Dr. Shahrul Rahman, SP - PD, FINASIMDocument50 pagesHiperparatiroid: Dr. Dr. Shahrul Rahman, SP - PD, FINASIMBonitavanyNo ratings yet
- Bhatia Diabetes SpecialDocument24 pagesBhatia Diabetes Specialnaga tanoojNo ratings yet
- Assignment 3Document5 pagesAssignment 3api-577583685No ratings yet
- A Simple Guide to Parathyroid Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Parathyroid Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Thornton 2016Document5 pagesThornton 2016AfdhalRuslanNo ratings yet
- 2 - Med - Endocrine MCQs - SGDocument33 pages2 - Med - Endocrine MCQs - SGOsman Somi50% (2)
- Parathyroid Glands: Serum PTH Levels Are Inappropriately Elevated For The LevelDocument4 pagesParathyroid Glands: Serum PTH Levels Are Inappropriately Elevated For The LevelNada MuchNo ratings yet
- Phase 2a Endocrinology - Sba Saq Session 2Document54 pagesPhase 2a Endocrinology - Sba Saq Session 2Zeyad AmrNo ratings yet
- Metabolic Bone ConditionsDocument66 pagesMetabolic Bone ConditionsNaeem AminNo ratings yet
- HypercalcemiaDocument6 pagesHypercalcemiajamil aoudeNo ratings yet
- Management of Normocalcemic Primary HyperparathyroidismDocument19 pagesManagement of Normocalcemic Primary HyperparathyroidismErika AvilaNo ratings yet
- CP PPQsDocument5 pagesCP PPQsJenny LowsleyNo ratings yet
- PIR 2023 HypocalcemiaDocument5 pagesPIR 2023 HypocalcemiamasonicpgsNo ratings yet
- Endocrinology 101 150Document29 pagesEndocrinology 101 150Ahmed El AlfyNo ratings yet
- HyperparathyroidismDocument5 pagesHyperparathyroidismapi-297055195No ratings yet
- Chronic Kidney Disease AffaqDocument7 pagesChronic Kidney Disease AffaqAfaq ali khanNo ratings yet
- Hypercalcemic Crisis: Reinhard ZieglerDocument7 pagesHypercalcemic Crisis: Reinhard ZieglerRo KohnNo ratings yet
- CA A Cancer J Clinicians - 2018 - Zagzag - Hypercalcemia and Cancer Differential Diagnosis and TreatmentDocument10 pagesCA A Cancer J Clinicians - 2018 - Zagzag - Hypercalcemia and Cancer Differential Diagnosis and TreatmentWilliam Perero RodríguezNo ratings yet
- Weakness Following Diarrhea: 1/4: 1. What Can Be The Cause of Her Condition?Document4 pagesWeakness Following Diarrhea: 1/4: 1. What Can Be The Cause of Her Condition?ZauzaNo ratings yet
- Dr. Rabia 1700 Plab Material McqsDocument1,092 pagesDr. Rabia 1700 Plab Material McqsMuhammad Amin100% (9)
- Thyrotoxic Periodic Paralysis As A Presentation of Thyrotoxicosis: A Case ReportDocument4 pagesThyrotoxic Periodic Paralysis As A Presentation of Thyrotoxicosis: A Case ReportAdvanced Research PublicationsNo ratings yet
- 2 - Parathyroid GlandDocument21 pages2 - Parathyroid Glandtaha55860No ratings yet
- (03241750 - Acta Medica Bulgarica) Recurrent Hyponatremia As Presenting Manifestation of Pituitary MacroadenomaDocument4 pages(03241750 - Acta Medica Bulgarica) Recurrent Hyponatremia As Presenting Manifestation of Pituitary MacroadenomaTeodorNo ratings yet
- Thyroid Gland McqsDocument6 pagesThyroid Gland Mcqssabreena.samad.ssNo ratings yet
- Parathyroid DiseaseDocument10 pagesParathyroid Diseasemohammedghassan53No ratings yet
- McceeDocument3 pagesMcceedocali11No ratings yet
- Screenshot 2023-04-01 at 11.36.03 AM PDFDocument29 pagesScreenshot 2023-04-01 at 11.36.03 AM PDFqurathNo ratings yet
