Download as pdf or txt
You might also like
- Lecture On MEASLESDocument16 pagesLecture On MEASLESNicole Villanueva, BSN - Level 3ANo ratings yet
- Patrick, Ph.D. Guilfoile-Tetanus (Deadly Diseases and Epidemics) (2008)Document101 pagesPatrick, Ph.D. Guilfoile-Tetanus (Deadly Diseases and Epidemics) (2008)FATIN NAJIHAH100% (1)
- CorynebacteriumDocument7 pagesCorynebacteriumskNo ratings yet
- Diphtheria HandoutsDocument8 pagesDiphtheria HandoutsRachelle Mae DimayugaNo ratings yet
- Diphtheria Pertussis TetanusDocument43 pagesDiphtheria Pertussis Tetanuspnalinl108No ratings yet
- Diphtheria Pertussis TetanusDocument43 pagesDiphtheria Pertussis TetanusPURVI BARIANo ratings yet
- Tuberculosis: DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistDocument59 pagesTuberculosis: DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- I-1B. Bacterial Infection 2Document6 pagesI-1B. Bacterial Infection 2Soad ShedeedNo ratings yet
- Diphtheria JellyDocument23 pagesDiphtheria JellyRexaurus EncarriosusNo ratings yet
- ImpetigoDocument66 pagesImpetigozbestgurlNo ratings yet
- Infections of Larynx: Drravikumar M.S (ENT)Document57 pagesInfections of Larynx: Drravikumar M.S (ENT)Drravikumar BhandariNo ratings yet
- Group 1Document20 pagesGroup 1Emily BalmesNo ratings yet
- Catarrhal Stage: 1-2 Weeks Coryza, FeverDocument45 pagesCatarrhal Stage: 1-2 Weeks Coryza, FeverAbigail BrillantesNo ratings yet
- UNIT I Disorders Spread by Droplet InfectionsDocument20 pagesUNIT I Disorders Spread by Droplet InfectionsAmmar BhattiNo ratings yet
- DIPTHERIADocument2 pagesDIPTHERIADr KhatidjaNo ratings yet
- Diphtheria - Pertussis (REPORT)Document48 pagesDiphtheria - Pertussis (REPORT)Charlz ZipaganNo ratings yet
- In House COMMUNICABLE DISEASES HANDOUTDocument10 pagesIn House COMMUNICABLE DISEASES HANDOUTniczdelosreyes8No ratings yet
- Epidemiology of Communicable DiseaseDocument256 pagesEpidemiology of Communicable DiseaseShubhaNo ratings yet
- A Presentation On-: Dr. Nikhil Oza Intern BvdumcDocument43 pagesA Presentation On-: Dr. Nikhil Oza Intern BvdumcMaheboob GanjalNo ratings yet
- PERTUSISDocument28 pagesPERTUSISFaridNorNo ratings yet
- 4i4 (L@pq2b50ya1ku4Document16 pages4i4 (L@pq2b50ya1ku4Kristel AnneNo ratings yet
- D Canine InfectiousDocument8 pagesD Canine InfectiousshemeshjNo ratings yet
- Diptheria Converted 200726175940Document44 pagesDiptheria Converted 2007261759407dbnf4stjyNo ratings yet
- (Whooping Cough) : PertussisDocument19 pages(Whooping Cough) : PertussisFerdinand Rosendo JrNo ratings yet
- Diseases Affecting Respiratory SystemDocument21 pagesDiseases Affecting Respiratory Systemzchantal08.prietoNo ratings yet
- Oxygenation ReviewerDocument8 pagesOxygenation ReviewerDamie FernandezNo ratings yet
- MEASLESDocument34 pagesMEASLESImran KhanNo ratings yet
- Community Notes by DR - Khan Final-1Document44 pagesCommunity Notes by DR - Khan Final-1Aqib IshaqNo ratings yet
- DiphtheriaDocument15 pagesDiphtheriaelka.kgmaNo ratings yet
- PertussisDocument17 pagesPertussisAbduraman NazifNo ratings yet
- Diphtheria: By: Aguilloso, Shella Cano, Charnelle Jayne GDocument19 pagesDiphtheria: By: Aguilloso, Shella Cano, Charnelle Jayne Gjudith_carlosNo ratings yet
- Nursing Care of Patients With Respiratory Comunicable DiseasesDocument74 pagesNursing Care of Patients With Respiratory Comunicable DiseasesGiselle EstoquiaNo ratings yet
- Lerelyn Case Reading4Document53 pagesLerelyn Case Reading4Ma Lerelyn DatinguinooNo ratings yet
- Vaccine Preventable Communicable DiseasesDocument7 pagesVaccine Preventable Communicable DiseasesmadmarycashNo ratings yet
