Download as pdf or txt
You might also like
- Case Report ScoliosisDocument67 pagesCase Report ScoliosisNurul Husna RashidNo ratings yet
- Amado Carrillo Fuentes - The Killer Across The River by Charles BowdenDocument16 pagesAmado Carrillo Fuentes - The Killer Across The River by Charles BowdenChad B Harper100% (1)
- Ic 01 Last Day Test 3Document30 pagesIc 01 Last Day Test 3Sohini0% (1)
- Ufc 1 200 01 PDFDocument28 pagesUfc 1 200 01 PDFadangkoswaraNo ratings yet
- SPLK-1001: Number: SPLK-1001 Passing Score: 800 Time Limit: 120 Min File Version: 1Document36 pagesSPLK-1001: Number: SPLK-1001 Passing Score: 800 Time Limit: 120 Min File Version: 1abhishek_singh10272No ratings yet
- Shoulder Dislocation: Orthopedics Department DR Kilian K.KDocument32 pagesShoulder Dislocation: Orthopedics Department DR Kilian K.KInnocentNo ratings yet
- Ortho Review 1Document67 pagesOrtho Review 1mark tNo ratings yet
- Lapsus Ortho Word - Id.enDocument17 pagesLapsus Ortho Word - Id.eninhaNo ratings yet
- Ortho - Surgery PDFDocument15 pagesOrtho - Surgery PDFIC BNo ratings yet
- CaseDocument31 pagesCaseNovitasariyantiNo ratings yet
- Rekapan Kuis CPPDS Orthopedi Periode Januari 2023Document82 pagesRekapan Kuis CPPDS Orthopedi Periode Januari 2023Indra Anwari RukmanNo ratings yet
- Compilation Spinal SsmsDocument35 pagesCompilation Spinal SsmsPiaRomildaTagaoCayetano100% (1)
- Dislocations (PDFDrive)Document111 pagesDislocations (PDFDrive)hemasary15No ratings yet
- Chapter 24Document26 pagesChapter 24Dr Uvarani Sp Care Rawang TinNo ratings yet
- Halaman PengesahanDocument16 pagesHalaman PengesahanEga NoristaNo ratings yet
- Case ReportDocument29 pagesCase ReportMagnusNo ratings yet
- Trauma Musculoskeletal - Spine FKK UMJ1Document92 pagesTrauma Musculoskeletal - Spine FKK UMJ1Hendra Hash AwoNo ratings yet
- Fractures of The Elbow Joint 2Document41 pagesFractures of The Elbow Joint 2Noor Al Zahraa AliNo ratings yet
- S.S. Medical College Rewa & Associated G.M.H & SGM Hospital, Rewa (M.P.)Document47 pagesS.S. Medical College Rewa & Associated G.M.H & SGM Hospital, Rewa (M.P.)Chrysi TsiouriNo ratings yet
- Surgery - OSPE - Dr. - Talat - With - Bookmarks - PDF Filename - UTF-8''Surgery OSPE (Dr. Talat) - With Bookmarks-1 PDFDocument92 pagesSurgery - OSPE - Dr. - Talat - With - Bookmarks - PDF Filename - UTF-8''Surgery OSPE (Dr. Talat) - With Bookmarks-1 PDFM NMNo ratings yet
- Cervical Spine DisorderDocument9 pagesCervical Spine DisorderANDRE MANo ratings yet
- Case ReportDocument19 pagesCase Reportrizaldy syahNo ratings yet
- Neuro Year 3 MedEd Rehaan Khokar 2Document91 pagesNeuro Year 3 MedEd Rehaan Khokar 2Sugoi SagaNo ratings yet
- Adhesive CapsulitisDocument7 pagesAdhesive CapsulitisMariane GumbanNo ratings yet
- TrunkDocument86 pagesTrunkdr_asalehNo ratings yet
- Self-Directed LearningDocument3 pagesSelf-Directed Learningapi-479849199No ratings yet
- Orthopaedic!Document15 pagesOrthopaedic!bowelprepcolonNo ratings yet
- Orthopedic: OrthopaedicsDocument11 pagesOrthopedic: OrthopaedicsDrAyyoub AbboodNo ratings yet
- Evaluation of Lumbar Spine MRIDocument20 pagesEvaluation of Lumbar Spine MRIDharam Pandey100% (2)
- ContractureDocument45 pagesContracturePramitha Yustia100% (1)
- 1 - Introduction To The Orthopedics (Updated)Document11 pages1 - Introduction To The Orthopedics (Updated)Dahir Sani YaAmeerNo ratings yet