- MCQs Endo FinalDocument6 pagesMCQs Endo Finalhassan qureshiNo ratings yet
- BIO 202 Essay 1Document2 pagesBIO 202 Essay 1Cindy PetersonNo ratings yet
- Primary HyperparathyroidismDocument13 pagesPrimary Hyperparathyroidismqayyum consultantfpscNo ratings yet
- Hypercalcemia, An Uncommon Presentation of HyperthyroidismDocument2 pagesHypercalcemia, An Uncommon Presentation of HyperthyroidismJOSE LUIS COTRINA CASTAÑEDANo ratings yet
- Critical Care PASSTHEMRCSDocument131 pagesCritical Care PASSTHEMRCSthinzarNo ratings yet
- Ppe (2016-2017) #31Document23 pagesPpe (2016-2017) #31باقر كاظم عبد الشريفNo ratings yet
- Module 2 Fluid Electrolyte Disorders Acid Base NotesDocument9 pagesModule 2 Fluid Electrolyte Disorders Acid Base NotesSara FNo ratings yet
- Case History 33Document4 pagesCase History 33Hida KurticNo ratings yet
- NCM 106 Learning Activities (Semis)Document12 pagesNCM 106 Learning Activities (Semis)Kimberly Abellar LatoNo ratings yet
- Rachel I Gafni Hypoparathyroidism 2019Document10 pagesRachel I Gafni Hypoparathyroidism 2019Ibrahim SabraNo ratings yet
- Parathyroid, HyperparathyroidismDocument4 pagesParathyroid, Hyperparathyroidismjamil aoudeNo ratings yet
- אלון קלציום חלק 3Document25 pagesאלון קלציום חלק 3Alon GoldfainerNo ratings yet
- 2 Bvab048.1976Document1 page2 Bvab048.1976Anca LunguNo ratings yet
- Endocrinology Best RDocument27 pagesEndocrinology Best RfrabziNo ratings yet
- Volume 2 GDVs and More - Rev1 Ed6jvjDocument39 pagesVolume 2 GDVs and More - Rev1 Ed6jvjErhan ErtuçNo ratings yet
- Hyperparathyroidism Main Jan 2020Document20 pagesHyperparathyroidism Main Jan 2020paingmyint100% (1)
- Review Sheet Laprak EndokrinDocument4 pagesReview Sheet Laprak EndokrinrhismaNo ratings yet
- Medicine: Hyperthyroidism-Associated Hypercalcemic CrisisDocument4 pagesMedicine: Hyperthyroidism-Associated Hypercalcemic CrisisDwinkha Agita PNo ratings yet
- Disorders of The Parathyroid GlandsDocument30 pagesDisorders of The Parathyroid Glandsikram ullah khan100% (1)
- Pediatric Endocrinology Review MCQS: Part - 6Document29 pagesPediatric Endocrinology Review MCQS: Part - 6wanjala francis xavierNo ratings yet
- Hypoparathyroidism NEJM 2019 PDFDocument10 pagesHypoparathyroidism NEJM 2019 PDFalejandro toro riveraNo ratings yet
- Familia HypercholesterolemiaDocument12 pagesFamilia Hypercholesterolemia909 Devang GawasNo ratings yet
- Case Hipertensi SekunderDocument8 pagesCase Hipertensi Sekunderkintan utariNo ratings yet
- Hypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 3.4 Paralytic Ileus Due To Potassium Depletion. Dr. S. GieveDocument3 pages3.4 Paralytic Ileus Due To Potassium Depletion. Dr. S. GieveDaru KristiyonoNo ratings yet
- Study Guide For NURS 320 Exam 2Document15 pagesStudy Guide For NURS 320 Exam 2Anthony Del RioNo ratings yet
- Health Hazards in The Pharmaceutical Industry 2167 7689 1000145Document15 pagesHealth Hazards in The Pharmaceutical Industry 2167 7689 1000145Emillya SariNo ratings yet
- APA Draft Practice Guidelines Eating DisordersDocument139 pagesAPA Draft Practice Guidelines Eating DisordersGaby ZavalaNo ratings yet
- PINS in Brief July 2023Document20 pagesPINS in Brief July 2023Luke TEARONo ratings yet
- Healthcare in Myanmar: Review ArticleDocument12 pagesHealthcare in Myanmar: Review ArticleMin Chan Moon100% (1)