- Tuberculosis 150808111627 Lva1 App6891Document43 pagesTuberculosis 150808111627 Lva1 App6891RAMJIBAN YADAVNo ratings yet
- Pulmonary Diseases - Dental ManagementDocument45 pagesPulmonary Diseases - Dental Managementfilyouth4life100% (3)
- Whooping CoughDocument19 pagesWhooping CoughSalaxar Senpai0% (1)
- Pulmonary Tuberculosis (PTB)Document6 pagesPulmonary Tuberculosis (PTB)carls burg a. resurreccion100% (2)
- Pathogens That Involve The Respiratory TractDocument28 pagesPathogens That Involve The Respiratory TractLeeShauran100% (2)
- NCM109 - Reviewer-Lp-1-To-Lp-4Document54 pagesNCM109 - Reviewer-Lp-1-To-Lp-4princessNo ratings yet
- East Africa University Bosaso, Puntland Somalia Faculty of Medicine Communicable Disease MR Buruj Ali SaladDocument42 pagesEast Africa University Bosaso, Puntland Somalia Faculty of Medicine Communicable Disease MR Buruj Ali SaladShaimaa AbdulkadirNo ratings yet
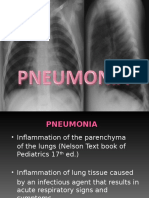
- Pneumonia 1Document35 pagesPneumonia 1suheel raiNo ratings yet
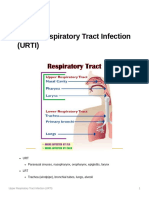
- 8 - Upper Respiratory Tract Infection (URTI)Document21 pages8 - Upper Respiratory Tract Infection (URTI)Kaela Beatrice Sy LatoNo ratings yet
- Diphtheria and MeaslesDocument35 pagesDiphtheria and MeaslesMurugesanNo ratings yet
- DIPTHERIADocument2 pagesDIPTHERIARhoanne HandangNo ratings yet
- Diphtheria: Sabah Mohsin Al-Maamuri MDDocument3 pagesDiphtheria: Sabah Mohsin Al-Maamuri MDAmmar AlnajjarNo ratings yet
- Microbial Diseases of The Respiratory SystemDocument9 pagesMicrobial Diseases of The Respiratory SystemAnaNo ratings yet
- L23 - Pneumonia MedDocument51 pagesL23 - Pneumonia MedAL-ashai MohammedNo ratings yet
- Respiratory Tract Infections 2022Document36 pagesRespiratory Tract Infections 2022m-9904772No ratings yet
- Tuberculosis PowerpointDocument69 pagesTuberculosis PowerpointCeline Villo100% (1)
- Vaccine PreventableDocument89 pagesVaccine PreventableMohammad Doctor CabdiraxmanNo ratings yet
- Paramyxo PPRDocument14 pagesParamyxo PPRstraihan234No ratings yet
- Circulatory System: Nursing Care of Patient With Disease of TheDocument56 pagesCirculatory System: Nursing Care of Patient With Disease of TheMada mada DaneNo ratings yet
- BPNDocument49 pagesBPNlovelots1234100% (1)
- Diphtheria Pertussis TetanusDocument43 pagesDiphtheria Pertussis TetanusRomel Ciptoadi WijayaNo ratings yet
- Kuliah Respirologi Anak: Divisi Respirologi Departemen Ilmu Kesehatan Anak FK Undip / Rsup DR Kariadi SemarangDocument114 pagesKuliah Respirologi Anak: Divisi Respirologi Departemen Ilmu Kesehatan Anak FK Undip / Rsup DR Kariadi SemarangLailatuz ZakiyahNo ratings yet
- TB Pneumonia 1Document51 pagesTB Pneumonia 1Zelle Pastor YambaoNo ratings yet
- Department of Child Health Faculty of Medicine University of Syiah KualaDocument55 pagesDepartment of Child Health Faculty of Medicine University of Syiah KualaIrfandy Chairi Sulaiman LubisNo ratings yet
- Communicable DiseasesDocument7 pagesCommunicable DiseasesRaisa Robelle Quicho100% (1)
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- 1.2 Leptospirosis Dengue Fever Malaria Filariais EncephalitisDocument95 pages1.2 Leptospirosis Dengue Fever Malaria Filariais Encephalitisesbercinio8528valNo ratings yet
- Att SMYmcyjCHlx5R9Fsyl5vFmvJla8jNjmOSdqHRvHASxADocument95 pagesAtt SMYmcyjCHlx5R9Fsyl5vFmvJla8jNjmOSdqHRvHASxAesbercinio8528valNo ratings yet
- Sustainable Economic SystemDocument17 pagesSustainable Economic Systemesbercinio8528valNo ratings yet
