
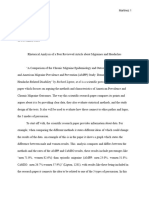
Psychometric Properties of The MMPI-3 in A Sample of Black and White American Undergraduate Students Examining Group Differences and Convergent Discr
Psychometric Properties of The MMPI-3 in A Sample of Black and White American Undergraduate Students Examining Group Differences and Convergent Discr
You might also like
- LO4: Testing: Unit 18-Computer Systems HardwareDocument8 pagesLO4: Testing: Unit 18-Computer Systems Hardware20holmesloNo ratings yet
- Data Migration Projects TDDDocument30 pagesData Migration Projects TDDMadhuNo ratings yet
- F 584 C 6481 FDBDocument157 pagesF 584 C 6481 FDBgayathriNo ratings yet
- Cross-Cultural Reliability andDocument26 pagesCross-Cultural Reliability anderazermanuelNo ratings yet
- Chapter 3Document4 pagesChapter 3Dariann Jane HipolitoNo ratings yet
- 2022 Article 9908Document14 pages2022 Article 9908Harshita SinghNo ratings yet
- Development and Initial Validation of Personality Disorder Syndrome Scales For The MMPI-3Document16 pagesDevelopment and Initial Validation of Personality Disorder Syndrome Scales For The MMPI-3rushnaNo ratings yet
- WhitmanHolmesetal.2023MMPI 3NEOPI RincrementalvalidityDocument23 pagesWhitmanHolmesetal.2023MMPI 3NEOPI RincrementalvalidityrushnaNo ratings yet
- Comparison of Three Multigroup Ethnic Identity Measure Models: A Confirmatory Analysis With Female PopulationDocument10 pagesComparison of Three Multigroup Ethnic Identity Measure Models: A Confirmatory Analysis With Female PopulationAJHSSR JournalNo ratings yet
- Final Draft Essay 3Document5 pagesFinal Draft Essay 3api-709105209No ratings yet
- Running Head: Evaluating Significance of Findings 1Document4 pagesRunning Head: Evaluating Significance of Findings 1Juliet vutemeNo ratings yet
- The Sexist in You: Relationship of Entitlement To Ambivalent SexismDocument17 pagesThe Sexist in You: Relationship of Entitlement To Ambivalent SexismJ. ClimacoNo ratings yet
- Comparing The Validity of MMPI-3 Scores in Prehire Psychological Screenings of Male and Female Police Officer CandidatesDocument11 pagesComparing The Validity of MMPI-3 Scores in Prehire Psychological Screenings of Male and Female Police Officer CandidatesrushnaNo ratings yet
- 1Document5 pages1Mdeme CleptoNo ratings yet
- Gender Body Size and Social Relations in American High Schools - 50Document29 pagesGender Body Size and Social Relations in American High Schools - 50AgungNo ratings yet
- Catania 2015Document17 pagesCatania 2015Max SarmentoNo ratings yet
- Spss Data Assignment FinalDocument8 pagesSpss Data Assignment Finalapi-282530805No ratings yet
- Jackson Et Al. 2009. Reporting Practices in Confirmatory Factor Analysis An Overview and Some RecommendationsDocument18 pagesJackson Et Al. 2009. Reporting Practices in Confirmatory Factor Analysis An Overview and Some RecommendationslengocthangNo ratings yet
- Criminal PersonalityDocument17 pagesCriminal PersonalityLori JeffriesNo ratings yet
- 2020 Article 323Document13 pages2020 Article 323Sarra TekayaNo ratings yet
- Background and PurposeDocument6 pagesBackground and Purposerupa4No ratings yet
- Mata 2021Document11 pagesMata 2021Archondakis StavrosNo ratings yet
- Allen and Tussey, 2012Document15 pagesAllen and Tussey, 2012Ellis FreedmanNo ratings yet
- CTQDocument15 pagesCTQElliott FisherNo ratings yet
- Mortier 2018Document12 pagesMortier 2018PiramaxNo ratings yet