- 0 Yazan Mini-OSCE Others and ToolsDocument68 pages0 Yazan Mini-OSCE Others and Toolsmoyasserayoub78No ratings yet
- 14 - Bone Tumors (Ubdated)Document23 pages14 - Bone Tumors (Ubdated)khalifasweadNo ratings yet
- Lapsus Fraktur VickDocument32 pagesLapsus Fraktur VickBhethari Ayu KusumaNo ratings yet
- Kamars RadiologyDocument135 pagesKamars RadiologyNayantara Nair100% (1)
- Review - SurgeryDocument40 pagesReview - SurgerymedstudNo ratings yet
- Thoracal Fracture of The SpineDocument32 pagesThoracal Fracture of The Spinefaranur sabudinNo ratings yet
- DR - Rieva Kuliah 7 November - 2018Document38 pagesDR - Rieva Kuliah 7 November - 2018Nisrina100% (1)
- Shoulder HX and Ex.-1Document61 pagesShoulder HX and Ex.-1Saleem BahranNo ratings yet
- Spinal Cord Injury: Philippine Orthopedic Center Group1 Section B "Reydi Badi"Document11 pagesSpinal Cord Injury: Philippine Orthopedic Center Group1 Section B "Reydi Badi"Sugar Capule - ManuelNo ratings yet
- Closed Fracture of Left Femoral Neck: Case ReportDocument31 pagesClosed Fracture of Left Femoral Neck: Case Reporttari nurulNo ratings yet
- Medi 95 E2797Document3 pagesMedi 95 E2797Rui Pedro PereiraNo ratings yet
- TB SpineDocument18 pagesTB SpineUsaid SulaimanNo ratings yet
- SLAP Lesions of The ShoulderDocument6 pagesSLAP Lesions of The ShoulderPaula Valeria González MarchantNo ratings yet
- You Answered Subacute Degeneration of The CordDocument80 pagesYou Answered Subacute Degeneration of The Cord5alifa55No ratings yet
- 15 - Common Shoulder DisordersDocument70 pages15 - Common Shoulder DisordersSyafaringga Dian oscarNo ratings yet
- Bone CongenitalDocument33 pagesBone CongenitalRadio ResidentNo ratings yet
- Closed Comminutive Fracture Middle Left Clavicle Allman Classification Group IDocument32 pagesClosed Comminutive Fracture Middle Left Clavicle Allman Classification Group IWilliamtatokieesz Tembokrumahampebenjol-benjolNo ratings yet
- Cedera Saraf Spinal Cervical DR FAZDocument52 pagesCedera Saraf Spinal Cervical DR FAZditya_madridistasNo ratings yet
- Paediatric OrthopaedicDocument77 pagesPaediatric Orthopaedicdr_asalehNo ratings yet
- Random Axial (Free / Pedicle)Document10 pagesRandom Axial (Free / Pedicle)Sara Abdul RahmanNo ratings yet
- Rotator Cuff Lesions: A Case ReportDocument8 pagesRotator Cuff Lesions: A Case ReportUbaidillah Romadlon AlfairuziNo ratings yet
- Shoulder Injuries and SportDocument12 pagesShoulder Injuries and SportSurgicalgownNo ratings yet
- All Previous Essay SurgeryDocument170 pagesAll Previous Essay Surgeryalsfyabdullah2021No ratings yet
- Fractures and Dislocation: ArnadiDocument30 pagesFractures and Dislocation: ArnadiNizai Rama DeswiraNo ratings yet
- Shoulder Arthroplasty: Types - Indication - RehabilitationDocument35 pagesShoulder Arthroplasty: Types - Indication - RehabilitationPerjalanan SukarNo ratings yet
- DD Case Report Elbow DislocationDocument33 pagesDD Case Report Elbow DislocationKurniawan Nur IhsanNo ratings yet
- S - Fractures of The Scapula - RIDocument42 pagesS - Fractures of The Scapula - RIdokter ilhamNo ratings yet
- Proteus SyndromeDocument6 pagesProteus SyndromeAnshul JainNo ratings yet
- Musculoskeletal Cases For Finals: DR Alastair Brown ST1 Neurosurgery CXHDocument38 pagesMusculoskeletal Cases For Finals: DR Alastair Brown ST1 Neurosurgery CXHAravind RaviNo ratings yet
