Professional Documents
Culture Documents
LAM Lancet 2021
LAM Lancet 2021
Uploaded by
aabigutCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
LAM Lancet 2021
LAM Lancet 2021
Uploaded by
aabigutCopyright:
Available Formats
Review
Lymphangioleiomyomatosis: pathogenesis, clinical features,
diagnosis, and management
Cormac McCarthy, Nishant Gupta, Simon R Johnson, Jane J Yu, Francis X McCormack
Lymphangioleiomyomatosis (LAM) is a slowly progressive, low-grade, metastasising neoplasm of women, Lancet Respir Med 2021
characterised by infiltration of the lung parenchyma with abnormal smooth muscle-like cells, resulting in cystic lung Published Online
destruction. The invading cell in LAM arises from an unknown source and harbours mutations in tuberous sclerosis August 27, 2021
https://doi.org/10.1016/
complex (TSC) genes that result in constitutive activation of the mechanistic target of rapamycin (mTOR) pathway,
S2213-2600(21)00228-9
dysregulated cellular proliferation, and a programme of frustrated lymphangiogenesis, culminating in disordered
Department of Respiratory
lung remodelling and respiratory failure. Over the past two decades, all facets of LAM basic and clinical science have Medicine, St Vincent’s
seen important advances, including improved understanding of molecular mechanisms, novel diagnostic and University Hospital, University
prognostic biomarkers, effective treatment strategies, and comprehensive clinical practice guidelines. Further College Dublin, Dublin, Ireland
(C McCarthy PhD); Division of
research is needed to better understand the natural history of LAM; develop more powerful diagnostic, prognostic,
Pulmonary, Critical Care,
and predictive biomarkers; optimise the use of inhibitors of mTOR complex 1 in the treatment of LAM; and explore and Sleep Medicine, University
novel approaches to the development of remission-inducing therapies. of Cincinnati, Cincinnati,
OH, USA (N Gupta MD,
Introduction natural history of LAM, the optimisation of mTOR Prof J J Yu PhD,
Prof F X McCormack MD);
Lymphangioleiomyomatosis (LAM) is a rare, slowly inhibitor use, and the discovery of remission-inducing Division of Respiratory
progressive, systemic disease associated with cystic lung therapies. Medicine, University of
destruction, abdominal tumours, and chylous fluid In this Review, we highlight advances in understanding Nottingham, NIHR Respiratory
Biomedical Research Centre,
accumulations due to infiltration of neoplastic LAM cells.1–3 of disease pathogenesis, including molecular mechanisms
Nottingham, UK
These cells arise from an unknown source and probably of disease and targets for treatment. We describe the (Prof S R Johnson DM)
reach the lung via the lymphatic system or bloodstream. clinical features of LAM, discuss current approaches to Correspondence to:
Radiological evidence of LAM develops in most women evaluation and diagnosis, and provide an update on Dr Cormac McCarthy,
(30–60%)4–6 and up to 10% of men with tuberous sclerosis pharmacological treatment options and considerations for Department of Respiratory
Medicine, St Vincent’s University
complex (TSC), a multisystem genetic disease caused by
Hospital, University College
germline mutations in TSC genes, TSC1 or TSC2. LAM Dublin, Dublin 4, Ireland
occurring in patients with underlying TSC is termed Key messages cormac.mccarthy@ucd.ie
TSC-LAM. This disease can also occur sporadically in • In women with compatible cystic lung disease on a chest
women who do not have TSC, due to somatic mutations in CT scan, the additional presence of any one of the
the TSC2 gene, in a form known as sporadic LAM. following is sufficient to establish a definitive diagnosis of
Progressive dyspnoea on exertion and spontaneous lymphangioleiomyomatosis (LAM) without requiring a
pneumothorax are the most common presenting lung biopsy: tuberous sclerosis complex (TSC), elevated
manifestations of LAM. Pneumothorax tends to be serum vascular endothelial growth factor D (VEGF-D;
recurrent (lifetime average of 3–4 per patient) and a major ≥800 pg/mL), renal angiomyolipoma,
source of morbidity, often requiring multiple interventions. lymphangioleiomyoma, or chylous effusions
Angiomyolipomas occur in most patients with TSC-LAM • High-resolution CT screening of women of childbearing
and around 30–40% of those with sporadic LAM,7,8 age who present with spontaneous pneumothorax can
although lymphatic manifestations—including axial facilitate timely recognition of LAM
lymphadenopathy in the pelvis, abdomen, and chest, • Initial assessment in women with suspected LAM should
abdominal lymphangioleiomyomas, and chylous fluid include screening for angiomyolipoma, lymphatic
collections in the chest and abdomen—occur more involvement, and the presence of unrecognised TSC
frequently in patients with sporadic LAM (approximately • Disease manifestations and rate of progression in LAM
30–40%) than in those with TSC-LAM (10%).8 are highly variable and best managed with a personalised
Discovery of the genetic basis of LAM rapidly led to treatment and monitoring plan
trials of mechanistic target of rapamycin (mTOR) • mTORC1 inhibitors reduce loss of lung function, chylous
inhibitors, which showed efficacy in stabilising lung accumulation, and angiomyolipoma growth, and are the
function for most patients with LAM.9–11 Additional first-line treatment for patients with LAM
advances have included the development of a useful • Early definitive treatment for pneumothorax reduces
diagnostic and prognostic biomarker in the form of morbidity associated with recurrent spontaneous
vascular endothelial growth factor D (VEGF-D),12–14 pneumothoraces and should be considered after the
evidence for a uterine source of LAM cells,15 and the initial episode rather than after a recurrent event;
development of clinical practice guidelines.16–18 However, previous pleurodesis is not a contraindication for future
challenges that remain in meeting the needs of people lung transplantation
with LAM include progress in understanding of the
www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9 1
Review
the management of LAM. Finally, we consider the natural synthesis in a balanced and coordinated manner, and
history and prognosis of TSC-LAM and sporadic LAM. ultimately leads to cell growth and proliferation.29,36–39
Increased expression of the angiogenic factor VEGF-A,28
Epidemiology and lymphangiogenic growth factors VEGF-C and
Data suggest that sporadic LAM is restricted to VEGF-D, stimulates angiogenesis and the formation of
women.1,7,19 Although cystic change on CT consistent lymphatic channels within and around LAM lesions that
with LAM is seen in 10–38% of men with TSC,4,20,21 might facilitate access of LAM cells to the circulation.
including some cases with histological confirmation, There is increasing evidence that LAM cells are capable of
symptomatic disease is rare in men.22,23 There is one immune evasion though mTOR-dependent expression
report24 of suspected sporadic LAM in a man that was of checkpoint ligands and modulation of natural killer
shown to be caused by TSC mosaicism. Another report23 cell function.40–42 Improved understanding of disease
requires further confirmation because of limitations in pathogenesis has identified a multitude of potential
the sensitivity of genetic analysis to identify TSC treatment targets for patients with LAM (figure 1).
mutations and mosaicism at the time. LAM is estimated
to affect approximately 3·4–7·8 per million women, The metastatic origin of LAM
although the true prevalence is probably much higher.19 LAM has been reported to recur in donor allografts
TSC has an incidence of around 1 in 6000 births, a of patients who have undergone lung transplantation.
prevalence of 7–12 per 100 000 people, and no sex bias. The lesions are composed of LAM cells that have
Neither TSC nor LAM is known to have a geographical been genetically proven to arise from the recipient.43,44
or racial predilection.7 Conservative estimates suggest Although these findings first supported a metastatic
that there are approximately 8000–21 000 patients with mechanism for the disease almost 20 years ago,
sporadic LAM and 80 000–160 000 patients with TSC- the source of the invading cell has remained elusive.
LAM worldwide. Therefore, although TSC-LAM appears Because angiomyolipomas contain cells with genetic,
to be more common, more than 80% of patients with morphological, and immunohistochemical profiles that
LAM in pulmonary clinics, registries, and trials have are similar to those of LAM cells,45 these tumours have
sporadic LAM. This paradox remains unexplained, but been proposed as the potential primary origin; however,
could be attributable to differences in the severity of not all patients with LAM have angiomyolipomas.
sporadic LAM compared with TSC-LAM, or because LAM lesions have also been reported in the uterus,46–48
other TSC health priorities divert the focus of patients but whether the uterus is the source or another target of
with TSC and their health-care providers away from metastases has been the subject of debate. Single-cell
lung manifestations. RNA sequencing of lungs from patients with LAM
reveals an ectopic population of mesenchymal cells that
Pathogenesis express a uterine transcriptional programme, consistent
Signalling pathways in LAM pathogenesis with a uterine source.15 The same cellular transcriptional
TSC1 encodes hamartin and TSC2 encodes tuberin, profile was discovered in a mesenchymal subpopulation
which associate with TBC1D7 in a complex that functions by single-nuclear RNA sequencing of the uterus from a
as a key regulator of the kinase mTOR through an patient with sporadic LAM, and identical TSC2 mutations
intermediate G protein called Rheb.25–27 The intact were present in the uterus and lungs, also consistent
tuberin–hamartin complex maintains Rheb in an inactive, with a mechanism involving uterine metastasis. Other
GDP-bound form (figure 1). Phosphorylation of tuberin potential sources must exist given the occurrence of
by Akt (protein kinase B) inactivates the tuberin–hamartin LAM in males, and presumably would overlap with
complex, increases the abundance of Rheb-GTP, drives locations where perivascular epithelioid cell tumours
association of mTOR with Raptor (and mLST8 and have been found, including the kidney, bladder, prostate,
PRAS40) to form the mTORC1 complex, and results in gastrointestinal tract, soft tissue, and bone.
phosphorylation and activation of downstream proteins
mTOR, p70S6K, and 4E-BP1. These events lead to Sex hormone dependence
increased expression of proteases, HIF-1α, VEGF-A,28 LAM has the strongest sex predilection of any non-
VEGF-C, VEGF-D, and IMPDH;29 and inhibition of genitourinary neoplasm. The almost exclusive restriction
FKBP38–BCL2,30 transcription factor EB,31 and ULK1. of symptomatic LAM to women strongly suggests
The association of mTOR with Rictor (and mSIN1 that female hormones play an important part in the
and mLST8) to form mTORC2 results in activation of development and progression of the disease. LAM
Akt (Ser473), ROCK, and RhoA kinase, and expression cells uniformly express oestrogen and progesterone
of cyclooxygenase 2, thereby supporting glucose met receptors.49,50 Pulmonary symptoms worsen immediately
abol
ism, cell survival, cytoskeletal rearrangement, cell before and during menses in around 30% of women
movement, and prostaglandin metabolism.32–35 mTORC1 with LAM, and exogenous oestrogen use and pregnancy
hyperactivity in TSC mutant cells promotes anabolic have been associated with accelerated decline in lung
metabolism by increasing protein, lipid, and nucleotide function.51–55 Oestrogen promotes anoikis resistance,
2 www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9
Review
Ligand Oestrogen
RTK RTK inhibitors Oestrogen receptor antagonist
Oestrogen receptor
TSC1
TSC2
TBC1D7
(Inactive) Rheb-GDP
GAP
(Active) Rheb-GTP TSC Complex
resistance
metabolism
Glucose
Anoikis
MEK–MAPK B-Raf Raptor Rictor Akt
mTOR mTOR
MEK inhibitors
Sirolimus mTORC2
mTORC1
Lung remodelling and LAM cell metastasis
Angiogenesis
Everolimus
Cell survival and metastasis
HIF1α
Simvastatin
movement
Cell
VEGF-A
ROCK–RhoA
Lymphangio-
VEGF-C and VEGF-D
genesis
VEGFR3
inhibitors metabolism
Prostaglandin
Celecoxib
Extracellular matrix
MMP or CatK
inhibitors
P38
Resveratrol COX2
dynamics
FKB
TFEB
Hydroxychloroquine Mizoribine
MMP
ULK1
CatK
BCL2 4E-BP1 p70S6K IMPDH SREBP
Mitochondrial Lysosome Protein Nucleotide Lipid
Autophagy
degradation biogenesis translation synthesis synthesis
Apoptosis Cell survival Cell proliferation and growth
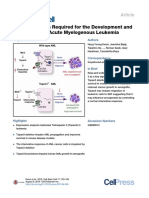
Figure 1: Dysregulation of signalling pathways in LAM pathogenesis reveals targets for LAM clinical trials
The TBC1D7, TSC1, and TSC2 protein complex inactivates GTPase Rheb via a GAP moiety on TSC2. Rheb suppression of B-Raf leads to inactivation of MEK–MAPK
signalling. Mutations in TSC1 or TSC2 result in an activation cascade that includes GTP-loaded Rheb, Raptor-containing mTORC1, and p70S6K, and pathways that
upregulate IMPDH, SREBP, HIF-1α, VEGF-A, VEGF-C, VEGF-D, MMPs, and CatK; and inhibit 4E-BP1, ULK1, TFEB, and BCL2. Rictor-containing mTORC2 activates Akt,
ROCK–RhoA, and COX2. Oestrogen stimulates activation of MEK–MAPK and Akt. RTKs mediate activation of STAT and MEK–MAPK signalling. Dysregulated mTOR
signalling in LAM cells alters the processes shown in blue boxes and cell behaviours shown in red boxes. Agents studied in clinical trials are shown in bold.