- A Meta-Analytic Review of Racial Discrimination Relationships To Health and CultureDocument18 pagesA Meta-Analytic Review of Racial Discrimination Relationships To Health and Cultureflavio rodasNo ratings yet
- Personality and Individual Differences: Graeme GallowayDocument5 pagesPersonality and Individual Differences: Graeme GallowayAndreea PîntiaNo ratings yet
- BirkmanvsbmtiDocument20 pagesBirkmanvsbmtiDavid BergeNo ratings yet
- Clinical Social Work Scope ofDocument12 pagesClinical Social Work Scope ofblackrandioresNo ratings yet
- Mcmi Sexual OfendersDocument17 pagesMcmi Sexual OfendersllamavioletNo ratings yet
- The Prevalence of Posttraumatic Stress Disorder and Its Severity Among Sexual and Gender Minority Individuals From Selected Support Groups in KenyaDocument9 pagesThe Prevalence of Posttraumatic Stress Disorder and Its Severity Among Sexual and Gender Minority Individuals From Selected Support Groups in KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter ThreeDocument3 pagesChapter Threeariwodola daramolaNo ratings yet
- A Critical Review of Objective Personality Inventories With Sex OffendersDocument28 pagesA Critical Review of Objective Personality Inventories With Sex Offenderstim radellNo ratings yet
- Research Critique PaperDocument6 pagesResearch Critique PaperJeremy RichuNo ratings yet
- Homicide Studies 2011 Nivette 103 31Document30 pagesHomicide Studies 2011 Nivette 103 31Corina IcaNo ratings yet
- Racial Ethnic Reporting Differences in Cancer Literature Regarding Machine Learning Vs A Radiologist - A Systematic Review and Meta-AnalysisDocument11 pagesRacial Ethnic Reporting Differences in Cancer Literature Regarding Machine Learning Vs A Radiologist - A Systematic Review and Meta-Analysiscerberus thanatosNo ratings yet
- American Association For Public Opinion Research, Oxford University Press The Public Opinion QuarterlyDocument31 pagesAmerican Association For Public Opinion Research, Oxford University Press The Public Opinion QuarterlyVLad2385No ratings yet
- University Students Perceptions and Attitudes Towards Sexual OffendersDocument16 pagesUniversity Students Perceptions and Attitudes Towards Sexual Offendersapi-607589196No ratings yet
- KeithkatDocument16 pagesKeithkatEunice Ann TiquiaNo ratings yet
- Meera Khemani 2039237 - Cia2 - br2Document3 pagesMeera Khemani 2039237 - Cia2 - br2Meera KhemaniNo ratings yet
- Personality Outcomes Across Samples Final MSDocument22 pagesPersonality Outcomes Across Samples Final MSpsleonardolagosNo ratings yet
- 2-S2.0-S0027968418301640-Am Imp PUMEDDocument14 pages2-S2.0-S0027968418301640-Am Imp PUMEDFabiana H. ShimabukuroNo ratings yet
- A Systematic Review of Empirical Research On Self-Reported Racism and HealthDocument14 pagesA Systematic Review of Empirical Research On Self-Reported Racism and Healthbob antonioNo ratings yet
- Personality Assessment in A Diverse Urban Sample: Brief ReportDocument6 pagesPersonality Assessment in A Diverse Urban Sample: Brief ReportNaga Sayana Srinivas KoneruNo ratings yet
- Kuhns WebDocument14 pagesKuhns WebRafael HenriqueNo ratings yet
- The Structure of The Statistics Anxiety Rating Scale: A Confirmatory Factor Analysis Using UK Psychology StudentsDocument24 pagesThe Structure of The Statistics Anxiety Rating Scale: A Confirmatory Factor Analysis Using UK Psychology StudentsTroy CabrillasNo ratings yet