- M208 MSK+CNS Summative (12 Nov 2010)Document11 pagesM208 MSK+CNS Summative (12 Nov 2010)Thulasi tootsieNo ratings yet
- All Previous Essay Surgery 2Document162 pagesAll Previous Essay Surgery 2DR/ AL-saifiNo ratings yet
- Medad Note of Orthopedics SpecialityDocument34 pagesMedad Note of Orthopedics SpecialityAtef FahmyNo ratings yet
- 13L00501A - 7P-A: General NotesDocument7 pages13L00501A - 7P-A: General NotesCLS AKNo ratings yet
- Ebiz Steps PDFDocument59 pagesEbiz Steps PDFBathina Srinivasa RaoNo ratings yet
- Dvp-Es2 Ss2 Sa2 Sx2-Program o en 20110302Document609 pagesDvp-Es2 Ss2 Sa2 Sx2-Program o en 20110302puskyboyNo ratings yet
- Characteristics Finite Element Methods in Computational Fluid Dynamics - J. Iannelli (Springer, 2006) WW PDFDocument744 pagesCharacteristics Finite Element Methods in Computational Fluid Dynamics - J. Iannelli (Springer, 2006) WW PDFsanaNo ratings yet
- Mccsemi: 1N746 A Thru 1N759 ADocument3 pagesMccsemi: 1N746 A Thru 1N759 AЕвгений ИвановNo ratings yet
- HP Catalogue-NewDocument5 pagesHP Catalogue-NewNasree NiswongNo ratings yet
- Chapter Outline For FTSDocument1 pageChapter Outline For FTSBalvinder SinghNo ratings yet
- PoonamDocument54 pagesPoonamCH Rajan GujjarNo ratings yet
- Lean Six Sigma Black Belt - BrochureDocument3 pagesLean Six Sigma Black Belt - BrochureDevraj NagarajraoNo ratings yet
- Case Study Emirates AirlinesDocument4 pagesCase Study Emirates Airlinesuzzmapk33% (9)
- Bahasa Inggris Lawang SewuDocument12 pagesBahasa Inggris Lawang Sewuaisyah100% (1)
- Fructin PDFDocument1 pageFructin PDFSaifur Rahman SuzonNo ratings yet
- Nasa Design On Jet PumpsDocument44 pagesNasa Design On Jet PumpsJason BakerNo ratings yet
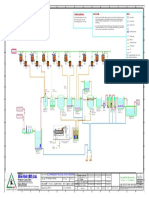
- Alim Knit (BD) LTD.: Recommended Process Flow DiagramDocument1 pageAlim Knit (BD) LTD.: Recommended Process Flow DiagramKamrul HasanNo ratings yet
- Score:: 1 Out of 1.00 PointDocument12 pagesScore:: 1 Out of 1.00 PointDiscord YtNo ratings yet
- PMP Exam EVOVLE Free SampleDocument47 pagesPMP Exam EVOVLE Free SampleEvolve trainingmaterialsNo ratings yet
- Comparing Low RPM Juicers by John KohlerDocument12 pagesComparing Low RPM Juicers by John Kohlerandra_panaitNo ratings yet
- The Filipino EmpanadaDocument2 pagesThe Filipino EmpanadaMaria Lourdez Bayan100% (3)
- Vietnam Reward Trends 2015-2016.mercer - TalentnetDocument50 pagesVietnam Reward Trends 2015-2016.mercer - TalentnetTran TamNo ratings yet
- Nokia: Management of SmesDocument32 pagesNokia: Management of SmesSimone SantosNo ratings yet
- ASR 2020 J2Prelim H2Chem P4 QP PDFDocument20 pagesASR 2020 J2Prelim H2Chem P4 QP PDFchuasioklengNo ratings yet
- Heat, Temperature, and Heat Transfer: Cornell Doodle Notes FREE SAMPLERDocument13 pagesHeat, Temperature, and Heat Transfer: Cornell Doodle Notes FREE SAMPLERShraddha PatelNo ratings yet
- Discussion Questions Activity NoDocument2 pagesDiscussion Questions Activity NoAngilene Lacson CabinianNo ratings yet
- Sist TS Cen TS 17091 2018Document11 pagesSist TS Cen TS 17091 2018سعد خضر الياسNo ratings yet
- From Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityDocument14 pagesFrom Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityLing LIUNo ratings yet
- 1097-1136 Metallogenic Provinces in An Evolving Geodynamic FrameworkDocument40 pages1097-1136 Metallogenic Provinces in An Evolving Geodynamic FrameworkLYNAMARICELA83No ratings yet