4E-BP1=eukaryotic translation initiation factor 4E-binding protein 1. Akt=AKT serine–threonine protein kinase. BCL2=B-cell lymphoma 2. B-Raf=V-Raf murine sarcoma
viral oncogene homologue B1. CatK=cathepsin K. COX2=cyclooxygenase 2. FKBP38=FK506-binding protein 38. GAP=GTPase-activating protein. HIF-1α=hypoxia-
inducible factor 1α. IMPDH=inosine 5’-monophosphate dehydrogenase. LAM=lymphangioleiomyomatosis. MAPK=mitogen-activated protein kinase. MEK=MAPK
kinase. MMP=matrix metalloproteinase. mTOR=mechanistic target of rapamycin. mTORC1=mTOR complex 1. p70S6K=70 kDa ribosomal protein S6 kinase. Rheb=Ras
homologue enriched in brain. RhoA=Ras homologue family member A. ROCK=Rho-associated protein kinase. RTK=receptor tyrosine kinase. SREBP=sterol regulatory
element-binding protein. STAT=signal transducer and activator of transcription. TBC1D7=TBC1 domain family member 7. TFEB=transcription factor EB. TSC=tuberous
sclerosis complex. ULK1=Unc-51-like autophagy-activating kinase 1. VEGF=vascular endothelial growth factor.
survival and pulmonary metastasis of tuberin-null function decline in LAM is more rapid in premenopausal
cells in preclinical models,48,56–59 and phosphorylation of women and slows down after menopause,64 retrospective
pro-survival kinases MAPK and Akt in uterine leiomyoma- case series of anti-hormonal interventions have yielded
derived ELT3 cells from Eker rats60,61 and in cells derived conflicting results. The only randomised trial of an anti-
from patients with LAM (figure 1).35,58,62,63 Although lung oestrogen strategy in LAM showed that the aromatase
www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9 3
Review
inhibitor letrozole was safe in postmenopausal women, and asymptomatic, but those greater than 4 cm or
but the study underenrolled women and was not containing aneurysmal blood vessels are prone to
adequately powered to address questions of efficacy.65 haemorrhage.72 Large, multiple, and bilateral tumours
are more typical of TSC-LAM than sporadic LAM, and
Presentation and clinical features more rapid growth has been reported in patients with
Spontaneous pneumothorax in a woman in her fourth or large tumours and during pregnancy.73–75 Chronic
fifth decade of life, especially when recurrent, is a classic abdominal pain can occur, and a haemorrhage turning
presentation of LAM.66 The number of patients with into an angiomyolipoma can result in acute abdomen,
LAM who first seek medical attention for progressive life-threatening blood loss, and death.76
dyspnoea is almost equal to that of patients presenting Dyspnoea in LAM results from the replacement of
with pneumothorax, with the initial evaluation often lung parenchyma with cysts, airway narrowing due to
revealing an unremarkable chest radiograph and an reduced elastic recoil or direct involvement of airways,
obstructive defect on spirometry. Presentation with reactive airway disease, chylous congestion of the
dyspnoea is almost invariably initially interpreted as parenchyma, chylous effusions, or pneumothorax.
asthma or chronic obstructive pulmonary disease, and Pneumothoraces and chylothoraces in LAM are often
the diagnosis of LAM is often delayed for another refractory to conservative treatment and can recur even
3–5 years until suspicions are raised by the absence of a after well executed pleurodesis.77,78 The causes of
pattern of exacerbations and remissions, or lack of pleurodesis failure are unknown, but infiltration of
response to conventional therapy. Chylothorax is the pleura with LAM cells or prevention of close apposition
presenting manifestation in approxi mately 20% of of the visceral and parietal pleural surfaces by blebs
patients, and chylous ascites occurs in around 5% of might play a part. Infiltration of axial and mesenteric
patients.7 Additional atypical presentations include lymphatic tissues by LAM cells can lead to lymph
haemoptysis, abdominal pain due to angiomyolipoma adenopathy, thoracic duct enlargement and occlusion,
rupture or lymphangioleiomyoma distension, or appear lymphangioleiomyomas, or weeping masses of dys
ance of chyle in sputum, urine, stool, or vaginal plastic tissue (most often in the omentum), resulting
discharge. Increasingly, LAM and angiomyolipoma are in chylous pleural effusions and ascites.79,80 Chylous
discovered as incidental findings on imaging done for pericardial effusions, chyloptysis, and chyluria are also
other purposes. occasionally seen, often due to atypical communications
Regardless of the mode of presentation, a CT scan of between hollow viscera, airways, or potential spaces.
the chest that reveals diffuse, thin-walled cystic change is Abdominopelvic lymphatic disease can cause protein-
the key to correct diagnosis. For a definitive diagnosis, losing enteropathy, abdominal bloating, and distention
tissue or cytological confirmation is required, but a that sometimes worsens throughout the day due to
clinical diagnosis can be achieved with a compatible CT gravitational engorgement and increase in size of the
and at least one other accompanying feature, such as a lymphangioleiomyomas.81
diagnosis of TSC, an angiomyolipoma, elevated VEGF-D
(≥800 pg/mL), a chylous effusion, or a lymphangio Evaluation and diagnosis
leiomyoma.16,18 Doing a chest CT for patients presenting Diagnostic approach
with spontaneous pneumothorax to screen for the When cystic change compatible with LAM is found on
presence of underlying cystic lung diseases such as LAM, chest CT—whether identified by the screening of
Birt-Hogg-Dubé syndrome, and pulmonary Langerhans women with TSC or pneumothorax, revealed incidentally
cell histiocytosis has been shown to be cost-effective.67,68 on scans done for another purpose, or discovered during
We recommend CT screening for the first event of evaluation for recurrent pneumothorax, progressive
pneumothorax in women of childbearing age, for all dyspnoea, or chylous complications—the objective is to
women with recurrent pneumothorax or spontaneous exclude other diffuse cystic lung diseases in the differ
bilateral pneumothorax, and for those aged 18 years or ential and establish a diagnosis of LAM using the least
older with TSC.67,69,70 invasive means possible. The diseases that can mimic
Angiomyolipomas are benign mixed mesenchymal LAM radiologically include emphysema, Birt-Hogg-Dubé
tumours that are most often found in the kidneys but can syndrome, follicular bronchiolitis or lymphoid inter
occur in the liver, lung, bowel, bladder wall, and at other stitial pneumonia, amyloidosis, light-chain deposition
sites. Angiomyolipomas occur in around 30–40% of disease, and pulmonary Langerhans cell histiocytosis.
women with sporadic LAM and almost 90% of women Although a chest CT is not typically sufficient to defini
with TSC-LAM.7,8 Sporadic angiomyolipomas are tively distinguish between these entities,82 the radio
common in the general population, occurring as an logical characteristics of cysts—including distribution,
incidental finding in almost 1 in 100 abdominal CTs, and wall thickness, internal structure, and relationship to
have been associated with cystic pulmonary changes other structures—can provide helpful clues.
consistent with LAM in around 12% of patients in a Laboratory evaluation should include testing to rule out
referral population.71 Most of these tumours are small the following conditions: α1-antitrypsin deficiency, which
4 www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9
Review
can predispose patients to emphysema; connective pulmonary cysts are defined as spherical parenchymal
tissue diseases, which can be associated with follicular lucencies or low-attenuating areas with a well defined
bronchiolitis or lymphoid interstitial pneumonia (such boundary with normal appearing lung.88 LAM cysts
as rheumatoid factor, antinuclear antibodies, anti-Ro, are thin-walled, bilateral, diffusely distributed, round,
and anti-La); and lymphoproliferative disorders such as 2–30 mm in size, and typically devoid of internal
multiple myeloma (including serum and urine protein structure.16,18,74,87,89,90 Over time, cysts might coalesce and
electrophoresis and serum free light chains). A serum become polygonal or atypically shaped.87,89 Pulmonary
VEGF-D value greater than 800 pg/mL is reasonably cysts can occur as a normal consequence of ageing;91
sensitive and highly specific for the diagnosis of LAM. therefore, a minimum number of four cysts has been
A dedicated abdominopelvic CT to screen for lymph suggested as the threshold for considering a pathological
angioleiomyomas and renal and extrarenal angiomyo origin of cysts,69 and four71,92 or ten16 cysts as the threshold
lipomas should be considered, because identification of for establishing a diagnosis of LAM in patients with
these entities can obviate the need for biopsy. However, TSC.93
in some situations in which a firm diagnosis cannot be Other radiological features that might be identified on
established in a non-invasive way, a lung biopsy might be CT chest include focal ground-glass opacities, which
needed to guide treatment, especially in symptomatic occur secondary to proliferation of smooth muscle cells,
patients with substantial disease burden and those with pulmonary haemorrhage, lymphatic congestion (a form
atypical features suggestive of other causes. of interstitial pulmonary oedema), or alveolar filling
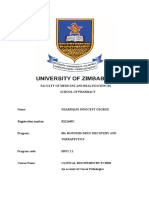
with lymphatic fluid (figure 2).89,94 Other thoracic
Pulmonary function testing lymphatic manifestations of LAM include septal
Pulmonary function tests are useful for determining thickening, chylothorax, pericardial effusion, thoracic
the severity of pulmonary dysfunction and for guiding duct dilatation, mediastinal lymph node enlargement,
therapy. LAM causes diffuse infiltration of the pulmonary and rarely, cystic lymphangioleiomyomas.77,89,95 Centri
interstitium with smooth muscle cells and cystic lobular nodules have also been reported, suspected to be
remodelling of the lung parenchyma, which have a manifestation of smooth muscle infiltration and
opposing effects on elastic recoil. Additionally, extensive macroscopic nodule formation.89 Features of multifocal
infiltration of the airways with LAM cells results in chronic micronodular pneumocyte hyperplasia, resulting from
inflammation, goblet cell hyperplasia, and squamous cell benign proliferation of type 2 alveolar epithelial cells,
metaplasia of the epithelium, all of which contribute to might occur in patients with TSC-LAM.96
increased airflow resistance and reversible airflow Several radiological features can help to distinguish
obstruction.83 These unique pathological features result in LAM from other diffuse cystic lung diseases.18,89 The
physiological patterns that are unusual among interstitial
lung diseases. Airflow obstruction is the most common A B C
physiological manifestation of LAM, but restrictive or
mixed patterns might also occur. Air trapping in the form
of elevated residual volume is often evident when
measured by plethysmography but not always by gas
dilution, suggesting poor communication between air
ways and cystic spaces,7 as confirmed by a hyperpolarised
¹²⁹Xe MRI study.84 Reversible airflow obstruction is D E F
present in approximately 20–30% of patients and has been
reported to correlate inversely with prognosis.64,85 Diffusion
capacity is reduced in up to 90% of patients7 and, along
with elevated residual volume, is often the first pulmonary
function abnormality that develops.
Radiological evaluation
Early in the disease course, the chest radiograph is often Figure 2: Radiological features of LAM
normal or might show features of a subtle increase (A) Chest radiograph showing a small-to-moderate right pneumothorax (arrow). (B) Axial CT of the thorax
in interstitial markings or a pleural effusion. As LAM showing scattered thin-walled pulmonary cysts with uniform shape. (C) Axial CT thorax showing diffuse cysts,
a large loculated left chylous pleural effusion, and smooth interlobular septal thickening secondary to lymphatic
progresses, reticular or nodular opacities, pleural thick congestion (arrow). Images A–C courtesy of David Murphy (St Vincent’s University Hospital, Dublin, Ireland).
ening, lymphadenopathy, or hyperinflation can appear.7,86 (D) MRI coronal maximum-intensity projection image of the abdomen and pelvis acquired with a heavily
A chronic or acute pneumothorax is occasionally T2-weighted sequence with fat suppression, showing a grossly dilated left pelvic sidewall and retroperitoneal
discovered as an incidental finding in asymptomatic lymphatics (arrows). (E) Axial CT image of the upper abdomen showing a large vascular fatty mass (arrow) arising
from the interpolar region of the right kidney and displacing abdominal and retroperitoneal structures compatible
patients (figure 2).87 with a large angiomyolipoma. (F) Hyperpolarised ¹²⁹Xe ventilation MRI image showing ventilation heterogeneity
Thin-walled cysts on chest CT are essential for the within pulmonary cysts. Image F courtesy of Laura Walkup (Cincinnati Children’s Hospital Medical Center,
diagnosis of pulmonary LAM (figure 2). Radiologically, OH, USA). LAM=lymphangioleiomyomatosis.
www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9 5
Review
lymphangioleiomyoma, or chylous effusion are not
A B present. A serum VEGF-D concentration of more than
800 pg/mL in the presence of characteristic cysts on CT is
associated with a sensitivity of approximately 60–70% and
specificity of nearly 100% for distinguishing LAM from
other cystic lung diseases, whereas concentrations greater
than 600 pg/mL have a sensitivity of 84% and specificity
of 98%.12,18,99 In a woman with a compatible chest CT, a
serum VEGF-D concentration of more than 800 pg/mL
obviates the need for lung biopsy, concentrations between
600–800 pg/mL are highly suspicious for LAM, and values
0 1 2 3 4 5 mm 0 0·2 0·4 0·6 0·8 1 mm of less than 600 pg/mL are considered uninformative and
do not exclude LAM. Commercially available VEGF-D
testing is offered in the USA, but ready access to
C D
standardised, quality-controlled, and third-party payer
reimbursable VEGF-D testing remains a global need.
