
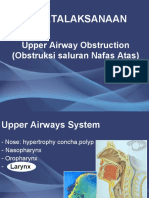
Airway Obstruction
Airway Obstruction
You might also like
- Just You See Dr. Sunirmal Sarkar-1Document54 pagesJust You See Dr. Sunirmal Sarkar-1Gg K75% (4)
- (K24) Acute & Chronic LaryngitisDocument47 pages(K24) Acute & Chronic LaryngitisSyarifah Fauziah100% (3)
- ICALL's Crowdsourced List of Mental Health Professionals We Can Trust (23rd April 2021)Document1,403 pagesICALL's Crowdsourced List of Mental Health Professionals We Can Trust (23rd April 2021)Learner's LicenseNo ratings yet
- StridorDocument48 pagesStridorMahindra Kumar100% (1)
- Cardiac Electrophysiology 2 An Advanced Visual Guide For Nurses Techs and Fellows 2EDocument294 pagesCardiac Electrophysiology 2 An Advanced Visual Guide For Nurses Techs and Fellows 2ETemptation100% (4)
- Tracheostomy LectureDocument5 pagesTracheostomy LectureNashat SaadiNo ratings yet
- ENT LectureDocument14 pagesENT Lectureمنى حاج احمد100% (1)
- Upper Airways Obstruction For DR - Zaenal SP - THT-KLDocument28 pagesUpper Airways Obstruction For DR - Zaenal SP - THT-KLElqowiyyaNo ratings yet
- Respiratory System SummaryDocument6 pagesRespiratory System SummaryKiara GovenderNo ratings yet
- Pulmonology Short CasesDocument10 pagesPulmonology Short CasesRZ Ng100% (1)
- ReferatDocument26 pagesReferatAtikahNo ratings yet
- 4-Larynx. Cong&trauma of LarynxDocument26 pages4-Larynx. Cong&trauma of LarynxislamNo ratings yet
- 02 Acute Airway ObstructionDocument3 pages02 Acute Airway Obstructioncharmainemargaret.parreno.medNo ratings yet
- ENT Approach To StridorDocument2 pagesENT Approach To StridorVanessa HermioneNo ratings yet
- Exam 1Document4 pagesExam 1Nataraj LoganathanNo ratings yet
- Suppurative Lung Diseases: DR Taher El Naggar Prof of Pulmonary Medicine Ain Shams UniversityDocument65 pagesSuppurative Lung Diseases: DR Taher El Naggar Prof of Pulmonary Medicine Ain Shams UniversitykingmedicNo ratings yet
- Oxygenation ReviewerDocument8 pagesOxygenation ReviewerDamie FernandezNo ratings yet
- Reviewer HA LECTURE Assignments CompilationDocument5 pagesReviewer HA LECTURE Assignments CompilationAmbot sa ImoNo ratings yet
- Common Disorde Rs in ChildrenDocument172 pagesCommon Disorde Rs in Childrenblacklilha100% (1)
- Onciectasis - FDocument4 pagesOnciectasis - FhebaNo ratings yet
- Acute CoughDocument14 pagesAcute CoughMerna MahrousNo ratings yet
- File 18584Document12 pagesFile 18584Mohammed MuthanaNo ratings yet
- Upper Airway Resp DistressDocument25 pagesUpper Airway Resp DistressAlexander GoldfarbNo ratings yet
- 3-4-5 Larynx Pharynx EsophagusDocument25 pages3-4-5 Larynx Pharynx Esophagustaliya. shvetzNo ratings yet
- COPDDocument4 pagesCOPDitsmailbbkNo ratings yet
- Nursing Lecture RespiratoryDocument13 pagesNursing Lecture RespiratoryAedge010100% (1)
- P1 Medworld Academy: Respiratory SystemDocument123 pagesP1 Medworld Academy: Respiratory SystemThenunda തേനുണ്ടNo ratings yet
- E Learning RespiratoryDocument160 pagesE Learning RespiratoryGrape JuiceNo ratings yet
- Ear, Nose and Throat EmergenciesDocument3 pagesEar, Nose and Throat Emergenciesfmta100% (1)
- Boeerhave SyndromeDocument1 pageBoeerhave Syndromesmitha lakkavallyNo ratings yet
- CcroupDocument53 pagesCcroupOlivia BernadiNo ratings yet
- Acute EpiglottisDocument20 pagesAcute EpiglottissuciNo ratings yet