- Chapter 3 Research MethodologyDocument8 pagesChapter 3 Research MethodologyMr PlagiarismNo ratings yet
- Using Latent Class Analysis To Model Prescription Medications in The Measurement of Falling Among A Community Elderly PopulationDocument7 pagesUsing Latent Class Analysis To Model Prescription Medications in The Measurement of Falling Among A Community Elderly PopulationIcaroNo ratings yet
- Epm318769 0 PDFDocument17 pagesEpm318769 0 PDFDristorXelaNo ratings yet
- Sampling TechniquesDocument23 pagesSampling TechniquesanilNo ratings yet
- How Prevalent Are Potentially Illegal Questions During Residency Interviews - A Follow-Up Study of Applicants To All Specialties in The National Resident Matching ProgramDocument8 pagesHow Prevalent Are Potentially Illegal Questions During Residency Interviews - A Follow-Up Study of Applicants To All Specialties in The National Resident Matching ProgramMohammad ZaherNo ratings yet
- Chapter 3 - SampleDocument5 pagesChapter 3 - SampleJe CoNo ratings yet
- Incidence of Anorexia Nervosa in Women: A Systematic Review and Meta-AnalysisDocument15 pagesIncidence of Anorexia Nervosa in Women: A Systematic Review and Meta-AnalysisandreaNo ratings yet
- Semenza-Et-Al-2022-Mental-Illness-And-Racial-Disparities-In-Correctional-Staff-Involved-Violence-An-Analysis-Of-Jails Mental 1 YesDocument28 pagesSemenza-Et-Al-2022-Mental-Illness-And-Racial-Disparities-In-Correctional-Staff-Involved-Violence-An-Analysis-Of-Jails Mental 1 YessilviaNo ratings yet
- FoMO341 354Document15 pagesFoMO341 354Phan Thanh ĐạtNo ratings yet
- Population Pharmacokinetics: Theory Practice: RecentlyDocument2 pagesPopulation Pharmacokinetics: Theory Practice: RecentlyabinchandrakumarNo ratings yet
- Audit DiscriminationDocument30 pagesAudit DiscriminationnachersNo ratings yet
- PsNP07-08.04 Blazevska - Stoilkovska, B., Naumova, KDocument15 pagesPsNP07-08.04 Blazevska - Stoilkovska, B., Naumova, KBorjan AdziskiNo ratings yet
- Jurnal Psikologi KlinisDocument6 pagesJurnal Psikologi KlinisRosaDeviNo ratings yet
- The Childhood Trauma Questionnaire in ADocument15 pagesThe Childhood Trauma Questionnaire in ATuấn KhangNo ratings yet
- Maureen Order 559755.86 Data Collection, Evaluating, Summarizing and Analysis Strategies 2pg FDocument4 pagesMaureen Order 559755.86 Data Collection, Evaluating, Summarizing and Analysis Strategies 2pg Fwriter lonicNo ratings yet
- Qualitative Research:: Intelligence for College StudentsFrom EverandQualitative Research:: Intelligence for College StudentsRating: 4 out of 5 stars4/5 (1)
- Psychiatric Disorders in Term-Born Children With Marginally Low Birth Weight: A Population-Based StudyDocument11 pagesPsychiatric Disorders in Term-Born Children With Marginally Low Birth Weight: A Population-Based StudyrushnaNo ratings yet
- Short Term Neonatal and Long Term Neurodevelopmental Outcome of Children Born Term Low Birth WeightDocument8 pagesShort Term Neonatal and Long Term Neurodevelopmental Outcome of Children Born Term Low Birth WeightrushnaNo ratings yet
- Machine Learning Applied To Student Attentiveness Detection: Using Emotional and Non Emotional MeasuresDocument21 pagesMachine Learning Applied To Student Attentiveness Detection: Using Emotional and Non Emotional MeasuresrushnaNo ratings yet
- Systematic Literature Review and Bibliometric Analysis On Virtual Reality and EducationDocument38 pagesSystematic Literature Review and Bibliometric Analysis On Virtual Reality and EducationrushnaNo ratings yet