Pathological evaluation
The decision to proceed to biopsy should be made jointly
by the physician and patient, and considered only when
minimally invasive measures have been unsuccessful
and the benefit of a diagnosis exceeds the risk.18 In
patients with mild disease, a clinical diagnosis of
probable LAM with regular monitoring might suffice,
0 20 40 60 80 100 μm especially if the care plan would not be altered by a
definite diagnosis and the patient is comfortable with a
Figure 3: Histopathological appearance of LAM degree of diagnostic uncertainty.16,18
(A) Low-power lung biopsy stained with haematoxylin and eosin showing cystic spaces and LAM nodules Although surgical lung biopsy was previously considered
interspersed with normal lung parenchyma. (B) Lung biopsy stained with α smooth muscle actin to highlight LAM the gold standard, transbronchial lung biopsy has been
nodules, which stain brown. Nodules appear within lung parenchyma (green arrow), surrounding cystic spaces
(red arrow), and within small lymphatics (blue arrow). (C) High-power view of a LAM nodule stained with PNL2
reported in a small series100 to have an estimated diagnostic
monoclonal antibody, showing LAM cells marked with granular cytoplasmic brown staining representing yield of more than 50%, and might be useful in some
pre-melanosomes (green arrow). (D) Dual immunostaining of a LAM nodule for the LAM cell marker cases. The yield and safety of transbronchial lung biopsy
glycoprotein 100 (brown) and the lymphatic endothelial marker podoplanin (blue), showing clefts lined by and the newer technique of transbronchial cryobiopsy
lymphatic endothelial cells within LAM nodules (green arrow). Immunostaining done by Suzanne Miller and
Debbie Clements (University of Nottingham, Nottingham, UK). Reproduced from Miller and colleagues,108
require further study. The diagnostic yield of surgical
by permission of John Wiley and Sons. LAM=lymphangioleiomyomatosis. lung biopsy is almost 100% and might be required to
distinguish between LAM, follicular bronchiolitis or
presence of nodules, upper lobe predominance, thicker lymphoid interstitial pneumonia, pulmonary Langerhans
cyst walls, atypical cyst shapes, and relative sparing of the cell histiocytosis, and amyloidosis or light-chain deposition
bases could indicate pulmonary Langerhans cell histio disease when less invasive methods are inadequate.
cytosis. Cysts in Birt-Hogg-Dubé syndrome are thin However, surgical lung biopsy is associated with risks of
walled, round or elliptical, predominant in the lower general anaesthesia, the potential for intraoperative
zone, often paramediastinal, and closely associated with pneumothorax, persistent air leak, and chronic chest pain
pleura and blood vessels, whereas those in follicular due to intercostal nerve compression.18
bronchiolitis or lymphoid interstitial pneumonia tend to Expert pathological consultation is a key component of
contain internal septae, are bordered by eccentric vessels, diagnosing LAM. LAM cells are spindle shaped or
and are more variable in size.97,98 Despite sensitivity epithelioid with few mitoses and a bland appearance.
and specificity for a LAM diagnosis of around 90%, These cells have features of smooth muscle that can be
characteristic cystic disease on CT alone is not considered identified by antibodies, including smooth muscle actin,
sufficiently diagnostic of LAM to support long-term and pre-melanocytic lineages identified by human
therapy with sirolimus.17,18,82 melanoma black (HMB-45) antibody.101 LAM cells also
express oestrogen receptors α and β and progesterone
Serum VEGF-D receptor.102,103 This unusual immunohistochemical profile
The 2016–17 American Thoracic Society and Japanese is seen in all perivascular epithelioid tumours, often
Respiratory Society clinical practice guidelines17,18 support termed PEComas, which in addition to LAM also
the use of serum VEGF-D as a diagnostic test when LAM include angiomyolipoma and clear cell tumours.104
is suspected in women with a compatible CT, even if other Immunostaining for HMB-45 is useful diagnostically
confirmatory features such as TSC, angiomyolipoma, especially when examining small samples such as
6 www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9
Review
transbronchial biopsies, although in rare cases, LAM
lesions do not express this marker.105 As the disease Clinical presentation and CT
features suggestive of LAM
progresses, lung cysts increase in number and LAM cells
form characteristic nodules and line the walls of cysts
and small airways.79 Hyperplastic alveolar type 2 cells are Detailed clinical review* confirms
Yes
Confirmed diagnosis
the presence of TSC of TSC-LAM
found lining cysts in a discontinuous manner and
surrounding LAM nodules.106 The stroma of LAM
nodules evolves to become more abundant and complex, No
comprising fibroblasts, T cells, and mast cells, such that
only a proportion (4–60%) of cells in the mature LAM
Abdominopelvic imaging Confirmed diagnosis
lesion contains TSC mutations.107,108 Lymphatic clefts (non-contrast CT or MRI) reveals of LAM
lined by LYVE1, podoplanin, and VEGFR3-positive angiomyolipomas or Yes
lymphangioleiomyomas
lymphatic endothelial cells are found in and around LAM
nodules (figure 3).109 Interactions between multiple cell
types within nodules are thought to facilitate LAM cell No
growth and survival, and the production of tissue-
damaging proteases.110–113 A stepwise algorithm to guide
the diagnosis of LAM in patients with compatible clinical Serum VEGF-D concentration Confirmed diagnosis
Yes
≥800 pg/mL of LAM
presentation and chest CT findings is shown in figure 4.
The management of LAM is shown in the table.
No
Pharmacological treatment
mTORC1 inhibitors Confirmation of chyle by chemical Confirmed diagnosis
Discovery of the central role of activated mTORC1 analysis in patients with pleural of LAM
signalling in LAM pathogenesis formed the basis for effusions or ascites, or both, or
Yes
the presence of LAM cells by
trials of the mTORC1 inhibitor sirolimus (rapamycin) as cytological examination of
a potential treatment for LAM. In an open-label pilot effusions or lymph node aspirates
study9 in patients with TSC or LAM, the use of sirolimus
for 12 months led to an almost 50% reduction in No
angiomyolipoma size (n=20) and an improvement in
FEV1 and forced vital capacity (FVC), along with a
reduction in residual volume in patients with LAM (n=11). Is there a need to obtain Probable diagnosis
histopathological confirmation of LAM; serial PFT
These results led to the pivotal MILES trial (NCT00414648), on the basis of symptom severity, No monitoring done to
a randomised, double-blind, placebo-controlled, phase 3 disease extent on CT or PFTs, or assess disease
both, and patient preferences? progression
trial in which 89 women with LAM and abnormal lung
function (percentage of predicted FEV1 ≤70%) were
assigned (1:1) to receive sirolimus or placebo for Yes
12 months followed by 12 months of off-treatment
observation. During the 12-month treatment period, FEV1
Lung biopsy done; we suggest a Confirmed diagnosis
declined at a rate of –12 mL (SD 2 mL) per month in the stepwise approach, with of LAM
placebo group and increased by 1 mL (SD 2 mL) transbronchial biopsy considered
before a VATS-guided lung biopsy
per month in the treatment group (p<0·001). Treatment
with sirolimus also led to an improvement in the FVC
slope and in overall quality of life, and a reduction in Figure 4: Methods for the diagnosis of LAM
Methods presented from least (top) to most (bottom) invasive. *Includes
serum VEGF-D concentrations compared with placebo. detailed family history for TSC and seizures or cognitive impairment, physical
During off-treatment observation, the FEV1 decline examination focused on facial angiofibromas, subungual fibromas, shagreen
resumed in the sirolimus group at a similar rate to that of patches, dental pitting, hypomelanotic macules, confetti lesions, and imaging
the placebo group. These results indicate that sirolimus is review for the presence of cortical dysplasias, subependymal nodules,
and subependymal giant cell astrocytomas. LAM=lymphangioleiomyomatosis.
an effective suppressive treatment for LAM that stabilises PFT=pulmonary function test. TSC=tuberous sclerosis complex.
lung function decline while the therapy continues, but VATS=video-assisted thoracoscopic surgery. VEGF-D=vascular endothelial
that disease progression resumes upon cessation of growth factor D.
treatment.11
The beneficial effect of sirolimus and another mTORC1 Sirolimus was also shown to be helpful in managing
inhibitor, everolimus, in patients with LAM has been lymphatic manifestations of LAM, such as chylous
reported in multiple other studies.118,119,135–142 Although not effusions and lymphangioleiomyomas.18,118,119 Questions
studied as rigorously, everolimus appears to have similar about the long-term safety and efficacy of sirolimus for
efficacy to sirolimus in the management of LAM.135 LAM await results from the MIDAS Registry
www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9 7
Review
Considerations Management options and indication
Pneumothorax18,77,78,114,115 High rate of recurrent pneumothorax Video-assisted thoracoscopic surgery-guided mechanical pleurodesis after first
pneumothorax; chemical pleurodesis, talc pleurodesis, or pleurectomy for recurrent or
refractory pneumothorax
Angiomyolipoma9,69,72,116,117 Risk of haemorrhage in large angiomyolipomas Surveillance imaging every 12–24 months (angiomyolipomas <3 cm); mTORC1
inhibitors (angiomyolipomas >3 cm), especially in patients with significant
concomitant pulmonary disease or with multiple, bilateral or symptomatic, growing
angiomyolipomas; embolisation, especially for single lesion with high burden of
aneurysmal vessels, if refractory to mTORC1 inhibitors, or if sole indication for
mTORC1 inhibitors; surgical resection for large, complex lesions refractory to mTORC1
inhibitors or if concern for malignant transformation (nephron-sparing surgeries
preferred, total nephrectomy as a last resort)
Lymphatic Pleural drainage might be needed to relieve dyspnoea or abdominal mTORC1 inhibitors as preferred first-line treatment; lymphatic imaging and thoracic
complications17,118–120 distension from large effusions; mTORC1 inhibitors might take several duct embolisation for recurrent or refractory cases
months for full effect
End-stage respiratory Discuss with transplant team, consider continued mTORC1 inhibitor use or Lung transplantation for end-stage respiratory failure, as defined by one of the
failure121–126 switching to mTORC1 inhibitor with shorter half-life such as everolimus following: FEV1% predicted of 30% or less, resting hypoxaemia, progressive lung
while on transplant waiting list; stop treatment immediately before function decline, New York Heart Association functional class 4
transplantation; previous pleurodesis should not be considered a
contraindication for lung transplantation
Vaccinations127–129 Avoid live vaccines in patients taking mTORC1 inhibitors Annual influenza vaccination with inactivated vaccine, pneumococcal vaccination
with PCV13 and PPSV23 for all patients with LAM; herpes zoster vaccination with
recombinant zoster vaccine for patients >50 years or those on mTORC1 inhibitors
(regardless of age)
Pulmonary rehabilitation130 Shown to improve exercise capacity, 6-min walk distance, and quality of life Pulmonary rehabilitation programme an option in patients with reduced physical
activity
Supplemental oxygen Required in patients with hypoxia Ambulatory oxygen or long-term oxygen therapy (resting room air PaO2 <7·3 kPa and
SpO2 desaturation with exercise or sleep)
Pregnancy52,55,131,132 Often associated with accelerated disease progression and increased risk of Counselling for all patients with LAM about potential risks; genetic counselling for
spontaneous pneumothorax prospective mothers with TSC-LAM; mTORC1 inhibitors withheld before conception
and throughout pregnancy; close monitoring of patients with LAM during pregnancy
Bone density16,133,134 Low bone mineral density is prevalent in patients with LAM Dual-energy x-ray absorptiometry scan done periodically; treatment for low bone
mineral density as per guidelines in all postmenopausal patients, those with
substantial impairment in mobility, and those receiving anti-oestrogen agents
LAM=lymphangioleiomyomatosis. mTORC1= mechanistic target of rapamycin complex 1. PaO2=partial pressure of arterial oxygen. SpO2=blood oxygen saturation. TSC=tuberous sclerosis complex.
Table: Management considerations in patients with LAM
(NCT02432560), but a 2014 US National Institutes of common in the first 6 months of therapy and decrease
Health report of 12 patients who received long-term over time.14,136,137,140 In the MILES trial, sirolimus was
sirolimus therapy indicated that the drug has durable started at 2 mg per day and the dose was titrated to
efficacy and an acceptable safety prolife during 5-year maintain a blood trough of 5–15 ng/mL, with a
follow-up.139 The American Thoracic Society and Japanese mean sirolimus trough concentration of 7·2 ng/mL.11,14
Respiratory Society clinical practice guidelines recom Subsequent studies136,119 have suggested that lower doses
mend using sirolimus as first-line treatment for patients of sirolimus might have similar treatment efficacy and a
with LAM who meet at least one of the following criteria: reduced incidence of adverse events, but one study143
percentage of predicted FEV1 of 70% or less, chylous found better treatment response with higher sirolimus
complications, rapidly declining lung function (FEV1 doses. Further investigation is required to define the
decline ≥90 mL per year), or other measures suggesting optimal sirolimus dosing strategy for patients with LAM
substantial disease burden such as abnormal diffusion that maximises efficacy and balances the risk of adverse
capacity, air trapping, hyperinflation, or the need for events.