- Airway Obstruction Final2Document33 pagesAirway Obstruction Final2Mahindra KumarNo ratings yet
- Laryngitis, Laryngeal Paralysis, DDX of Stridor, StertorDocument44 pagesLaryngitis, Laryngeal Paralysis, DDX of Stridor, StertorDurand S. KhadkaNo ratings yet
- Infections and Tumors of The LarynxDocument45 pagesInfections and Tumors of The Larynxk8hxrn5ddbNo ratings yet
- Respiratory Disorders in ChildrenDocument77 pagesRespiratory Disorders in ChildrenJharaNo ratings yet
- Broncho PneumoniaDocument3 pagesBroncho PneumoniakathzcNo ratings yet
- 12 StridorDocument5 pages12 StridorLankeshwaraNo ratings yet
- Respi PACES - V2Document6 pagesRespi PACES - V2Rebecca Teng Siew YanNo ratings yet
- Approach To A Child With Cough and Difficulty in BreathingDocument23 pagesApproach To A Child With Cough and Difficulty in BreathingKashif Burki100% (2)
- Med Surg CH 49Document19 pagesMed Surg CH 49amberNo ratings yet
- High-Yield Review For The Pulmonary/Allergy/ENT Module Exam and USMLE Step 1Document6 pagesHigh-Yield Review For The Pulmonary/Allergy/ENT Module Exam and USMLE Step 1frabziNo ratings yet
- Acute LaryngitisDocument18 pagesAcute LaryngitisROXTA RAHULNo ratings yet
- Greywolfred: Allergic Rhinitis (Hay Fever)Document6 pagesGreywolfred: Allergic Rhinitis (Hay Fever)RI NANo ratings yet
- Upper Airway ObstructionDocument15 pagesUpper Airway ObstructionThelma ChikaNo ratings yet
- Online Learning ModuleDocument38 pagesOnline Learning ModuleMani SainiNo ratings yet
- ENT Practice MCQs With Key 4th Year MBBSDocument7 pagesENT Practice MCQs With Key 4th Year MBBSPatrick BatemanNo ratings yet
- Respiratory System: SecretionsDocument4 pagesRespiratory System: SecretionsMarian FloresNo ratings yet
- Subject Seminar ON Approach To StridorDocument68 pagesSubject Seminar ON Approach To StridorAimhigh_PPM100% (1)
- 13 Inflammatory Disorders of LarynxDocument83 pages13 Inflammatory Disorders of LarynxAbhishek ShahNo ratings yet
- Lower Airways ConditionsDocument6 pagesLower Airways ConditionsMabesNo ratings yet
- Respiratory Plab 1 Notes 2014: SamsonDocument19 pagesRespiratory Plab 1 Notes 2014: Samsonزكريا عمرNo ratings yet
- Laryngo Tracheo BronchitisDocument4 pagesLaryngo Tracheo BronchitisNichole CollinsNo ratings yet
- ENT MCQsDocument4 pagesENT MCQsMayar MohammadNo ratings yet
- TracheostomyDocument4 pagesTracheostomyAshiqur Rahman KhanNo ratings yet
- Lung SoundsDocument5 pagesLung SoundsAmiel dionisioNo ratings yet
- Lec 15a - Esophagial Atresia and Respiratory Emergencies in ChildrenDocument15 pagesLec 15a - Esophagial Atresia and Respiratory Emergencies in ChildrenAnas RbaihatNo ratings yet
- Lung AbscessDocument26 pagesLung AbscessPrajwal Rao KNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Anaphylaxis: A Practical GuideFrom EverandAnaphylaxis: A Practical GuideAnne K. EllisNo ratings yet
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- 3 Q Epidemiology Part 1Document26 pages3 Q Epidemiology Part 1Prince GoelNo ratings yet
- An Intensive Swallowing Exercise Protocol For Improving Swallowing Physiology in Older Adults With Radiographically Confirmed DysphagiaDocument7 pagesAn Intensive Swallowing Exercise Protocol For Improving Swallowing Physiology in Older Adults With Radiographically Confirmed DysphagiaMaria DemetriouNo ratings yet