- Autism in Lebanon Looking Back To Inform The FutureDocument10 pagesAutism in Lebanon Looking Back To Inform The FuturerushnaNo ratings yet
- Hosozawa 2024 Oi 231548 1705094509.26292Document12 pagesHosozawa 2024 Oi 231548 1705094509.26292rushnaNo ratings yet
- WhitmanHolmesetal.2023MMPI 3NEOPI RincrementalvalidityDocument23 pagesWhitmanHolmesetal.2023MMPI 3NEOPI RincrementalvalidityrushnaNo ratings yet
- SSRN Id3799204Document20 pagesSSRN Id3799204rushnaNo ratings yet
- Neuropsychological AssessmentsDocument48 pagesNeuropsychological AssessmentsrushnaNo ratings yet
- The Role of Spatial Ability in Mixed Reality Learning With The HololensDocument12 pagesThe Role of Spatial Ability in Mixed Reality Learning With The HololensrushnaNo ratings yet
- Ucar Icatces ProceedingDocument15 pagesUcar Icatces ProceedingrushnaNo ratings yet
- Research Methods Tools and TechniquesDocument84 pagesResearch Methods Tools and TechniquesrushnaNo ratings yet
- Comment: Materials and Devices For Immersive Virtual RealityDocument3 pagesComment: Materials and Devices For Immersive Virtual RealityrushnaNo ratings yet
- Psychopathology of adults-CODocument17 pagesPsychopathology of adults-COrushnaNo ratings yet
- VR4Health: Personalized Teaching and Learning Anatomy Using VRDocument11 pagesVR4Health: Personalized Teaching and Learning Anatomy Using VRrushnaNo ratings yet
- What Are Research Objectives and How To Write ThemDocument9 pagesWhat Are Research Objectives and How To Write ThemrushnaNo ratings yet
- Disruptive DisorderDocument24 pagesDisruptive DisorderrushnaNo ratings yet
- BGT 2Document29 pagesBGT 2rushnaNo ratings yet
- Psychodiagnostic Assessment of ChildrenDocument26 pagesPsychodiagnostic Assessment of ChildrenrushnaNo ratings yet
- Research Methodology-CODocument5 pagesResearch Methodology-COrushnaNo ratings yet
- Neuropsychological AssessmentDocument35 pagesNeuropsychological AssessmentrushnaNo ratings yet
- Neuropsychological AssessmentDocument27 pagesNeuropsychological AssessmentrushnaNo ratings yet
- Psychosocial AssesmentDocument37 pagesPsychosocial AssesmentrushnaNo ratings yet
- Course Outline On Psychodiagnostic Assessment of ChildrenDocument5 pagesCourse Outline On Psychodiagnostic Assessment of ChildrenrushnaNo ratings yet
- Endocrinology LectureDocument40 pagesEndocrinology LecturerushnaNo ratings yet
- PsychopharmacologyDocument59 pagesPsychopharmacologyrushnaNo ratings yet
- NeurotransmittersDocument29 pagesNeurotransmittersrushnaNo ratings yet
- Antipsychotics PsychopharmacologyDocument15 pagesAntipsychotics PsychopharmacologyrushnaNo ratings yet
- ADHDDocument29 pagesADHDrushnaNo ratings yet
- Psychopathology-Multicultral UnderstandingDocument21 pagesPsychopathology-Multicultral UnderstandingrushnaNo ratings yet
- Pipe Bend RadiusDocument8 pagesPipe Bend RadiusAdagharaNo ratings yet
- Configurar Session-Ttl en FortigateDocument2 pagesConfigurar Session-Ttl en FortigatemasmisemNo ratings yet
- PC 2201Document12 pagesPC 2201Irwan SamtaniNo ratings yet
- SSC CGL 2 Dec 2022 Shift 3 Question PaperDocument27 pagesSSC CGL 2 Dec 2022 Shift 3 Question Papernakul yadavNo ratings yet
- Home Work Assignment - 1Document4 pagesHome Work Assignment - 1Agnivesh SharmaNo ratings yet
- Python Modules: What Is A Module?Document9 pagesPython Modules: What Is A Module?Krishnaprasad kNo ratings yet