supplemental oxygen.17 Sirolimus is approved for the
treatment of LAM by the US Food and Drug Adminis Other pharmacological agents
tration, the European Medicines Agency, and regulatory Reversible airflow obstruction can be seen in approximately
agencies in multiple other countries such as Japan, 20% of patients with LAM,7,144 and a therapeutic trial of
South Korea, Brazil, Russia, and Uruguay. bronchodilators should be considered for symptomatic
In general, sirolimus is a well tolerated drug with a patients, especially those with an obstructive defect on
favourable side-effect profile. The most common adverse spirometry.16 Doxycycline is active against several matrix
events related to sirolimus in the MILES trial were metalloproteinases,145 and was believed to be a promising
nausea, diarrhoea, mucositis, acne, lower-extremity drug for LAM on the basis of a 2006 case report.146 However,
swelling, and hyperlipidaemia.11 Adverse events are most subsequent investigations did not show a beneficial
8 www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9
Review
effect,147–150 and routine use of doxycycline in LAM is not Lymphatic involvement
recommended.18 Owing to the female predominance of The most common lymphatic complications encountered
LAM, the slowing of lung function decline after in patients with LAM include the following: lymphaden
menopause, and reports of disease worsening with opathy; lymphangioleiomyomas of the pelvis, abdomen,
exogenous oestrogen supplemen tation,53 several hor- or mediastinum; and chylous fluid collections in pleural
monal agents such as selective oestrogen receptor or peritoneal cavities. Drainage procedures might be
modulators,66,151 progesterone,51,66,131,152,153 aromatase inhib needed to confirm the chylous nature of the fluid at initial
itors,65 gonadotropin-releasing hormone agonists,154–156 and presentation or to relieve dyspnoea from large effusions;
surgical procedures such as oophorectomy66,131,157–159 have however, cystic lymphangioleiomyomas generally should
been attempted as potential treatments for LAM with not be biopsied, drained, or resected given the risk of
inconsistent and often inconclusive results. Currently, inducing a chronic leak. Sirolimus was shown to be
anti-oestrogen treatments are not recommended outside effective at reducing chylous accumulation,118–120 and is
of clinical trials, although further studies including the preferred first-line treatment option for chylous
combination therapies with mTORC1 inhibitors and anti- complications in LAM rather than invasive procedures.17
oestrogen agents are warranted.16,18 Early-stage investi Notably, in some patients sirolimus might take several
gations of statins,160 hydroxychloroquine,161 and celecoxib162 months to be effective for chylous indications. Invasive
in LAM have been published, but larger studies are needed options such as thoracic duct embolisation should be
to determine their clinical effects. Exciting new data from reserved for recurrent or refractory cases and considered
cell and animal models suggest that immune checkpoint only if the source of the leak is identified through
inhibitors and purine and pyrimidine nucleotide ana specialised lymphatic imaging techniques.168
logues might have the potential to induce LAM cell death.41
Pregnancy and LAM
Spontaneous pneumothorax Pregnancy in patients with LAM has been associated with
Patients with LAM should be informed about the signs accelerated disease progression and increased incidence
and symptoms of pneumothorax and counselled to seek of spontaneous pneumothorax.52,55,131,132 Uneventful preg
medical attention promptly if symptoms develop. Given nancies have also been reported.77 In an analysis
the high rate of pneumothorax recurrence after con involving 16 pregnant patients with LAM who had lung
servative treatment,77,78,114,115 pleurodesis is recommended function data available for the pre-pregnancy and
with the first episode of spontaneous pneumothorax post-pregnancy periods, accelerated rate of decline in
rather than during recurrent events.18 Pleurodesis can FEV1 and diffusing capacity of the lungs for carbon
reduce the 70% risk of recurrence with conservative monoxide (DLCO) was noted during and after pregnancy
treatment to around 30%.78 Video-assisted thoracoscopic in most patients. A third of patients (five of 16) had
surgery-guided mechanical abrasion is generally the spontaneous pneumothorax during pregnancy.52 Patients
preferred method for initial pleurodesis, with chemical with LAM who are considering becoming pregnant
pleurodesis using agents such as talc reserved for should be counselled about the potential risks, which
recurrent or refractory episodes.18 Another technique depend partly on the pulmonary reserves of the mother.169
that has been used successfully to prevent recurrent Although not known to be teratogenic, in animal models,
pneumothoraces is total pleural covering, in which the sirolimus has been associated with intrauterine fetal
visceral pleural surface is reinforced with a bioabsorbable demise and is excreted in breastmilk. Safe use of
mesh.163 However, this technique is currently available sirolimus throughout pregnancy has been reported in
only at select centres in Japan and requires specialised patients who had a renal transplant and in at least one
technical expertise, limiting its generalised application. patient with LAM;170,171 however, the long-term safety and
Although not yet studied rigorously, treatment with efficacy of sirolimus for mother and child requires
sirolimus might help to reduce the risk of recurrent further investigation.
pneumothoraces.164 Notably, because of the delayed
wound healing associated with sirolimus, stopping the Lung transplantation
drug for 2–4 weeks after the resolution of a pneumo Lung transplantation is a viable management option for
thorax before reinitiating might be prudent. The patients with LAM and end-stage disease. Outcomes after
atmospheric pressure changes associated with air travel lung transplantation are similar to121–123 or better than124–126
might cause expansion of pulmonary cysts and lead to post-transplant outcomes in other chronic pulmonary
spontaneous pneumothorax in patients with LAM, with conditions. In a 2019 analysis, Khawar and colleagues126
a risk that has been estimated to range from one to evaluated outcomes in 134 patients with LAM who had a
two episodes per 100 flights.115,165,166 Although patients lung transplant in the USA between 2003 and 2017, and
should be counselled regarding this risk and the reported a remarkable median post-transplant survival of
potential need for supplemental oxygen in flight, most 12 years, with a survival rate of 94% at 1 year, 73% at
LAM clinicians do not recommend restricting air 5 years, and 55% at 10 years. Previous pleurodesis is
travel.167 not a contraindication for lung transplantation.18,172 Use
www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9 9
Review
of sirolimus in the immediate post-operative period Elevated baseline serum VEGF-D concentrations are
following lung transplantation has been associated linked to faster disease progression in some studies13,14,179
with increased risk of dehiscence of the bronchial but not others.64,180–182 Similarly, a positive response to
anastomosis.173 However, premature discontinuation of bronchodilators has been linked to faster disease
sirolimus before transplantation can put patients at progression,64,85 although this association was not seen
risk of precipitous lung function decline. Given that in the MILES trial.14 Neither baseline FEV114,51,64 nor the
most cases of bronchial dehiscence occur 4–6 weeks presence or number of spontaneous pneumothoraces64
post-transplantation, after the sirolimus wash-out period seems to have a significant effect on future rate of
(<1 week), some centres have adopted a policy of decline in FEV1.
continuing sirolimus until the day of surgery, or a change The median survival of patients with LAM is estimated
to an mTORC1 inhibitor with a shorter half-life, such as at more than 20 years after diagnosis,64,183 with a transplant-
everolimus, upon placement on the waiting list.174,175 free survival probability of 94% at 5 years, 85% at 10 years,
75% at 15 years, and 64% at 20 years.64 In general, these
Natural history and prognosis estimates represent an overall improvement in prognosis
LAM is a gradually progressive disease with over half of compared with earlier reports,66,184 probably because of
patients estimated to have MRC grade 3 dyspnoea (when increased awareness of LAM and identification earlier in
walking on a level surface) 10 years after symptom the disease course. Premenopausal status,64 abnormal
onset,176 although these data were collected before the baseline lung function (FEV1 and DLCO),64 lower
routine use of mTORC1 inhibitors as therapy. The rate of FEV1:FVC ratio,184 presentation with dyspnoea (as opposed
decline in FEV1 in patients with LAM is variable (range to pneumothorax),185 a worse histology score,186 and the
47–134 mL per year).11,51,64,152,131,177,178 In a prospective, need for supplemental oxygen183 have all been linked to
longitudinal analysis of 230 patients with LAM enrolled lower survival in LAM.
in the US National Heart, Lung, and Blood Institute Although TSC-LAM is believed to represent a milder
(NHLBI) LAM Registry, the mean rate of decline in FEV1 lung disease than sporadic LAM, guideline-directed
was 89 mL (SD 53 mL) per year.64 screening of young adult females with TSC identifies
Premenopausal women with LAM have a faster rate of early disease, which probably leads to ascertainment
decline in FEV1 than do postmenopausal women.14,51,64,152,177 bias.69 In a NHLBI cohort study8 in which patients with
In a post-hoc analysis of the placebo cohort from the TSC-LAM and sporadic LAM were matched for disease
MILES trial, FEV1 in premenopausal women declined severity, the rates of decline in FEV1 were similar in
approximately five-times faster than in postmenopausal both groups. Similar conclusions were reached by a
women (approximately 200 mL per year vs 40 mL post-hoc analysis of participants in the MILES trial14
per year; p=0·003).14 Similarly, the rate of decline in and in a Brazilian cohort of patients with an incidental
FEV1 in the NHLBI cohort was 44 mL per year lower in diagnosis of LAM, an approach that was not confounded
post
menopausal women than in premenopausal by the selection bias posed by screening.187 LAM can be
women (74 mL per year vs 118 mL per year; p=0·003).64 a substantial cause of mortality in patients with TSC; in
a retrospective analysis of a large tertiary care referral
centre for TSC, LAM was reported as the second most
Search strategy and selection criteria common cause of death in adults overall and the
We searched MEDLINE and PubMed from database inception leading cause of death among adult women with TSC.188
to April 28, 2021, for reviews and original research papers The effect of sirolimus on overall survival and the
about lymphangioleiomyomatosis, published in English. likelihood of progression to lung transplantation is not
We used the terms “lymphangioleiomyomatosis”, “LAM”, yet known.
and “lymphangiomyomatosis” in combination with
“pathogenesis”, “diagnosis”, and “treatment”. We also Conclusions
searched individual terms such as “mTOR inhibitors”, Rapid advances in understanding and management, and
“tuberous sclerosis complex”, “sirolimus”, “rapamycin”, improved outcomes in LAM can be attributed in part to
“angiomyolipoma”, “lymphangioleiomyoma”, “chylothorax”, the foresight of patients who have collaborated in a
and “lung transplantation”. We focused on studies published manner that has facilitated research and clinical trials.
in the past 20 years, although we did not exclude earlier Close interactions between investigators and patients in
reports, especially if they were unique or high-quality clinical scientific meetings, grassroots fundraising to support
trials. We also searched the reference lists of articles identified pilot studies, and distribution of expertise across multiple
using this search and our own personal files. We used original centres have been key to progress. Lessons learned from
reports where available, with the aim of highlighting the the study of the mTOR pathway in TSC and LAM have
most important advances in the field and providing a led to fundamental advances in our understanding of
comprehensive overview of pathogenesis, diagnosis, cellular metabolism and contributed to interest in the
and management. use of mTOR inhibitors in other lung diseases, such
as sarcoidosis, diffuse idiopathic neuroendocrine cell
10 www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9
Review
hyperplasia, Castleman disease, and COVID-19. Future 12 Young LR, Inoue Y, McCormack FX. Diagnostic potential of serum
research goals include generating cell and animal models VEGF-D for lymphangioleiomyomatosis. N Engl J Med 2008;
358: 199–200.
of LAM that more accurately recapitulate the human 13 Young L, Lee HS, Inoue Y, et al. Serum VEGF-D a concentration as
disease, understanding the role of the immune system in a biomarker of lymphangioleiomyomatosis severity and treatment
LAM pathogenesis and therapy, and further defining how response: a prospective analysis of the Multicenter International
Lymphangioleiomyomatosis efficacy of sirolimus (MILES) trial.
mTORC1 activation promotes cell growth and metastasis. Lancet Respir Med 2013; 1: 445–52.
The next steps in LAM therapeutic development are to 14 Gupta N, Lee HS, Young LR, et al. Analysis of the MILES cohort
refine the approach to mTORC1 inhibitor use, including reveals determinants of disease progression and treatment
response in lymphangioleiomyomatosis. Eur Respir J 2019;
optimal dosing and cytolytic combination therapies; 53: 1802066.
to harness understanding of disease mechanisms to 15 Guo M, Yu JJ, Perl AK, et al. Single-cell transcriptomic analysis
develop more powerful diagnostic, prognostic, and pre identifies a unique pulmonary lymphangioleiomyomatosis cell.
Am J Respir Crit Care Med 2020; 202: 1373–87.
dictive biomarkers; and to explore novel approaches to
16 Johnson SR, Cordier JF, Lazor R, et al. European Respiratory
trial design for the development of remission-inducing Society guidelines for the diagnosis and management of
therapies. lymphangioleiomyomatosis. Eur Respir J 2010; 35: 14–26.
17 McCormack FX, Gupta N, Finlay GR, et al. Official American
Contributors Thoracic Society/Japanese Respiratory Society Clinical Practice
All authors conceptualised and planned the Review, and prepared the guidelines: lymphangioleiomyomatosis diagnosis and
figures and table. All authors contributed equally to the writing and management. Am J Respir Crit Care Med 2016; 194: 748–61.
revision of this Review. 18 Gupta N, Finlay GA, Kotloff RM, et al. Lymphangioleiomyomatosis
Declaration of interests diagnosis and management: high-resolution chest computed
CM, NG, SRJ, and FXM are scientific advisory board members of the LAM tomography, transbronchial lung biopsy, and pleural disease
management. An official American Thoracic Society/Japanese
Foundation. CM reports grants (LAM0144SG01-20) from the LAM
Respiratory Society clinical practice guideline.
Foundation, which did not influence the content of this Review. Am J Respir Crit Care Med 2017; 196: 1337–48.
SRJ reports grants from the UK Medical Research Council, LAM Action,
19 Harknett EC, Chang WY, Byrnes S, et al. Use of variability in
the LAM Foundation, and the Tuberous Sclerosis Association; and a grant national and regional data to estimate the prevalence of
from Pfizer for post-marketing surveillance on rapamycin, outside the lymphangioleiomyomatosis. Q JM 2011; 104: 971–79.
submitted work. FXM reports grants from National Institutes of Health 20 Ryu JH, Sykes AM, Lee AS, Burger CD. Cystic lung disease is not
(NIH; U01HL131755, U01HL131022). JJY reports grants from NIH uncommon in men with tuberous sclerosis complex. Respir Med
National Heart, Lung, and Blood Institute (RO1HL153045, R01HL138481), 2012; 106: 1586–90.
the US Department of Defense (W81XWH1910474, 81XWH2010736), 21 Adriaensen ME, Schaefer-Prokop CM, Duyndam DA,
and The LAM Foundation (LAM0141E01-20). NG reports grants from NIH Zonnenberg BA, Prokop M. Radiological evidence of
(U01HL131755, R34HL138235) and the LAM Foundation. lymphangioleiomyomatosis in female and male patients with
tuberous sclerosis complex. Clin Radiol 2011; 66: 625–28.