- Flyer PIT IDI Bandung LINKDocument1 pageFlyer PIT IDI Bandung LINKBabo SanNo ratings yet
- Flinstones Sex-Linked Traits Worksheet - F12Document4 pagesFlinstones Sex-Linked Traits Worksheet - F12Sophia RichardsonNo ratings yet
- Overview of Nurses' Role in Management of Patient With Atrial FibrillationDocument5 pagesOverview of Nurses' Role in Management of Patient With Atrial FibrillationAhmed AlkhaqaniNo ratings yet
- JSA E&I 1.instrument Installation (Stand Mounted)Document5 pagesJSA E&I 1.instrument Installation (Stand Mounted)AmyNo ratings yet
- 6.sick Child Feeding Practice and Associated Factors Among Mothers of Children Less Than 24 Months Old, in Burayu Tow, EthiopiaDocument8 pages6.sick Child Feeding Practice and Associated Factors Among Mothers of Children Less Than 24 Months Old, in Burayu Tow, EthiopiaTomas YeheisNo ratings yet
- Catalogue v09Document4 pagesCatalogue v09KRISHNA L BAISETTINo ratings yet
- Phylum Nematoda PDFDocument257 pagesPhylum Nematoda PDFsummer dj100% (1)
- Abstract Book FinalDocument45 pagesAbstract Book Finalapi-200029530No ratings yet
- 1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamDocument4 pages1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamGeorgi GugicevNo ratings yet
- What Is ECG?Document2 pagesWhat Is ECG?Lê Thanh HàNo ratings yet
- Locomotor Training in People With Parkinson DiseaseDocument10 pagesLocomotor Training in People With Parkinson DiseasemilananandNo ratings yet
- Specialized Cells: Sperm Cell Oocyte Stem CellDocument45 pagesSpecialized Cells: Sperm Cell Oocyte Stem CellShiro MisakiNo ratings yet
- Chapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusDocument10 pagesChapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusAgnieszka WisniewskaNo ratings yet
- Interventional Cardiac Electrophysiology - A Multidisciplinary Approach Section 1, Technology and Therapeutic Techniques - PDF RoomDocument306 pagesInterventional Cardiac Electrophysiology - A Multidisciplinary Approach Section 1, Technology and Therapeutic Techniques - PDF RoomVeronica JanethNo ratings yet
- Feyer 2020 WvngoshawkDocument13 pagesFeyer 2020 WvngoshawkAgnieszka CzujkowskaNo ratings yet
- Benda Asing Dalam Kornea Akibat Kurangnya Peralatan Keselamatan: Laporan KasusDocument6 pagesBenda Asing Dalam Kornea Akibat Kurangnya Peralatan Keselamatan: Laporan KasusRachmad SammuliaNo ratings yet
- On LeukemiaDocument28 pagesOn LeukemiaMeena Koushal100% (1)
- Medical English - Viruses, Epidemics, and PandemicsDocument2 pagesMedical English - Viruses, Epidemics, and PandemicsМилена МићићNo ratings yet
- TriageDocument37 pagesTriagekyuleen05No ratings yet
- Dr. Ranjita Singh Department of PathologyDocument19 pagesDr. Ranjita Singh Department of PathologyMohan Prasad GuptaNo ratings yet
- ADA EASD Consensus 2012Document16 pagesADA EASD Consensus 2012Beta Cells in DiabetesNo ratings yet
- Maternal Experience With Neonatal JaundiceDocument9 pagesMaternal Experience With Neonatal JaundiceLorraine BuelvaNo ratings yet
- 17 ADD Type TestDocument7 pages17 ADD Type TestEvandro Pinho0% (1)
- Exam 5 TermsDocument2 pagesExam 5 Termsapi-315572926No ratings yet
- Synopsis in The Management of Urinary Incontinence - 2017Document102 pagesSynopsis in The Management of Urinary Incontinence - 2017Dennise IlieNo ratings yet























































