- Oscillatory Motion: Multiple ChoiceDocument14 pagesOscillatory Motion: Multiple ChoiceCamilo ValenciaNo ratings yet
- Chemical Formula Writing Worksheet PDFDocument4 pagesChemical Formula Writing Worksheet PDFkezia0% (1)
- Pic16f84a PDFDocument88 pagesPic16f84a PDFBenjamin Michael LandisNo ratings yet
- Murray, Norris y BawendiDocument10 pagesMurray, Norris y BawendialkimiaNo ratings yet
- Proinert® Ig-55 Agent: Gaseous Suppression SystemDocument2 pagesProinert® Ig-55 Agent: Gaseous Suppression SystemMohammed SbeitanNo ratings yet
- Points, Pixels, and Gray Levels: Digitizing Image Data: James B. PawleyDocument22 pagesPoints, Pixels, and Gray Levels: Digitizing Image Data: James B. PawleyÖner AyhanNo ratings yet
- Full Paper IMPACT OF TEAMWORK ON ORGANIZATIONAL PRODUCTIVITY IN SOME SELECTED BASIC SCHOOLSDocument13 pagesFull Paper IMPACT OF TEAMWORK ON ORGANIZATIONAL PRODUCTIVITY IN SOME SELECTED BASIC SCHOOLSPrasad SirsangiNo ratings yet
- Updated NewDocument73 pagesUpdated NewAbhishek GaurNo ratings yet
- Linkedin Sales Automation Sequences That ConvertDocument53 pagesLinkedin Sales Automation Sequences That ConvertVictor BustillosNo ratings yet
- The Short-Form Revised Eysenck Personality Questionnaire A Hindi Edition (EPQRS-H)Document5 pagesThe Short-Form Revised Eysenck Personality Questionnaire A Hindi Edition (EPQRS-H)sashasaliny50% (2)
- HandyShare Install Guide EnglishDocument1 pageHandyShare Install Guide EnglishJulia AbrilNo ratings yet
- Therblig Chart (17 Motions)Document10 pagesTherblig Chart (17 Motions)Marianne Tajanlangit BebitNo ratings yet
- 0580 m24 Ms 32 (Provisional)Document10 pages0580 m24 Ms 32 (Provisional)Hassan HussainNo ratings yet
- Frank W Seeberger WWW - Educhem.Eu The Clausius-Clapeyron Equation 1 / 8Document8 pagesFrank W Seeberger WWW - Educhem.Eu The Clausius-Clapeyron Equation 1 / 8Ossama BohamdNo ratings yet
- Non Linear ProgrammingDocument109 pagesNon Linear ProgramminginftraNo ratings yet
- Workshop - Eleventh Grade - Week 6Document4 pagesWorkshop - Eleventh Grade - Week 6GustavoEcheverryNo ratings yet
- Pizza Ordering Python Project NewDocument25 pagesPizza Ordering Python Project NewUday TheNo ratings yet
- Adv Control & Robotic Lec 5Document31 pagesAdv Control & Robotic Lec 5key3hseNo ratings yet
- Ird ManualDocument44 pagesIrd ManualhcayetanoNo ratings yet
- Materi 7b Mohr CircleDocument35 pagesMateri 7b Mohr Circle17 / Imada Millatul KNo ratings yet
- Operations Manual For BMR 1000Document18 pagesOperations Manual For BMR 1000johnstn4544No ratings yet




















































































































Download as pdf or txt
You might also like
- LO4: Testing: Unit 18-Computer Systems HardwareDocument8 pagesLO4: Testing: Unit 18-Computer Systems Hardware20holmesloNo ratings yet
- Data Migration Projects TDDDocument30 pagesData Migration Projects TDDMadhuNo ratings yet
- F 584 C 6481 FDBDocument157 pagesF 584 C 6481 FDBgayathriNo ratings yet
- Cross-Cultural Reliability andDocument26 pagesCross-Cultural Reliability anderazermanuelNo ratings yet
- Chapter 3Document4 pagesChapter 3Dariann Jane HipolitoNo ratings yet
- 2022 Article 9908Document14 pages2022 Article 9908Harshita SinghNo ratings yet
- Development and Initial Validation of Personality Disorder Syndrome Scales For The MMPI-3Document16 pagesDevelopment and Initial Validation of Personality Disorder Syndrome Scales For The MMPI-3rushnaNo ratings yet