References
1 Johnson SR. Lymphangioleiomyomatosis. Eur Respir J 2006; 22 Aubry MC, Myers JL, Ryu JH, et al. Pulmonary
27: 1056–65. lymphangioleiomyomatosis in a man. Am J Respir Crit Care Med
2000; 162: 749–52.
2 McCormack FX, Travis WD, Colby TV, Henske EP, Moss J.
Lymphangioleiomyomatosis: calling it what it is: a low-grade, 23 Schiavina M, Di Scioscio V, Contini P, et al. Pulmonary
destructive, metastasizing neoplasm. Am J Respir Crit Care Med lymphangioleiomyomatosis in a karyotypically normal man without
2012; 186: 1210–12. tuberous sclerosis complex. Am J Respir Crit Care Med 2007;
176: 96–98.
3 Gupta N, Vassallo R, Wikenheiser-Brokamp KA, McCormack FX.
Diffuse cystic lung disease. Part I. Am J Respir Crit Care Med 2015; 24 Han MK, Tyburczy ME, Darling TN, et al. Apparent sporadic
191: 1354–66. lymphangioleiomyomatosis in a man as a result of extreme
mosaicism for a TSC2 mutation. Ann Am Thorac Soc 2017;
4 Moss J, Avila NA, Barnes PM, et al. Prevalence and clinical
14: 1227–29.
characteristics of lymphangioleiomyomatosis (LAM) in patients
with tuberous sclerosis complex. Am J Respir Crit Care Med 2001; 25 Garami A, Zwartkruis FJ, Nobukuni T, et al. Insulin activation of
164: 669–71. Rheb, a mediator of mTOR/S6K/4E-BP signaling, is inhibited by
TSC1 and 2. Mol Cell 2003; 11: 1457–66.
5 Costello LC, Hartman TE, Ryu JH. High frequency of pulmonary
lymphangioleiomyomatosis in women with tuberous sclerosis 26 Stocker H, Radimerski T, Schindelholz B, et al. Rheb is an essential
complex. Mayo Clin Proc 2000; 75: 591–94. regulator of S6K in controlling cell growth in Drosophila.
Nat Cell Biol 2003; 5: 559–65.
6 Franz DN, Brody A, Meyer C, et al. Mutational and radiographic
analysis of pulmonary disease consistent with 27 Dibble CC, Elis W, Menon S, et al. TBC1D7 is a third subunit of the
lymphangioleiomyomatosis and micronodular pneumocyte TSC1-TSC2 complex upstream of mTORC1. Mol Cell 2012;
hyperplasia in women with tuberous sclerosis. 47: 535–46.
Am J Respir Crit Care Med 2001; 164: 661–68. 28 Dodd KM, Yang J, Shen MH, Sampson JR, Tee AR. mTORC1 drives
7 Ryu JH, Moss J, Beck GJ, et al. The NHLBI HIF-1α and VEGF-A signalling via multiple mechanisms involving
lymphangioleiomyomatosis registry: characteristics of 230 patients 4E-BP1, S6K1 and STAT3. Oncogene 2015; 34: 2239–50.
at enrollment. Am J Respir Crit Care Med 2006; 173: 105–11. 29 Valvezan AJ, Turner M, Belaid A, et al. mTORC1 couples nucleotide
8 Taveira-DaSilva AM, Jones AM, Julien-Williams P, Yao J, Stylianou M, synthesis to nucleotide demand resulting in a targetable metabolic
Moss J. Severity and outcome of cystic lung disease in women with vulnerability. Cancer Cell 2017; 32: 624–638.e5.
tuberous sclerosis complex. Eur Respir J 2015; 45: 171–80. 30 Ma D, Bai X, Zou H, Lai Y, Jiang Y. Rheb GTPase controls apoptosis
9 Bissler JJ, McCormack FX, Young LR, et al. Sirolimus for by regulating interaction of FKBP38 with Bcl-2 and Bcl-XL.
angiomyolipoma in tuberous sclerosis complex or J Biol Chem 2010; 285: 8621–27.
lymphangioleiomyomatosis. N Engl J Med 2008; 358: 140–51. 31 Mutvei AP, Nagiec MJ, Hamann JC, Kim SG, Vincent CT, Blenis J.
10 Davies DM, Johnson SR, Tattersfield AE, et al. Sirolimus therapy in Rap1-GTPases control mTORC1 activity by coordinating lysosome
tuberous sclerosis or sporadic lymphangioleiomyomatosis. organization with amino acid availability. Nat Commun 2020;
N Engl J Med 2008; 358: 200–03. 11: 1416.
11 McCormack FX, Inoue Y, Moss J, et al. Efficacy and safety of 32 Jacinto E, Facchinetti V, Liu D, et al. SIN1/MIP1 maintains rictor-
sirolimus in lymphangioleiomyomatosis. N Engl J Med 2011; mTOR complex integrity and regulates Akt phosphorylation and
364: 1595–606. substrate specificity. Cell 2006; 127: 125–37.
www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9 11
Review
33 Sarbassov DD, Ali SM, Kim DH, et al. Rictor, a novel binding 55 Cohen MM, Freyer AM, Johnson SR. Pregnancy experiences among
partner of mTOR, defines a rapamycin-insensitive and raptor- women with lymphangioleiomyomatosis. Respir Med 2009;
independent pathway that regulates the cytoskeleton. Curr Biol 103: 766–72.
2004; 14: 1296–302. 56 Li C, Zhou X, Sun Y, et al. Faslodex inhibits estradiol-induced
34 Goncharova EA, Goncharov DA, Li H, et al. mTORC2 is required extracellular matrix dynamics and lung metastasis in a model of
for proliferation and survival of TSC2-null cells. Mol Cell Biol 2011; lymphangioleiomyomatosis. Am J Respir Cell Mol Biol 2013;
31: 2484–98. 49: 135–42.
35 Li C, Lee PS, Sun Y, et al. Estradiol and mTORC2 cooperate to 57 Liu F, Lunsford EP, Tong J, et al. Real-time monitoring of
enhance prostaglandin biosynthesis and tumorigenesis in tumorigenesis, dissemination, & drug response in a preclinical
TSC2-deficient LAM cells. J Exp Med 2014; 211: 15–28. model of lymphangioleiomyomatosis/tuberous sclerosis complex.
36 Ben-Sahra I, Hoxhaj G, Ricoult SJH, Asara JM, Manning BD. PLoS One 2012; 7: e38589.
mTORC1 induces purine synthesis through control of the 58 Sun Y, Zhang E, Lao T, et al. Progesterone and estradiol synergistically
mitochondrial tetrahydrofolate cycle. Science 2016; 351: 728–33. promote the lung metastasis of tuberin-deficient cells in a preclinical
37 Ben-Sahra I, Manning BD. mTORC1 signaling and the metabolic model of lymphangioleiomyomatosis. Horm Cancer 2014; 5: 284–98.
control of cell growth. Curr Opin Cell Biol 2017; 45: 72–82. 59 Yu JJ, Robb VA, Morrison TA, et al. Estrogen promotes the survival
38 Hoxhaj G, Hughes-Hallett J, Timson RC, et al. The mTORC1 and pulmonary metastasis of tuberin-null cells.
signaling network senses changes in cellular purine nucleotide Proc Natl Acad Sci USA 2009; 106: 2635–40.
levels. Cell Rep 2017; 21: 1331–46. 60 Finlay GA, Thannickal VJ, Fanburg BL, Kwiatkowski DJ. Platelet-
39 Ricoult SJ, Yecies JL, Ben-Sahra I, Manning BD. Oncogenic PI3K derived growth factor-induced p42/44 mitogen-activated protein
and K-Ras stimulate de novo lipid synthesis through mTORC1 and kinase activation and cellular growth is mediated by reactive oxygen
SREBP. Oncogene 2016; 35: 1250–60. species in the absence of TSC2/tuberin. Cancer Res 2005;
40 Maisel K, Merrilees MJ, Atochina-Vasserman EN, et al. Immune 65: 10881–90.
checkpoint ligand PD-L1 is upregulated in pulmonary 61 Finlay GA, York B, Karas RH, et al. Estrogen-induced smooth
lymphangioleiomyomatosis. Am J Respir Cell Mol Biol 2018; muscle cell growth is regulated by tuberin and associated with
59: 723–32. altered activation of platelet-derived growth factor receptor-beta and
41 Liu H-J, Lizotte PH, Du H, et al. TSC2-deficient tumors have ERK-1/2. J Biol Chem 2004; 279: 23114–22.
evidence of T cell exhaustion and respond to anti-PD-1/anti-CTLA-4 62 Gu X, Yu JJ, Ilter D, Blenis N, Henske EP, Blenis J. Integration of
immunotherapy. JCI Insight 2018; 3: 98674. mTOR and estrogen-ERK2 signaling in lymphangioleiomyomatosis
42 Osterburg AR, Nelson RL, Yaniv BZ, et al. NK cell activating pathogenesis. Proc Natl Acad Sci USA 2013; 110: 14960–65.
receptor ligand expression in lymphangioleiomyomatosis is 63 Sun Y, Gu X, Zhang E, et al. Estradiol promotes pentose phosphate
associated with lung function decline. JCI Insight 2016; 1: e87270. pathway addiction and cell survival via reactivation of Akt in
43 Bittmann I, Rolf B, Amann G, Löhrs U. Recurrence of mTORC1 hyperactive cells. Cell Death Dis 2014; 5: e1231.
lymphangioleiomyomatosis after single lung transplantation: 64 Gupta N, Lee HS, Ryu JH, et al. The NHLBI LAM registry:
new insights into pathogenesis. Hum Pathol 2003; 34: 95–98. prognostic physiologic and radiologic biomarkers emerge from a
44 Karbowniczek M, Astrinidis A, Balsara BR, et al. Recurrent 15-year prospective longitudinal analysis. Chest 2019; 155: 288–96.
lymphangiomyomatosis after transplantation: genetic analyses 65 Lu C, Lee HS, Pappas GP, et al. A phase II clinical trial of an
reveal a metastatic mechanism. Am J Respir Crit Care Med 2003; aromatase inhibitor for postmenopausal women with
167: 976–82. lymphangioleiomyomatosis. Ann Am Thorac Soc 2017; 14: 919–28.
45 Carsillo T, Astrinidis A, Henske EP. Mutations in the tuberous 66 Taylor JR, Ryu J, Colby TV, Raffin TA. Lymphangioleiomyomatosis.
sclerosis complex gene TSC2 are a cause of sporadic pulmonary Clinical course in 32 patients. N Engl J Med 1990; 323: 1254–60.
lymphangioleiomyomatosis. Proc Natl Acad Sci USA 2000; 67 Gupta N, Langenderfer D, McCormack FX, Schauer DP,
97: 6085–90. Eckman MH. Chest computed tomographic image screening for
46 Hayashi T, Kumasaka T, Mitani K, et al. Prevalence of uterine and cystic lung diseases in patients with spontaneous pneumothorax is
adnexal involvement in pulmonary lymphangioleiomyomatosis: cost effective. Ann Am Thorac Soc 2017; 14: 17–25.
a clinicopathologic study of 10 patients. Am J Surg Pathol 2011; 68 Cattran A, Meganathan K, Gupta N. Epidemiology and healthcare
35: 1776–85. utilization of spontaneous pneumothorax and diffuse cystic lung
47 Prizant H, Hammes SR. Minireview: lymphangioleiomyomatosis diseases in the United States. Ann Am Thorac Soc 2021; 18: 534–36.
(LAM): the “other” steroid-sensitive cancer. Endocrinology 2016; 69 Krueger DA, Northrup H, Northrup H, et al. Tuberous sclerosis
157: 3374–83. complex surveillance and management: recommendations of the
48 Prizant H, Sen A, Light A, et al. Uterine-specific loss of Tsc2 leads 2012 International Tuberous Sclerosis Complex Consensus
to myometrial tumors in both the uterus and lungs. Mol Endocrinol conference. Pediatr Neurol 2013; 49: 255–65.
2013; 27: 1403–14. 70 Hagaman JT, Schauer DP, McCormack FX, Kinder BW. Screening
49 Logginidou H, Ao X, Russo I, Henske EP. Frequent estrogen and for lymphangioleiomyomatosis by high-resolution computed
progesterone receptor immunoreactivity in renal angiomyolipomas tomography in young, nonsmoking women presenting with
from women with pulmonary lymphangioleiomyomatosis. Chest spontaneous pneumothorax is cost-effective.
2000; 117: 25–30. Am J Respir Crit Care Med 2010; 181: 1376–82.
50 Gao L, Yue MM, Davis J, Hyjek E, Schuger L. In pulmonary 71 Ryu JH, Hartman TE, Torres VE, Decker PA. Frequency of
lymphangioleiomyomatosis expression of progesterone receptor is undiagnosed cystic lung disease in patients with sporadic renal
frequently higher than that of estrogen receptor. Virchows Arch 2014; angiomyolipomas. Chest 2012; 141: 163–68.
464: 495–503. 72 Yeoh ZW, Navaratnam V, Bhatt R, McCafferty I, Hubbard RB,
51 Johnson SR, Tattersfield AE. Decline in lung function in Johnson SR. Natural history of angiomyolipoma in
lymphangioleiomyomatosis: relation to menopause and lymphangioleiomyomatosis: implications for screening and
progesterone treatment. Am J Respir Crit Care Med 1999; surveillance. Orphanet J Rare Dis 2014; 9: 151.
160: 628–33. 73 van Baal JG, Smits NJ, Keeman JN, Lindhout D, Verhoef S.