Download as docx, pdf, or txt
You might also like
- Just You See Dr. Sunirmal Sarkar-1Document54 pagesJust You See Dr. Sunirmal Sarkar-1Gg K75% (4)
- (K24) Acute & Chronic LaryngitisDocument47 pages(K24) Acute & Chronic LaryngitisSyarifah Fauziah100% (3)
- ICALL's Crowdsourced List of Mental Health Professionals We Can Trust (23rd April 2021)Document1,403 pagesICALL's Crowdsourced List of Mental Health Professionals We Can Trust (23rd April 2021)Learner's LicenseNo ratings yet
- StridorDocument48 pagesStridorMahindra Kumar100% (1)
- Cardiac Electrophysiology 2 An Advanced Visual Guide For Nurses Techs and Fellows 2EDocument294 pagesCardiac Electrophysiology 2 An Advanced Visual Guide For Nurses Techs and Fellows 2ETemptation100% (4)
- Tracheostomy LectureDocument5 pagesTracheostomy LectureNashat SaadiNo ratings yet
- ENT LectureDocument14 pagesENT Lectureمنى حاج احمد100% (1)
- Upper Airways Obstruction For DR - Zaenal SP - THT-KLDocument28 pagesUpper Airways Obstruction For DR - Zaenal SP - THT-KLElqowiyyaNo ratings yet
- Respiratory System SummaryDocument6 pagesRespiratory System SummaryKiara GovenderNo ratings yet
- Pulmonology Short CasesDocument10 pagesPulmonology Short CasesRZ Ng100% (1)
- ReferatDocument26 pagesReferatAtikahNo ratings yet
- 4-Larynx. Cong&trauma of LarynxDocument26 pages4-Larynx. Cong&trauma of LarynxislamNo ratings yet
- 02 Acute Airway ObstructionDocument3 pages02 Acute Airway Obstructioncharmainemargaret.parreno.medNo ratings yet
- ENT Approach To StridorDocument2 pagesENT Approach To StridorVanessa HermioneNo ratings yet
- Exam 1Document4 pagesExam 1Nataraj LoganathanNo ratings yet
- Suppurative Lung Diseases: DR Taher El Naggar Prof of Pulmonary Medicine Ain Shams UniversityDocument65 pagesSuppurative Lung Diseases: DR Taher El Naggar Prof of Pulmonary Medicine Ain Shams UniversitykingmedicNo ratings yet
- Oxygenation ReviewerDocument8 pagesOxygenation ReviewerDamie FernandezNo ratings yet
- Reviewer HA LECTURE Assignments CompilationDocument5 pagesReviewer HA LECTURE Assignments CompilationAmbot sa ImoNo ratings yet
- Common Disorde Rs in ChildrenDocument172 pagesCommon Disorde Rs in Childrenblacklilha100% (1)
- Onciectasis - FDocument4 pagesOnciectasis - FhebaNo ratings yet
- Acute CoughDocument14 pagesAcute CoughMerna MahrousNo ratings yet
- File 18584Document12 pagesFile 18584Mohammed MuthanaNo ratings yet
- Upper Airway Resp DistressDocument25 pagesUpper Airway Resp DistressAlexander GoldfarbNo ratings yet
- 3-4-5 Larynx Pharynx EsophagusDocument25 pages3-4-5 Larynx Pharynx Esophagustaliya. shvetzNo ratings yet
- COPDDocument4 pagesCOPDitsmailbbkNo ratings yet
- Nursing Lecture RespiratoryDocument13 pagesNursing Lecture RespiratoryAedge010100% (1)
- P1 Medworld Academy: Respiratory SystemDocument123 pagesP1 Medworld Academy: Respiratory SystemThenunda തേനുണ്ടNo ratings yet
- E Learning RespiratoryDocument160 pagesE Learning RespiratoryGrape JuiceNo ratings yet
- Ear, Nose and Throat EmergenciesDocument3 pagesEar, Nose and Throat Emergenciesfmta100% (1)
- Boeerhave SyndromeDocument1 pageBoeerhave Syndromesmitha lakkavallyNo ratings yet
- CcroupDocument53 pagesCcroupOlivia BernadiNo ratings yet
- Acute EpiglottisDocument20 pagesAcute EpiglottissuciNo ratings yet