- WhitmanHolmesetal.2023MMPI 3NEOPI RincrementalvalidityDocument23 pagesWhitmanHolmesetal.2023MMPI 3NEOPI RincrementalvalidityrushnaNo ratings yet
- Comparison of Three Multigroup Ethnic Identity Measure Models: A Confirmatory Analysis With Female PopulationDocument10 pagesComparison of Three Multigroup Ethnic Identity Measure Models: A Confirmatory Analysis With Female PopulationAJHSSR JournalNo ratings yet
- Final Draft Essay 3Document5 pagesFinal Draft Essay 3api-709105209No ratings yet
- Running Head: Evaluating Significance of Findings 1Document4 pagesRunning Head: Evaluating Significance of Findings 1Juliet vutemeNo ratings yet
- The Sexist in You: Relationship of Entitlement To Ambivalent SexismDocument17 pagesThe Sexist in You: Relationship of Entitlement To Ambivalent SexismJ. ClimacoNo ratings yet
- Comparing The Validity of MMPI-3 Scores in Prehire Psychological Screenings of Male and Female Police Officer CandidatesDocument11 pagesComparing The Validity of MMPI-3 Scores in Prehire Psychological Screenings of Male and Female Police Officer CandidatesrushnaNo ratings yet
- 1Document5 pages1Mdeme CleptoNo ratings yet
- Gender Body Size and Social Relations in American High Schools - 50Document29 pagesGender Body Size and Social Relations in American High Schools - 50AgungNo ratings yet
- Catania 2015Document17 pagesCatania 2015Max SarmentoNo ratings yet
- Spss Data Assignment FinalDocument8 pagesSpss Data Assignment Finalapi-282530805No ratings yet
- Jackson Et Al. 2009. Reporting Practices in Confirmatory Factor Analysis An Overview and Some RecommendationsDocument18 pagesJackson Et Al. 2009. Reporting Practices in Confirmatory Factor Analysis An Overview and Some RecommendationslengocthangNo ratings yet
- Criminal PersonalityDocument17 pagesCriminal PersonalityLori JeffriesNo ratings yet
- 2020 Article 323Document13 pages2020 Article 323Sarra TekayaNo ratings yet
- Background and PurposeDocument6 pagesBackground and Purposerupa4No ratings yet
- Mata 2021Document11 pagesMata 2021Archondakis StavrosNo ratings yet
- Allen and Tussey, 2012Document15 pagesAllen and Tussey, 2012Ellis FreedmanNo ratings yet
- CTQDocument15 pagesCTQElliott FisherNo ratings yet
- Mortier 2018Document12 pagesMortier 2018PiramaxNo ratings yet
- A Meta-Analytic Review of Racial Discrimination Relationships To Health and CultureDocument18 pagesA Meta-Analytic Review of Racial Discrimination Relationships To Health and Cultureflavio rodasNo ratings yet
- Personality and Individual Differences: Graeme GallowayDocument5 pagesPersonality and Individual Differences: Graeme GallowayAndreea PîntiaNo ratings yet
- BirkmanvsbmtiDocument20 pagesBirkmanvsbmtiDavid BergeNo ratings yet
- Clinical Social Work Scope ofDocument12 pagesClinical Social Work Scope ofblackrandioresNo ratings yet
- Mcmi Sexual OfendersDocument17 pagesMcmi Sexual OfendersllamavioletNo ratings yet
- The Prevalence of Posttraumatic Stress Disorder and Its Severity Among Sexual and Gender Minority Individuals From Selected Support Groups in KenyaDocument9 pagesThe Prevalence of Posttraumatic Stress Disorder and Its Severity Among Sexual and Gender Minority Individuals From Selected Support Groups in KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter ThreeDocument3 pagesChapter Threeariwodola daramolaNo ratings yet