- Ncmb+312+Lec Hematologic+ProblemsDocument135 pagesNcmb+312+Lec Hematologic+Problemsesbercinio8528valNo ratings yet
- Disturbances in Oxygenation: Prepared By: Dr. Potenciana A. MaromaDocument87 pagesDisturbances in Oxygenation: Prepared By: Dr. Potenciana A. Maromaesbercinio8528valNo ratings yet
- Ncmb+312+Lec Coronary+Artery+Diseases+Document46 pagesNcmb+312+Lec Coronary+Artery+Diseases+esbercinio8528valNo ratings yet
- Soal Pretest AnaerobDocument4 pagesSoal Pretest AnaerobmuthiajayantiNo ratings yet
- CDDocument6 pagesCDMei JoyNo ratings yet
- Dwnload Full Primary Care Art and Science of Advanced Practice Nursing 4th Edition Dunphy Test Bank PDFDocument35 pagesDwnload Full Primary Care Art and Science of Advanced Practice Nursing 4th Edition Dunphy Test Bank PDFsangpaulina100% (13)
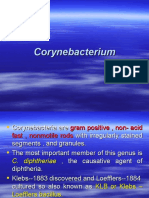
- Cory Ne BacteriumDocument28 pagesCory Ne BacteriumDayana PrasanthNo ratings yet
- CHN Combined WordDocument88 pagesCHN Combined WordRayne BonifacioNo ratings yet
- Special MicrobiologyDocument68 pagesSpecial MicrobiologyrefuapalackyNo ratings yet
- DiphtheriaDocument25 pagesDiphtheriaRohan TejaNo ratings yet
- Case Investigation Form: DiphtheriaDocument3 pagesCase Investigation Form: DiphtheriaSalihu MustaphaNo ratings yet
- HPA Maldives PDFDocument93 pagesHPA Maldives PDFshifanahmedNo ratings yet
- Toronto Public Health - Immunization of ChildrenDocument8 pagesToronto Public Health - Immunization of ChildrenCityNewsTorontoNo ratings yet
- Micro-Para Lec Diseases (Final)Document15 pagesMicro-Para Lec Diseases (Final)gelaciosandrageeNo ratings yet
- Communicable Diseases ReviewerDocument12 pagesCommunicable Diseases ReviewerClarissa GuifayaNo ratings yet
- CD Part 2 - Communicable Diseases With Pics (1) ConDocument239 pagesCD Part 2 - Communicable Diseases With Pics (1) ConMackoi SalamanesNo ratings yet
- 420 052 Guideline DiphtheriaDocument12 pages420 052 Guideline DiphtheriaLeo RinaldiNo ratings yet
- Communicable Disease NursingDocument41 pagesCommunicable Disease NursingBJ DUQUESA100% (2)
- No Batch Vaksin 2018Document8 pagesNo Batch Vaksin 2018lia fitrianiNo ratings yet
- First Term QP - Paper 4 - 6 E-AssessmentDocument15 pagesFirst Term QP - Paper 4 - 6 E-Assessmentyossra_abdullaNo ratings yet
- Seminar ON: Communicable DiseasesDocument159 pagesSeminar ON: Communicable DiseasesvishnuNo ratings yet
- ID Perbandingan Pemeriksaan ToksigenisitasDocument9 pagesID Perbandingan Pemeriksaan ToksigenisitasindahdwirahNo ratings yet
- Chapter 1: Diphtheria: I. Disease DescriptionDocument10 pagesChapter 1: Diphtheria: I. Disease DescriptionTina MorleyNo ratings yet
- 6 DiphtheriaDocument63 pages6 DiphtheriaTresnanda BellawanaNo ratings yet
- The Poisoned Needle by Eleanor McBean 1957 VACCINATION A MEDICAL DELUSION by Rex U LloydDocument186 pagesThe Poisoned Needle by Eleanor McBean 1957 VACCINATION A MEDICAL DELUSION by Rex U Lloydycescudero100% (3)
- Diphtheria HandoutsDocument8 pagesDiphtheria HandoutsRachelle Mae DimayugaNo ratings yet
- Tetanus Consent FormDocument2 pagesTetanus Consent FormAnmol PandeyNo ratings yet
- 8.2 UNDER FIVE CLINIC MCDocument8 pages8.2 UNDER FIVE CLINIC MCvicky RoseNo ratings yet
- CR Mbak YuliDocument10 pagesCR Mbak YuliNovel WidyaNo ratings yet
- Dr. DEEPAK.N.S (PG), Dr. PAGADPALLY SRINIVAS (Professor & Head) Dept. of Paediatrics, VMMC, KKLDocument2 pagesDr. DEEPAK.N.S (PG), Dr. PAGADPALLY SRINIVAS (Professor & Head) Dept. of Paediatrics, VMMC, KKLSumanth KumarNo ratings yet
- Microbiology TablesDocument19 pagesMicrobiology TablesRebecca MarshallNo ratings yet