- Airway Obstruction Final2Document33 pagesAirway Obstruction Final2Mahindra KumarNo ratings yet
- Laryngitis, Laryngeal Paralysis, DDX of Stridor, StertorDocument44 pagesLaryngitis, Laryngeal Paralysis, DDX of Stridor, StertorDurand S. KhadkaNo ratings yet
- Infections and Tumors of The LarynxDocument45 pagesInfections and Tumors of The Larynxk8hxrn5ddbNo ratings yet
- Respiratory Disorders in ChildrenDocument77 pagesRespiratory Disorders in ChildrenJharaNo ratings yet
- Broncho PneumoniaDocument3 pagesBroncho PneumoniakathzcNo ratings yet
- 12 StridorDocument5 pages12 StridorLankeshwaraNo ratings yet
- Respi PACES - V2Document6 pagesRespi PACES - V2Rebecca Teng Siew YanNo ratings yet
- Approach To A Child With Cough and Difficulty in BreathingDocument23 pagesApproach To A Child With Cough and Difficulty in BreathingKashif Burki100% (2)
- Med Surg CH 49Document19 pagesMed Surg CH 49amberNo ratings yet
- High-Yield Review For The Pulmonary/Allergy/ENT Module Exam and USMLE Step 1Document6 pagesHigh-Yield Review For The Pulmonary/Allergy/ENT Module Exam and USMLE Step 1frabziNo ratings yet
- Acute LaryngitisDocument18 pagesAcute LaryngitisROXTA RAHULNo ratings yet
- Greywolfred: Allergic Rhinitis (Hay Fever)Document6 pagesGreywolfred: Allergic Rhinitis (Hay Fever)RI NANo ratings yet
- Upper Airway ObstructionDocument15 pagesUpper Airway ObstructionThelma ChikaNo ratings yet
- Online Learning ModuleDocument38 pagesOnline Learning ModuleMani SainiNo ratings yet
- ENT Practice MCQs With Key 4th Year MBBSDocument7 pagesENT Practice MCQs With Key 4th Year MBBSPatrick BatemanNo ratings yet
- Respiratory System: SecretionsDocument4 pagesRespiratory System: SecretionsMarian FloresNo ratings yet
- Subject Seminar ON Approach To StridorDocument68 pagesSubject Seminar ON Approach To StridorAimhigh_PPM100% (1)
- 13 Inflammatory Disorders of LarynxDocument83 pages13 Inflammatory Disorders of LarynxAbhishek ShahNo ratings yet
- Lower Airways ConditionsDocument6 pagesLower Airways ConditionsMabesNo ratings yet
- Respiratory Plab 1 Notes 2014: SamsonDocument19 pagesRespiratory Plab 1 Notes 2014: Samsonزكريا عمرNo ratings yet
- Laryngo Tracheo BronchitisDocument4 pagesLaryngo Tracheo BronchitisNichole CollinsNo ratings yet
- ENT MCQsDocument4 pagesENT MCQsMayar MohammadNo ratings yet
- TracheostomyDocument4 pagesTracheostomyAshiqur Rahman KhanNo ratings yet
- Lung SoundsDocument5 pagesLung SoundsAmiel dionisioNo ratings yet
- Lec 15a - Esophagial Atresia and Respiratory Emergencies in ChildrenDocument15 pagesLec 15a - Esophagial Atresia and Respiratory Emergencies in ChildrenAnas RbaihatNo ratings yet
- Lung AbscessDocument26 pagesLung AbscessPrajwal Rao KNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Anaphylaxis: A Practical GuideFrom EverandAnaphylaxis: A Practical GuideAnne K. EllisNo ratings yet
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- 3 Q Epidemiology Part 1Document26 pages3 Q Epidemiology Part 1Prince GoelNo ratings yet
- An Intensive Swallowing Exercise Protocol For Improving Swallowing Physiology in Older Adults With Radiographically Confirmed DysphagiaDocument7 pagesAn Intensive Swallowing Exercise Protocol For Improving Swallowing Physiology in Older Adults With Radiographically Confirmed DysphagiaMaria DemetriouNo ratings yet