- A Critical Review of Objective Personality Inventories With Sex OffendersDocument28 pagesA Critical Review of Objective Personality Inventories With Sex Offenderstim radellNo ratings yet
- Research Critique PaperDocument6 pagesResearch Critique PaperJeremy RichuNo ratings yet
- Homicide Studies 2011 Nivette 103 31Document30 pagesHomicide Studies 2011 Nivette 103 31Corina IcaNo ratings yet
- Racial Ethnic Reporting Differences in Cancer Literature Regarding Machine Learning Vs A Radiologist - A Systematic Review and Meta-AnalysisDocument11 pagesRacial Ethnic Reporting Differences in Cancer Literature Regarding Machine Learning Vs A Radiologist - A Systematic Review and Meta-Analysiscerberus thanatosNo ratings yet
- American Association For Public Opinion Research, Oxford University Press The Public Opinion QuarterlyDocument31 pagesAmerican Association For Public Opinion Research, Oxford University Press The Public Opinion QuarterlyVLad2385No ratings yet
- University Students Perceptions and Attitudes Towards Sexual OffendersDocument16 pagesUniversity Students Perceptions and Attitudes Towards Sexual Offendersapi-607589196No ratings yet
- KeithkatDocument16 pagesKeithkatEunice Ann TiquiaNo ratings yet
- Meera Khemani 2039237 - Cia2 - br2Document3 pagesMeera Khemani 2039237 - Cia2 - br2Meera KhemaniNo ratings yet
- Personality Outcomes Across Samples Final MSDocument22 pagesPersonality Outcomes Across Samples Final MSpsleonardolagosNo ratings yet
- 2-S2.0-S0027968418301640-Am Imp PUMEDDocument14 pages2-S2.0-S0027968418301640-Am Imp PUMEDFabiana H. ShimabukuroNo ratings yet
- A Systematic Review of Empirical Research On Self-Reported Racism and HealthDocument14 pagesA Systematic Review of Empirical Research On Self-Reported Racism and Healthbob antonioNo ratings yet
- Personality Assessment in A Diverse Urban Sample: Brief ReportDocument6 pagesPersonality Assessment in A Diverse Urban Sample: Brief ReportNaga Sayana Srinivas KoneruNo ratings yet
- Kuhns WebDocument14 pagesKuhns WebRafael HenriqueNo ratings yet
- The Structure of The Statistics Anxiety Rating Scale: A Confirmatory Factor Analysis Using UK Psychology StudentsDocument24 pagesThe Structure of The Statistics Anxiety Rating Scale: A Confirmatory Factor Analysis Using UK Psychology StudentsTroy CabrillasNo ratings yet
- Chapter 3 Research MethodologyDocument8 pagesChapter 3 Research MethodologyMr PlagiarismNo ratings yet
- Using Latent Class Analysis To Model Prescription Medications in The Measurement of Falling Among A Community Elderly PopulationDocument7 pagesUsing Latent Class Analysis To Model Prescription Medications in The Measurement of Falling Among A Community Elderly PopulationIcaroNo ratings yet
- Epm318769 0 PDFDocument17 pagesEpm318769 0 PDFDristorXelaNo ratings yet
- Sampling TechniquesDocument23 pagesSampling TechniquesanilNo ratings yet
- How Prevalent Are Potentially Illegal Questions During Residency Interviews - A Follow-Up Study of Applicants To All Specialties in The National Resident Matching ProgramDocument8 pagesHow Prevalent Are Potentially Illegal Questions During Residency Interviews - A Follow-Up Study of Applicants To All Specialties in The National Resident Matching ProgramMohammad ZaherNo ratings yet
- Chapter 3 - SampleDocument5 pagesChapter 3 - SampleJe CoNo ratings yet
- Incidence of Anorexia Nervosa in Women: A Systematic Review and Meta-AnalysisDocument15 pagesIncidence of Anorexia Nervosa in Women: A Systematic Review and Meta-AnalysisandreaNo ratings yet