52 Taveira-DaSilva AM, Johnson SR, Julien-Williams P, Johnson J, The evolution of renal angiomyolipomas in patients with tuberous
Stylianou M, Moss J. Pregnancy in lymphangioleiomyomatosis: sclerosis. J Urol 1994; 152: 35–38.
clinical and lung function outcomes in two national cohorts. Thorax 74 Avila NA, Dwyer AJ, Rabel A, Moss J. Sporadic
2020; 75: 904–07. lymphangioleiomyomatosis and tuberous sclerosis complex with
53 Yano S. Exacerbation of pulmonary lymphangioleiomyomatosis by lymphangioleiomyomatosis: comparison of CT features. Radiology
exogenous oestrogen used for infertility treatment. Thorax 2002; 2007; 242: 277–85.
57: 1085–86. 75 Rakowski SK, Winterkorn EB, Paul E, Steele DJ, Halpern EF,
54 Shen A, Iseman MD, Waldron JA, King TE. Exacerbation of Thiele EA. Renal manifestations of tuberous sclerosis complex:
pulmonary lymphangioleiomyomatosis by exogenous estrogens. incidence, prognosis, and predictive factors. Kidney Int 2006;
Chest 1987; 91: 782–85. 70: 1777–82.
12 www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9
Review
76 Cohen MM, Pollock-BarZiv S, Johnson SR. Emerging clinical 99 Young LR, Vandyke R, Gulleman PM, et al. Serum vascular
picture of lymphangioleiomyomatosis. Thorax 2005; 60: 875–79. endothelial growth factor-D prospectively distinguishes
77 Johnson SR, Tattersfield AE. Clinical experience of lymphangioleiomyomatosis from other diseases. Chest 2010;
lymphangioleiomyomatosis in the UK. Thorax 2000; 55: 1052–57. 138: 674–81.
78 Almoosa KF, Ryu JH, Mendez J, et al. Management of 100 Koba T, Arai T, Kitaichi M, et al. Efficacy and safety of
pneumothorax in lymphangioleiomyomatosis: effects on recurrence transbronchial lung biopsy for the diagnosis of
and lung transplantation complications. Chest 2006; 129: 1274–81. lymphangioleiomyomatosis: a report of 24 consecutive patients.
79 Corrin B, Liebow AA, Friedman PJ. Pulmonary Respirology 2018; 23: 331–38.
lymphangiomyomatosis. A review. Am J Pathol 1975; 79: 348–82. 101 Zhe X, Schuger L. Combined smooth muscle and melanocytic
80 Chu SC, Horiba K, Usuki J, et al. Comprehensive evaluation of differentiation in lymphangioleiomyomatosis. J Histochem Cytochem
35 patients with lymphangioleiomyomatosis. Chest 1999; 2004; 52: 1537–42.
115: 1041–52. 102 Brentani MM, Carvalho CR, Saldiva PH, Pacheco MM, Oshima CT.
81 Avila NA, Dwyer AJ, Murphy-Johnson DV, Brooks P, Moss J. Steroid receptors in pulmonary lymphangiomyomatosis. Chest 1984;
Sonography of lymphangioleiomyoma in 85: 96–99.
lymphangioleiomyomatosis: demonstration of diurnal variation in 103 Matsui K, Takeda K, Yu ZX, et al. Downregulation of estrogen and
lesion size. AJR Am J Roentgenol 2005; 184: 459–64. progesterone receptors in the abnormal smooth muscle cells in
82 Gupta N, Meraj R, Tanase D, et al. Accuracy of chest high-resolution pulmonary lymphangioleiomyomatosis following therapy.
computed tomography in diagnosing diffuse cystic lung diseases. An immunohistochemical study. Am J Respir Crit Care Med 2000;
Eur Respir J 2015; 46: 1196–99. 161: 1002–09.
83 Hayashi T, Kumasaka T, Mitani K, et al. Bronchial involvement in 104 Bonetti F, Pea M, Martignoni G, et al. Clear cell (“sugar”)
advanced stage lymphangioleiomyomatosis: histopathologic and tumor of the lung is a lesion strictly related to angiomyolipoma–
molecular analyses. Hum Pathol 2016; 50: 34–42. the concept of a family of lesions characterized by the presence of
the perivascular epithelioid cells (PEC). Pathology 1994;
84 Walkup LL, Roach DJ, Hall CS, et al. Cyst ventilation
26: 230–36.
heterogeneity and alveolar airspace dilation as early disease
markers in lymphangioleiomyomatosis. Ann Am Thorac Soc 2019; 105 Bonetti F, Chiodera PL, Pea M, et al. Transbronchial biopsy in
16: 1008–16. lymphangiomyomatosis of the lung. HMB45 for diagnosis.
Am J Surg Pathol 1993; 17: 1092–102.
85 Taveira-DaSilva AM, Hedin C, Stylianou MP, et al. Reversible
airflow obstruction, proliferation of abnormal smooth muscle cells, 106 Matsui K, K Riemenschneider W, Hilbert SL, et al. Hyperplasia of
and impairment of gas exchange as predictors of outcome in type II pneumocytes in pulmonary lymphangioleiomyomatosis.
lymphangioleiomyomatosis. Am J Respir Crit Care Med 2001; Arch Pathol Lab Med 2000; 124: 1642–48.
164: 1072–76. 107 Badri KR, Gao L, Hyjek E, et al. Exonic mutations of TSC2/TSC1
86 Kalassian KG, Doyle R, Kao P, Ruoss S, Raffin TA. are common but not seen in all sporadic pulmonary
Lymphangioleiomyomatosis: new insights. lymphangioleiomyomatosis. Am J Respir Crit Care Med 2013;
Am J Respir Crit Care Med 1997; 155: 1183–86. 187: 663–65.
87 Tobino K, Johkoh T, Fujimoto K, et al. Computed tomographic 108 Miller S, Stewart ID, Clements D, Soomro I, Babaei-Jadidi R,
features of lymphangioleiomyomatosis: evaluation in 138 patients. Johnson SR. Evolution of lung pathology in
Eur J Radiol 2015; 84: 534–41. lymphangioleiomyomatosis: associations with disease course and
treatment response. J Pathol Clin Res 2020; 6: 215–26.
88 Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL,
Remy J. Fleischner society: glossary of terms for thoracic imaging. 109 Kumasaka T, Seyama K, Mitani K, et al. Lymphangiogenesis in
Radiology 2008; 246: 697–722. lymphangioleiomyomatosis: its implication in the progression of
lymphangioleiomyomatosis. Am J Surg Pathol 2004; 28: 1007–16.
89 Seaman DM, Meyer CA, Gilman MD, McCormack FX. Diffuse
cystic lung disease at high-resolution CT. AJR Am J Roentgenol 2011; 110 Valencia JC, Pacheco-Rodriguez G, Carmona AK, et al. Tissue-specific
196: 1305–11. renin-angiotensin system in pulmonary lymphangioleiomyomatosis.
Am J Respir Cell Mol Biol 2006; 35: 40–47.
90 Müller NL, Chiles C, Kullnig P. Pulmonary
lymphangiomyomatosis: correlation of CT with radiographic and 111 Inoue Y, King TE Jr, Barker E, Daniloff E, Newman LS. Basic
functional findings. Radiology 1990; 175: 335–39. fibroblast growth factor and its receptors in idiopathic pulmonary
fibrosis and lymphangioleiomyomatosis. Am J Respir Crit Care Med
91 Araki T, Nishino M, Gao W, et al. Pulmonary cysts identified on
2002; 166: 765–73.
chest CT: are they part of aging change or of clinical significance?
Thorax 2015; 70: 1156–62. 112 Dongre A, Clements D, Fisher AJ, Johnson SR. Cathepsin K in
lymphangioleiomyomatosis: LAM cell-fibroblast interactions
92 Northrup H, Krueger DA, Northrup H, et al. Tuberous sclerosis
enhance protease activity by extracellular acidification. Am J Pathol
complex diagnostic criteria update: recommendations of the 2012
2017; 187: 1750–62.
Iinternational Tuberous Sclerosis Complex Consensus conference.
Pediatr Neurol 2013; 49: 243–54. 113 Clements D, Dongre A, Krymskaya VP, Johnson SR. Wild type
mesenchymal cells contribute to the lung pathology of
93 Cudzilo CJ, Szczesniak RD, Brody AS, et al.
lymphangioleiomyomatosis. PLoS One 2015; 10: e0126025.
Lymphangioleiomyomatosis screening in women with tuberous
sclerosis. Chest 2013; 144: 578–85. 114 Young LR, Almoosa KF, Pollock-Barziv S, Coutinho M,
McCormack FX, Sahn SA. Patient perspectives on management of
94 Baldi BG, Pimenta SP, Kawassaki AM, Bernardi FC, Dolhnikoff M,
pneumothorax in lymphangioleiomyomatosis. Chest 2006;
Carvalho CR. Pulmonary arterial involvement leading to alveolar
129: 1267–73.
hemorrhage in lymphangioleiomyomatosis. Clinics (São Paulo)
2011; 66: 1301–03. 115 Gonano C, Pasquier J, Daccord C, et al. Air travel and incidence of
pneumothorax in lymphangioleiomyomatosis. Orphanet J Rare Dis
95 Moua T, Olson EJ, Jean HC, Ryu JH. Resolution of chylous
2018; 13: 222.
pulmonary congestion and respiratory failure in
lymphangioleiomyomatosis with sirolimus therapy. 116 Bissler JJ, Kingswood JC. Optimal treatment of tuberous sclerosis
Am J Respir Crit Care Med 2012; 186: 389–90. complex associated renal angiomyolipomata: a systematic review.
Ther Adv Urol 2016; 8: 279–90.
96 Muir TE, Leslie KO, Popper H, et al. Micronodular pneumocyte
hyperplasia. Am J Surg Pathol 1998; 22: 465–72. 117 Bissler JJ, Kingswood JC, Radzikowska E, et al. Everolimus for
angiomyolipoma associated with tuberous sclerosis complex or
97 Escalon JG, Richards JC, Koelsch T, Downey GP, Lynch DA.
sporadic lymphangioleiomyomatosis (EXIST-2): a multicentre,
Isolated cystic lung disease: an algorithmic approach to
randomised, double-blind, placebo-controlled trial. Lancet 2013;
distinguishing Birt-Hogg-Dubé syndrome,
381: 817–24.
lymphangioleiomyomatosis, and lymphocytic interstitial
pneumonia. AJR Am J Roentgenol 2019; 212: 1–5. 118 Taveira-DaSilva AM, Hathaway O, Stylianou M, Moss J. Changes in
lung function and chylous effusions in patients with
98 Gupta N, Vassallo R, Wikenheiser-Brokamp KA, McCormack FX.
lymphangioleiomyomatosis treated with sirolimus. Ann Intern Med
Diffuse cystic lung disease. Part II. Am J Respir Crit Care Med 2015;
2011; 154: 797–805.
192: 17–29.
www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9 13
Review
119 Ando K, Kurihara M, Kataoka H, et al. Efficacy and safety of 142 Freitas CS, Baldi BG, Araújo MS, Heiden GI, Kairalla RA,
low-dose sirolimus for treatment of lymphangioleiomyomatosis. Carvalho CR. Use of sirolimus in the treatment of
Respir Investig 2013; 51: 175–83. lymphangioleiomyomatosis: favorable responses in patients with
120 Hecimovic A, Jakopovic M, Pavlisa G, et al. Successful treatment of different extrapulmonary manifestations. J Bras Pneumol 2015;
pulmonary and lymphatic manifestations of 41: 275–80.
lymphangioleiomyomatosis with sirolimus. Lymphology 2015; 143 Yoon HY, Hwang JJ, Kim DS, Song JW. Efficacy and safety of
48: 97–102. low-dose sirolimus in lymphangioleiomyomatosis.
121 Kpodonu J, Massad MG, Chaer RA, et al. The US experience with Orphanet J Rare Dis 2018; 13: 204.
lung transplantation for pulmonary lymphangioleiomyomatosis. 144 Johnson J, Johnson SR. Cross-sectional study of reversible airway
J Heart Lung Transplant 2005; 24: 1247–53. obstruction in LAM: better evidence is needed for bronchodilator
122 Boehler A, Speich R, Russi EW, Weder W. Lung transplantation for and inhaled steroid use. Thorax 2019; 74: 999–1002.
lymphangioleiomyomatosis. N Engl J Med 1996; 335: 1275–80. 145 Bendeck MP, Conte M, Zhang M, Nili N, Strauss BH, Farwell SM.
123 Ussavarungsi K, Hu X, Scott JP, et al. Mayo clinic experience of Doxycycline modulates smooth muscle cell growth, migration,
lung transplantation in pulmonary lymphangioleiomyomatosis. and matrix remodeling after arterial injury. Am J Pathol 2002;
Respir Med 2015; 109: 1354–59. 160: 1089–95.
124 Baldi BG, Samano MN, Campos SV, et al. Experience of lung 146 Moses MA, Harper J, Folkman J. Doxycycline treatment for
transplantation in patients with lymphangioleiomyomatosis at a lymphangioleiomyomatosis with urinary monitoring for MMPs.
Brazilian reference centre. Lung 2017; 195: 699–705. N Engl J Med 2006; 354: 2621–22.