- A. Read The Text Below and Answer The QuestionsDocument6 pagesA. Read The Text Below and Answer The QuestionsMihaela CarabatNo ratings yet
- Assessing The Contribution of The Level of Knowledge and Awareness of HIV and AIDS To The Effective Implementation of Desired HIVAIDS Prevention Intervention Programs in Higher Tertiary InstitutionsDocument12 pagesAssessing The Contribution of The Level of Knowledge and Awareness of HIV and AIDS To The Effective Implementation of Desired HIVAIDS Prevention Intervention Programs in Higher Tertiary InstitutionsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Study On Hospital Acquired Infection ADocument22 pagesA Study On Hospital Acquired Infection AKamal Babu ENo ratings yet
- ISMST GuidelinesDocument112 pagesISMST GuidelinesDhrubo TaraNo ratings yet
- Eccentric Exercise Program Design - A Periodization Model For Rehabilitation ApplicationsDocument37 pagesEccentric Exercise Program Design - A Periodization Model For Rehabilitation ApplicationsDeivison Fellipe da Silva CâmaraNo ratings yet
- Knee InjuryDocument44 pagesKnee Injuryhendi_filipus_90No ratings yet
- Total Anomalous Pulmonary Venous ConnectionDocument30 pagesTotal Anomalous Pulmonary Venous Connectionwiyay34652ceoshubcomNo ratings yet
- Remember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your OwnDocument11 pagesRemember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your Ownavinash dhameriyaNo ratings yet
- Hypertensive Disorder in Pregnancy-5-19-2015-ZimbabweDocument39 pagesHypertensive Disorder in Pregnancy-5-19-2015-ZimbabwedanielNo ratings yet
- Direct Recruitment To The Posts of Officer Grade B (Manager) and Officer Grade A (Assistant Manager)Document4 pagesDirect Recruitment To The Posts of Officer Grade B (Manager) and Officer Grade A (Assistant Manager)Anmol SinghNo ratings yet
- Quadas 2Document11 pagesQuadas 2SelvaArockiamNo ratings yet
- Bela Fer Dextran K 08 03Document2 pagesBela Fer Dextran K 08 03andreisandorNo ratings yet
- Pharmacology On Your PalmsDocument75 pagesPharmacology On Your PalmsReza JahanimirNo ratings yet
- KBG SymptomDocument4 pagesKBG SymptomMidhun Thomas EdathinalNo ratings yet
- Parasitology LectureDocument7 pagesParasitology Lectureangela verayeNo ratings yet
- Keep It Clean!: Hygiene in The SalonDocument10 pagesKeep It Clean!: Hygiene in The SalonThe Health Therapist AcademyNo ratings yet
- Lesson Guide SampleDocument7 pagesLesson Guide SampleSehun OohNo ratings yet
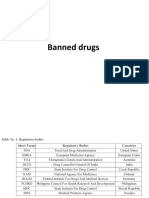
- Banned DrugsDocument26 pagesBanned DrugskarthikeyanpgtNo ratings yet
- 722 1983 1 PBDocument4 pages722 1983 1 PBravi_seth_9No ratings yet
- Pharma Final ModuleDocument139 pagesPharma Final ModuleQuantum XavierNo ratings yet
- Wolfis Law Letter PrintDocument1 pageWolfis Law Letter PrintSatyam PatelNo ratings yet
- Application of Nursing Standards Is A Must in Community Health Nursing. To Whom of The Following Do These Standards Apply?Document27 pagesApplication of Nursing Standards Is A Must in Community Health Nursing. To Whom of The Following Do These Standards Apply?L1NEDS DNo ratings yet
- Problem Set 1 Solutions: Statistics 104 Due February 6, 2020 at 11:59 PMDocument18 pagesProblem Set 1 Solutions: Statistics 104 Due February 6, 2020 at 11:59 PMjoshua arnettNo ratings yet