- Flyer PIT IDI Bandung LINKDocument1 pageFlyer PIT IDI Bandung LINKBabo SanNo ratings yet
- Flinstones Sex-Linked Traits Worksheet - F12Document4 pagesFlinstones Sex-Linked Traits Worksheet - F12Sophia RichardsonNo ratings yet
- Overview of Nurses' Role in Management of Patient With Atrial FibrillationDocument5 pagesOverview of Nurses' Role in Management of Patient With Atrial FibrillationAhmed AlkhaqaniNo ratings yet
- JSA E&I 1.instrument Installation (Stand Mounted)Document5 pagesJSA E&I 1.instrument Installation (Stand Mounted)AmyNo ratings yet
- 6.sick Child Feeding Practice and Associated Factors Among Mothers of Children Less Than 24 Months Old, in Burayu Tow, EthiopiaDocument8 pages6.sick Child Feeding Practice and Associated Factors Among Mothers of Children Less Than 24 Months Old, in Burayu Tow, EthiopiaTomas YeheisNo ratings yet
- Catalogue v09Document4 pagesCatalogue v09KRISHNA L BAISETTINo ratings yet
- Phylum Nematoda PDFDocument257 pagesPhylum Nematoda PDFsummer dj100% (1)
- Abstract Book FinalDocument45 pagesAbstract Book Finalapi-200029530No ratings yet
- 1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamDocument4 pages1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamGeorgi GugicevNo ratings yet
- What Is ECG?Document2 pagesWhat Is ECG?Lê Thanh HàNo ratings yet
- Locomotor Training in People With Parkinson DiseaseDocument10 pagesLocomotor Training in People With Parkinson DiseasemilananandNo ratings yet
- Specialized Cells: Sperm Cell Oocyte Stem CellDocument45 pagesSpecialized Cells: Sperm Cell Oocyte Stem CellShiro MisakiNo ratings yet
- Chapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusDocument10 pagesChapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusAgnieszka WisniewskaNo ratings yet
- Interventional Cardiac Electrophysiology - A Multidisciplinary Approach Section 1, Technology and Therapeutic Techniques - PDF RoomDocument306 pagesInterventional Cardiac Electrophysiology - A Multidisciplinary Approach Section 1, Technology and Therapeutic Techniques - PDF RoomVeronica JanethNo ratings yet
- Feyer 2020 WvngoshawkDocument13 pagesFeyer 2020 WvngoshawkAgnieszka CzujkowskaNo ratings yet
- Benda Asing Dalam Kornea Akibat Kurangnya Peralatan Keselamatan: Laporan KasusDocument6 pagesBenda Asing Dalam Kornea Akibat Kurangnya Peralatan Keselamatan: Laporan KasusRachmad SammuliaNo ratings yet
- On LeukemiaDocument28 pagesOn LeukemiaMeena Koushal100% (1)
- Medical English - Viruses, Epidemics, and PandemicsDocument2 pagesMedical English - Viruses, Epidemics, and PandemicsМилена МићићNo ratings yet
- TriageDocument37 pagesTriagekyuleen05No ratings yet
- Dr. Ranjita Singh Department of PathologyDocument19 pagesDr. Ranjita Singh Department of PathologyMohan Prasad GuptaNo ratings yet
- ADA EASD Consensus 2012Document16 pagesADA EASD Consensus 2012Beta Cells in DiabetesNo ratings yet
- Maternal Experience With Neonatal JaundiceDocument9 pagesMaternal Experience With Neonatal JaundiceLorraine BuelvaNo ratings yet
- 17 ADD Type TestDocument7 pages17 ADD Type TestEvandro Pinho0% (1)
- Exam 5 TermsDocument2 pagesExam 5 Termsapi-315572926No ratings yet
- Synopsis in The Management of Urinary Incontinence - 2017Document102 pagesSynopsis in The Management of Urinary Incontinence - 2017Dennise IlieNo ratings yet