125 Ando K, Okada Y, Akiba M, et al. Lung transplantation for 147 Chang WY, Cane JL, Kumaran M, Lewis S, Tattersfield AE,
lymphangioleiomyomatosis in Japan. PLoS One 2016; Johnson SR. A 2-year randomised placebo-controlled trial of
11: e0146749. doxycycline for lymphangioleiomyomatosis. Eur Respir J 2014;
126 Khawar MU, Yazdani D, Zhu Z, Jandarov R, Dilling DF, Gupta N. 43: 1114–23.
Clinical outcomes and survival following lung transplantation in 148 Pimenta SP, Baldi BG, Acencio MM, Kairalla RA, Carvalho CR.
patients with lymphangioleiomyomatosis. J Heart Lung Transplant Doxycycline use in patients with lymphangioleiomyomatosis: safety
2019; 38: 949–55. and efficacy in metalloproteinase blockade. J Bras Pneumol 2011;
127 McCormack FX, Gupta N. Sporadic lymphangioleiomyomatosis: 37: 424–30.
treatment and prognosis. Waltham, MA, USA: UpToDate, 2021. 149 Pimenta SP, Baldi BG, Kairalla RA, Carvalho CR. Doxycycline use
128 Singla A, Gupta N, Apewokin S, McCormack FX. Sirolimus for the in patients with lymphangioleiomyomatosis: biomarkers and
treatment of lymphangioleiomyomatosis. Expert Opin Orphan Drugs pulmonary function response. J Bras Pneumol 2013; 39: 5–15.
2017; 5: 907–21. 150 Baldi BG, Ribeiro Carvalho CR. Doxycycline in
129 Gupta N, Henske EP. Pulmonary manifestations in tuberous lymphangioleiomyomatosis: not all questions are answered.
sclerosis complex. Am J Med Genet C Semin Med Genet 2018; Eur Respir J 2014; 43: 1536–37.
178: 326–37. 151 Clemm C, Jehn U, Wolf-Hornung B, Siemon G, Walter G.
130 Araujo MS, Baldi BG, Freitas CS, et al. Pulmonary rehabilitation in Lymphangiomyomatosis: a report of three cases treated with
lymphangioleiomyomatosis: a controlled clinical trial. Eur Respir J tamoxifen. Klin Wochenschr 1987; 65: 391–93.
2016; 47: 1452–60. 152 Taveira-DaSilva AM, Stylianou MP, Hedin CJ, Hathaway O, Moss J.
131 Urban T, Lazor R, Lacronique J, Murris M, Labrune S, Decline in lung function in patients with
Valeyre D. Pulmonary lymphangioleiomyomatosis. A study of lymphangioleiomyomatosis treated with or without progesterone.
69 patients. Groupe d’Etudes et de Recherche sur les Maladies Chest 2004; 126: 1867–74.
“Orphelines” Pulmonaires (GERM“O”P). Medicine (Baltimore) 153 Ye L, Jin M, Bai C. Clinical analysis of patients with pulmonary
1999; 78: 321–37. lymphangioleiomyomatosis (PLAM) in mainland China. Respir Med
132 Yockey CC, Riepe RE, Ryan K. Pulmonary 2010; 104: 1521–26.
lymphangioleiomyomatosis complicated by pregnancy. Kans Med 154 Harari S, Cassandro R, Chiodini I, Taveira-DaSilva AM, Moss J. Effect
1986; 87: 277–93. of a gonadotrophin-releasing hormone analogue on lung function in
133 Taveira-Dasilva AM, Stylianou MP, Hedin CJ, Hathaway O, Moss J. lymphangioleiomyomatosis. Chest 2008; 133: 448–54.
Bone mineral density in lymphangioleiomyomatosis. 155 Rossi GA, Balbi B, Oddera S, Lantero S, Ravazzoni C. Response to
Am J Respir Crit Care Med 2005; 171: 61–67. treatment with an analog of the luteinizing-hormone-releasing
134 Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to hormone in a patient with pulmonary lymphangioleiomyomatosis.
prevention and treatment of osteoporosis. Osteoporos Int 2014; Am Rev Respir Dis 1991; 143: 174–76.
25: 2359–81. 156 de la Fuente J, Páramo C, Román F, Pérez R, Masa C, de Letona JM.
135 Goldberg HJ, Harari S, Cottin V, et al. Everolimus for the treatment Lymphangioleiomyomatosis: unsuccessful treatment with
of lymphangioleiomyomatosis: a phase II study. Eur Respir J 2015; luteinizing-hormone-releasing hormone analogues. Eur J Med 1993;
46: 783–94. 2: 377–78.
136 Bee J, Fuller S, Miller S, Johnson SR. Lung function response and 157 Banner AS, Carrington CB, Emory WB, et al. Efficacy of
side effects to rapamycin for lymphangioleiomyomatosis: oophorectomy in lymphangioleiomyomatosis and benign
a prospective national cohort study. Thorax 2018; 73: 369–75. metastasizing leiomyoma. N Engl J Med 1981; 305: 204–09.
137 Takada T, Mikami A, Kitamura N, et al. Efficacy and safety of 158 Logan RF, Fawcett IW. Oophorectomy for pulmonary
long-term sirolimus therapy for Asian patients with lymphangioleiomyomatosis: a case report. Br J Dis Chest 1985;
lymphangioleiomyomatosis. Ann Am Thorac Soc 2016; 79: 98–100.
13: 1912–22. 159 Kitzsteiner KA, Mallen RG. Pulmonary lymphangiomyomatosis:
138 Taveira-DaSilva AM, Jones AM, Julien-Williams P, Stylianou M, treatment with castration. Cancer 1980; 46: 2248–49.
Moss J. Long-term effect of sirolimus on serum vascular endothelial 160 Krymskaya VP, Courtwright AM, Fleck V, et al. A phase II clinical
growth factor D levels in patients with lymphangioleiomyomatosis. trial of the safety of simvastatin (SOS) in patients with pulmonary
Chest 2018; 153: 124–32. lymphangioleiomyomatosis and with tuberous sclerosis complex.
139 Yao J, Taveira-DaSilva AM, Jones AM, Julien-Williams P, Respir Med 2020; 163: 105898.
Stylianou M, Moss J. Sustained effects of sirolimus on lung 161 El-Chemaly S, Taveira-Dasilva A, Goldberg HJ, et al. Sirolimus and
function and cystic lung lesions in lymphangioleiomyomatosis. autophagy inhibition in lymphangioleiomyomatosis: results of a
Am J Respir Crit Care Med 2014; 190: 1273–82. phase I clinical trial. Chest 2017; 151: 1302–10.
140 Hu S, Wu X, Xu W, et al. Long-term efficacy and safety of sirolimus 162 El-Chemaly S, Taveira-DaSilva A, Bagwe S, et al. Celecoxib in
therapy in patients with lymphangioleiomyomatosis. lymphangioleiomyomatosis: results of a phase I clinical trial.
Orphanet J Rare Dis 2019; 14: 206. Eur Respir J 2020; 55: 1902370.
141 Zhan Y, Shen L, Xu W, et al. Functional improvements in patients 163 Kurihara M, Mizobuchi T, Kataoka H, et al. A total pleural covering
with lymphangioleiomyomatosis after sirolimus: an observational for lymphangioleiomyomatosis prevents pneumothorax recurrence.
study. Orphanet J Rare Dis 2018; 13: 34. PLoS One 2016; 11: e0163637.
14 www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9
Review
164 Zhou L, Ouyang R, Luo H, et al. Efficacy of sirolimus for the 177 Hayashida M, Yasuo M, Hanaoka M, et al. Reductions in pulmonary
prevention of recurrent pneumothorax in patients with function detected in patients with lymphangioleiomyomatosis:
lymphangioleiomyomatosis: a case series. Orphanet J Rare Dis 2018; An analysis of the Japanese National Research Project on intractable
13: 168. diseases database. Respir Investig 2016; 54: 193–200.
165 Pollock-BarZiv S, Cohen MM, Downey GP, Johnson SR, Sullivan E, 178 Lazor R, Valeyre D, Lacronique J, Wallaert B, Urban T, Cordier JF.
McCormack FX. Air travel in women with Low initial KCO predicts rapid FEV1 decline in pulmonary
lymphangioleiomyomatosis. Thorax 2007; 62: 176–80. lymphangioleiomyomatosis. Respir Med 2004; 98: 536–41.
166 Taveira-DaSilva AM, Burstein D, Hathaway OM, et al. 179 Radzikowska E, Jaguś P, Sobiecka M, et al. Correlation of serum
Pneumothorax after air travel in lymphangioleiomyomatosis, vascular endothelial growth factor-D concentration with clinical
idiopathic pulmonary fibrosis, and sarcoidosis. Chest 2009; presentation and course of lymphangioleiomyomatosis. Respir Med
136: 665–70. 2015; 109: 1469–75.
167 Edvardsen A, Akerø A, Christensen CC, Ryg M, Skjønsberg OH. 180 Hirose M, Matsumuro A, Arai T, et al. Serum vascular endothelial
Air travel and chronic obstructive pulmonary disease: a new growth factor-D as a diagnostic and therapeutic biomarker for
algorithm for pre-flight evaluation. Thorax 2012; 67: 964–69. lymphangioleiomyomatosis. PLoS One 2019; 14: e0212776.
168 Itkin M, McCormack FX. Nonmalignant adult thoracic lymphatic 181 Chang WY, Cane JL, Blakey JD, Kumaran M, Pointon KS,
disorders. Clin Chest Med 2016; 37: 409–20. Johnson SR. Clinical utility of diagnostic guidelines and putative
169 Gupta N, Johnson SR, Moss J, McCormack FX. Reply to biomarkers in lymphangioleiomyomatosis. Respir Res 2012; 13: 34.
Yanagisawa: treatment of pulmonary lymphangioleiomyomatosis 182 Glasgow CG, Avila NA, Lin JP, Stylianou MP, Moss J. Serum
during pregnancy. Am J Respir Crit Care Med 2018; 197: 1507–08. vascular endothelial growth factor-D levels in patients with
170 Faehling M, Frohnmayer S, Leschke M, Trinajstic-Schulz B, lymphangioleiomyomatosis reflect lymphatic involvement. Chest
Weber J, Liewald F. Successful pregnancy complicated by persistent 2009; 135: 1293–300.
pneumothorax in a patient with lymphangioleiomyomatosis (LAM) 183 Oprescu N, McCormack FX, Byrnes S, Kinder BW. Clinical
on sirolimus. Sarcoidosis Vasc Diffuse Lung Dis 2011; 28: 153–55. predictors of mortality and cause of death in
171 Faehling M, Wienhausen-Wilke V, Fallscheer S, lymphangioleiomyomatosis: a population-based registry. Lung 2013;
Trinajstic-Schulz B, Weber J, Leschke M. Long-term stable lung 191: 35–42.
function and second uncomplicated pregnancy on sirolimus in 184 Kitaichi M, Nishimura K, Itoh H, Izumi T. Pulmonary
lymphangioleiomyomatosis (LAM). lymphangioleiomyomatosis: a report of 46 patients including a
Sarcoidosis Vasc Diffuse Lung Dis 2015; 32: 259–64. clinicopathologic study of prognostic factors.
172 Weill D, Benden C, Corris PA, et al. A consensus document for the Am J Respir Crit Care Med 1995; 151: 527–33.
selection of lung transplant candidates: 2014--an update from the 185 Hayashida M, Seyama K, Inoue Y, Fujimoto K, Kubo K.
Pulmonary Transplantation Council of the International Society for The epidemiology of lymphangioleiomyomatosis in Japan:
Heart and Lung Transplantation. J Heart Lung Transplant 2015; a nationwide cross-sectional study of presenting features and
34: 1–15. prognostic factors. Respirology 2007; 12: 523–30.
173 Groetzner J, Kur F, Spelsberg F, et al. Airway anastomosis 186 Matsui K, Beasley MB, Nelson WK, et al. Prognostic significance of
complications in de novo lung transplantation with sirolimus-based pulmonary lymphangioleiomyomatosis histologic score.
immunosuppression. J Heart Lung Transplant 2004; 23: 632–38. Am J Surg Pathol 2001; 25: 479–84.
174 El-Chemaly S, Goldberg HJ, Glanville AR. Should mammalian 187 Di Marco F, Terraneo S, Dias OM, et al. Natural history of incidental
target of rapamycin inhibitors be stopped in women with sporadic and tuberous sclerosis complex associated
lymphangioleiomyomatosis awaiting lung transplantation? lymphangioleiomyomatosis. Respir Med 2020; 168: 105993.
Expert Rev Respir Med 2014; 8: 657–60. 188 Zak S, Mokhallati N, Su W, et al. Lymphangioleiomyomatosis
175 Dilling D, Nair A, Gries C, et al. Use of sirolimus in patients with mortality in patients with tuberous sclerosis complex.
lymphangioleiomyomatosis (LAM) on waiting lists for lung Ann Am Thorac Soc 2019; 16: 509–12.
transplant (LTX). J Heart Lung Transplant 2018; 37: S457.
176 Johnson SR, Whale CI, Hubbard RB, Lewis SA, Tattersfield AE. © 2021 Published by Elsevier Ltd. All rights reserved.
Survival and disease progression in UK patients with
lymphangioleiomyomatosis. Thorax 2004; 59: 800–03.
www.thelancet.com/respiratory Published online August 27, 2021 https://doi.org/10.1016/S2213-2600(21)00228-9 15
You might also like
- Andre Tan's Surgery Notes (Ed 1)Document163 pagesAndre Tan's Surgery Notes (Ed 1)Daniel LimNo ratings yet
- 1-3 Way Bottle System and SuctioningDocument9 pages1-3 Way Bottle System and SuctioningJz Andamun100% (2)
- Pneumothorax, Tension and TraumaticDocument29 pagesPneumothorax, Tension and TraumaticicaNo ratings yet
- ACS/ASE Medical Student Core Curriculum Trauma II: Diagnosis and ManagementDocument35 pagesACS/ASE Medical Student Core Curriculum Trauma II: Diagnosis and ManagementJefriantoNo ratings yet
- Emergency Ultrasound Course-Textbook Update 23 Sept 2008-AdiDocument194 pagesEmergency Ultrasound Course-Textbook Update 23 Sept 2008-AdiHaswady Husaini100% (6)
- Symptoms Differential ChartsDocument52 pagesSymptoms Differential ChartsXiaxin Liu100% (2)
- Tenascin-C Promotes Tumor Cell Migration and Metastasis Through Integrin A9b1-Mediated YAP InhibitionDocument12 pagesTenascin-C Promotes Tumor Cell Migration and Metastasis Through Integrin A9b1-Mediated YAP InhibitionSayda DhaouadiNo ratings yet
- Deros A 2015Document10 pagesDeros A 2015rakaNo ratings yet
- Gerard C Et Al., 2023Document12 pagesGerard C Et Al., 2023rkreid77No ratings yet
- LymphangioleiomyomatosisDocument11 pagesLymphangioleiomyomatosisJimmyNo ratings yet
- Aml NGSDocument13 pagesAml NGSRobie MikhelashviliNo ratings yet
- CSC Colorectal 6Document9 pagesCSC Colorectal 6Diana LaviniaNo ratings yet
- Katabathina Et Al 2021 Testicular Germ Cell Tumors Classification Pathologic Features Imaging Findings and ManagementDocument19 pagesKatabathina Et Al 2021 Testicular Germ Cell Tumors Classification Pathologic Features Imaging Findings and ManagementNicolae ConstantinNo ratings yet
- Tetraspanin 3 Is Required For The Development and Propagation - 2015 - Cell StemDocument14 pagesTetraspanin 3 Is Required For The Development and Propagation - 2015 - Cell StemFrankenstein MelancholyNo ratings yet
- Cellular and Molecular Players in The Tumor Microenvironment of Renal Cell CarcinomaDocument16 pagesCellular and Molecular Players in The Tumor Microenvironment of Renal Cell CarcinomaLuis Javier Vera ZamoraNo ratings yet
- The Potential of Conditionally Replicating AdenovirusDocument1 pageThe Potential of Conditionally Replicating AdenovirusJairo BermúdezNo ratings yet
- Paraneoplastic PCaDocument12 pagesParaneoplastic PCaBrendan DiasNo ratings yet
- Journal Club: Naughty NeutrophilsDocument1 pageJournal Club: Naughty NeutrophilsYanyingLiNo ratings yet
- Leptomeningeal DiseaseDocument17 pagesLeptomeningeal DiseaseForem ZayneNo ratings yet
- Kanker OriDocument17 pagesKanker OriDyah Ayu Septika WijayaNo ratings yet
- Tumores Germinales Del MediastinoDocument7 pagesTumores Germinales Del Mediastinoleonelari102929No ratings yet
- Clinical Practice GuidelinesDocument7 pagesClinical Practice GuidelinesRoppeNo ratings yet
- Liquid Biopsy From Discovery To Clinical ImplementationDocument5 pagesLiquid Biopsy From Discovery To Clinical ImplementationLais BritoNo ratings yet
- Review: Jolanta Malyszko, Petra Tesarova, Giovambattista Capasso, Anna CapassoDocument11 pagesReview: Jolanta Malyszko, Petra Tesarova, Giovambattista Capasso, Anna CapassodickypranataNo ratings yet
- The Role of Automated Cytometry in The New Era of Cancer Immunotherapy (Review)Document7 pagesThe Role of Automated Cytometry in The New Era of Cancer Immunotherapy (Review)Andrea SbranaNo ratings yet
- Extracellular Matrix and Its Therapeutic Potential For Cancer TreatmentDocument24 pagesExtracellular Matrix and Its Therapeutic Potential For Cancer TreatmentANA PAULANo ratings yet
- (2020) Moving From Cancer Burden To Cancer GenomicsDocument8 pages(2020) Moving From Cancer Burden To Cancer GenomicstodosobrecoronavirusNo ratings yet
- Renal and Adrenal Cancer: Clinical Trials, AI, VR and DL in Management and Surgery PlanDocument42 pagesRenal and Adrenal Cancer: Clinical Trials, AI, VR and DL in Management and Surgery PlanProfessor Rakesh Sharma Biochemistry LecturesNo ratings yet
- MTA1 Ekspression in Benign and Malignant Salivary Gland Ijo-28-051Document9 pagesMTA1 Ekspression in Benign and Malignant Salivary Gland Ijo-28-051lukman f0028No ratings yet
- Role of Stat3 in Nasopharyngeal Carcinoma: ReviewDocument5 pagesRole of Stat3 in Nasopharyngeal Carcinoma: Reviewagus karsetiyonoNo ratings yet
- International Myeloma Working Group Updated Criteria For The Diagnosis of Multiple Myeloma LancetOncol-Nov2015Document11 pagesInternational Myeloma Working Group Updated Criteria For The Diagnosis of Multiple Myeloma LancetOncol-Nov2015Andy LNo ratings yet
- Cutaneous MelanomaDocument15 pagesCutaneous MelanomadaltondittzNo ratings yet
- Ijo 35 5 1111 PDFDocument6 pagesIjo 35 5 1111 PDFTibor SzénásiNo ratings yet
- BC Metastasis .FullDocument10 pagesBC Metastasis .FullMAGNo ratings yet
- Radiology 39 3 7Document14 pagesRadiology 39 3 7Tria KurniawatiNo ratings yet
- European Journal of PharmacologyDocument13 pagesEuropean Journal of Pharmacologykamal.nayanNo ratings yet
- Nevus Melanocitico-Nevogenesis y MelanogenesisDocument16 pagesNevus Melanocitico-Nevogenesis y Melanogenesiscarmen lopezNo ratings yet
- Cancer PathologiesDocument5 pagesCancer PathologiesInnocent GeorgeNo ratings yet
- Research Paper Topics On Lung CancerDocument6 pagesResearch Paper Topics On Lung Cancergz8zw71w100% (1)
- ch210005954p PDFDocument5 pagesch210005954p PDFJanNo ratings yet
- Tumor Microenvironment and Immune-Related Therapies of Head and Neck Squamous Cell CarcinomaDocument10 pagesTumor Microenvironment and Immune-Related Therapies of Head and Neck Squamous Cell CarcinomaSpore FluxNo ratings yet
- Bergh 2013Document4 pagesBergh 2013bixagif369No ratings yet
- IUBMB Life - 2020 - Pozzi - Cancer Stem Cell Enrichment Is Associated With Enhancement of Nicotinamide N MethyltransferaseDocument11 pagesIUBMB Life - 2020 - Pozzi - Cancer Stem Cell Enrichment Is Associated With Enhancement of Nicotinamide N MethyltransferasePatricia SolarNo ratings yet
- Tumor Immune Microenvironment Characteristics and Their Prognostic Value in Non-Small-Cell Lung CancerDocument9 pagesTumor Immune Microenvironment Characteristics and Their Prognostic Value in Non-Small-Cell Lung CancerWilliamRayCassidyNo ratings yet
- Ewing 2013Document5 pagesEwing 2013Loc NguyenNo ratings yet
- 2012cancprevres 5 351 4 Metformin Cscs - SemimDocument5 pages2012cancprevres 5 351 4 Metformin Cscs - SemimYolita Satya Gitya UtamiNo ratings yet
- Sjögren's Syndrome: From Pathogenesis To Novel Therapeutic TargetsDocument5 pagesSjögren's Syndrome: From Pathogenesis To Novel Therapeutic TargetsOcha24 TupamahuNo ratings yet
- HLA Genotyping Using Next Generation SequencingDocument7 pagesHLA Genotyping Using Next Generation SequencingNguyen Nguyen ThanhNo ratings yet
- Cam4 9 8333Document12 pagesCam4 9 8333Mithua ghoshNo ratings yet
- Radiographics Esclerosis TuberosaDocument19 pagesRadiographics Esclerosis TuberosaSantiago CeliNo ratings yet
- MMP in MetastasisDocument7 pagesMMP in Metastasistasnishapeer15No ratings yet
- M2 Macrophage-Derived Exosomes Promote Cell Migration and Invasion in Colon CancerDocument13 pagesM2 Macrophage-Derived Exosomes Promote Cell Migration and Invasion in Colon Cancerhup4824No ratings yet
- Tumor Associated Neutrophils. Their Role in Tumorigenesis, Metastasis, Prognosis and TherapyDocument16 pagesTumor Associated Neutrophils. Their Role in Tumorigenesis, Metastasis, Prognosis and TherapyPraveenNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Patogenesis Del MelanomaDocument10 pagesPatogenesis Del Melanomajenith andradeNo ratings yet
- Science - Aaa4971 2Document7 pagesScience - Aaa4971 2Alejandro Zuñiga NaterasNo ratings yet
- Management of Acute LeukemiaDocument11 pagesManagement of Acute LeukemiaNicoletta ColomboNo ratings yet
- Modpathol 201783Document14 pagesModpathol 201783Tian Nopita SariNo ratings yet
- Article 5 POCDocument16 pagesArticle 5 POCmariimaria670No ratings yet
- The Molecular Biology of Cancer: A Bridge from Bench to BedsideFrom EverandThe Molecular Biology of Cancer: A Bridge from Bench to BedsideStella PelengarisNo ratings yet
- s41598 018 35903 5Document9 pagess41598 018 35903 5leartaNo ratings yet
- GMN MembranosaDocument23 pagesGMN MembranosaGabriela VaraNo ratings yet
- Extracellular Nucleotides As Novel, Underappreciated Pro-Metastatic Factors That Stimulate Purinerhuman LuDocument15 pagesExtracellular Nucleotides As Novel, Underappreciated Pro-Metastatic Factors That Stimulate Purinerhuman LuLeonel LedezmaNo ratings yet
- Loss of Mir-223 and JNK Signaling Contribute To Elevated Stathmin in Malignant Pleural MesotheliomaDocument14 pagesLoss of Mir-223 and JNK Signaling Contribute To Elevated Stathmin in Malignant Pleural MesotheliomaDario AnobileNo ratings yet
- Breast Tumor Microenvironment: Proteomics Highlights The Treatments Targeting SecretomeDocument9 pagesBreast Tumor Microenvironment: Proteomics Highlights The Treatments Targeting SecretomeestifanosNo ratings yet
- Leukocyte ComplexityDocument15 pagesLeukocyte ComplexityMelinda Rohmatika Arum DhatiNo ratings yet
- Thoracic Ultrasonography: Clinical Uses and ApplicationsDocument54 pagesThoracic Ultrasonography: Clinical Uses and ApplicationsMesay AssefaNo ratings yet
- Care of Patient On I C DDocument15 pagesCare of Patient On I C DGeorge John Jeelu SusanNo ratings yet
- Christopher Jefford CVDocument3 pagesChristopher Jefford CVapi-638165457No ratings yet
- Caring For The Patient On A VentilatorDocument10 pagesCaring For The Patient On A Ventilatorekrams100% (1)
- Tactical Combat Casualty CareDocument88 pagesTactical Combat Casualty CareFirefighther Ayala100% (4)
- Procedures ThoracentesisDocument4 pagesProcedures ThoracentesisPatty MArivel ReinosoNo ratings yet
- PJ Medical HandbookDocument210 pagesPJ Medical HandbookJared A. Lang100% (3)
- Bronchi 0Document52 pagesBronchi 0Jennifer DixonNo ratings yet
- Full Chapter Self Assessment in Respiratory Medicine 3Rd Edition Konrad E Bloch PDFDocument63 pagesFull Chapter Self Assessment in Respiratory Medicine 3Rd Edition Konrad E Bloch PDFgail.wright277100% (2)
- AtlsDocument2 pagesAtlsAlexandros Megas100% (2)
- Unusual Presentations of Child Abuse, A Report of Two Cases and The Role of ImagingDocument5 pagesUnusual Presentations of Child Abuse, A Report of Two Cases and The Role of ImaginggeaninalexaNo ratings yet
- Candid PTXDocument10 pagesCandid PTXSamruddhi ShastriNo ratings yet
- Medicine OSCE LatestDocument231 pagesMedicine OSCE LatestPrasad HewawasamNo ratings yet
- Expert DDX ChestDocument1,053 pagesExpert DDX ChestClaudio Rodriguez100% (1)
- SaveBooklet BookletDocument120 pagesSaveBooklet BookletRoscelie KhoNo ratings yet
- Pulmonary Emergencies 2016 PDFDocument252 pagesPulmonary Emergencies 2016 PDFBea Sph100% (2)
- Chest Tube: Dr. Feizal FaturahmanDocument21 pagesChest Tube: Dr. Feizal FaturahmanfaturNo ratings yet
- A Nurse Is Preparing To Obtain A Sputum Specimen From A Male ClientDocument32 pagesA Nurse Is Preparing To Obtain A Sputum Specimen From A Male ClientSophia Veron50% (2)
- The Radiology Assistant - Basic InterpretationDocument67 pagesThe Radiology Assistant - Basic InterpretationMaria LimaNo ratings yet
- HematotoraksDocument15 pagesHematotorakssafanj12No ratings yet
- Case Study TemplateDocument5 pagesCase Study TemplateDinarkram Rabreca EculNo ratings yet
- SPTatls2 9thDocument4 pagesSPTatls2 9thdevi ipul100% (6)
- Respirator Medical Evaluation Questionnaire: To Be Filled Out by The EmployeeDocument5 pagesRespirator Medical Evaluation Questionnaire: To Be Filled Out by The Employeerustynail35209No ratings yet
- Use of WhatsApp For Sharing Preanesthesia Evaluation FormDocument2 pagesUse of WhatsApp For Sharing Preanesthesia Evaluation FormaksinuNo ratings yet