- Semenza-Et-Al-2022-Mental-Illness-And-Racial-Disparities-In-Correctional-Staff-Involved-Violence-An-Analysis-Of-Jails Mental 1 YesDocument28 pagesSemenza-Et-Al-2022-Mental-Illness-And-Racial-Disparities-In-Correctional-Staff-Involved-Violence-An-Analysis-Of-Jails Mental 1 YessilviaNo ratings yet
- FoMO341 354Document15 pagesFoMO341 354Phan Thanh ĐạtNo ratings yet
- Population Pharmacokinetics: Theory Practice: RecentlyDocument2 pagesPopulation Pharmacokinetics: Theory Practice: RecentlyabinchandrakumarNo ratings yet
- Audit DiscriminationDocument30 pagesAudit DiscriminationnachersNo ratings yet
- PsNP07-08.04 Blazevska - Stoilkovska, B., Naumova, KDocument15 pagesPsNP07-08.04 Blazevska - Stoilkovska, B., Naumova, KBorjan AdziskiNo ratings yet
- Jurnal Psikologi KlinisDocument6 pagesJurnal Psikologi KlinisRosaDeviNo ratings yet
- The Childhood Trauma Questionnaire in ADocument15 pagesThe Childhood Trauma Questionnaire in ATuấn KhangNo ratings yet
- Maureen Order 559755.86 Data Collection, Evaluating, Summarizing and Analysis Strategies 2pg FDocument4 pagesMaureen Order 559755.86 Data Collection, Evaluating, Summarizing and Analysis Strategies 2pg Fwriter lonicNo ratings yet
- Qualitative Research:: Intelligence for College StudentsFrom EverandQualitative Research:: Intelligence for College StudentsRating: 4 out of 5 stars4/5 (1)
- Psychiatric Disorders in Term-Born Children With Marginally Low Birth Weight: A Population-Based StudyDocument11 pagesPsychiatric Disorders in Term-Born Children With Marginally Low Birth Weight: A Population-Based StudyrushnaNo ratings yet
- Short Term Neonatal and Long Term Neurodevelopmental Outcome of Children Born Term Low Birth WeightDocument8 pagesShort Term Neonatal and Long Term Neurodevelopmental Outcome of Children Born Term Low Birth WeightrushnaNo ratings yet
- Machine Learning Applied To Student Attentiveness Detection: Using Emotional and Non Emotional MeasuresDocument21 pagesMachine Learning Applied To Student Attentiveness Detection: Using Emotional and Non Emotional MeasuresrushnaNo ratings yet
- Systematic Literature Review and Bibliometric Analysis On Virtual Reality and EducationDocument38 pagesSystematic Literature Review and Bibliometric Analysis On Virtual Reality and EducationrushnaNo ratings yet
- Autism in Lebanon Looking Back To Inform The FutureDocument10 pagesAutism in Lebanon Looking Back To Inform The FuturerushnaNo ratings yet
- Hosozawa 2024 Oi 231548 1705094509.26292Document12 pagesHosozawa 2024 Oi 231548 1705094509.26292rushnaNo ratings yet
- WhitmanHolmesetal.2023MMPI 3NEOPI RincrementalvalidityDocument23 pagesWhitmanHolmesetal.2023MMPI 3NEOPI RincrementalvalidityrushnaNo ratings yet
- SSRN Id3799204Document20 pagesSSRN Id3799204rushnaNo ratings yet
- Neuropsychological AssessmentsDocument48 pagesNeuropsychological AssessmentsrushnaNo ratings yet
- The Role of Spatial Ability in Mixed Reality Learning With The HololensDocument12 pagesThe Role of Spatial Ability in Mixed Reality Learning With The HololensrushnaNo ratings yet
- Ucar Icatces ProceedingDocument15 pagesUcar Icatces ProceedingrushnaNo ratings yet
- Research Methods Tools and TechniquesDocument84 pagesResearch Methods Tools and TechniquesrushnaNo ratings yet
- Comment: Materials and Devices For Immersive Virtual RealityDocument3 pagesComment: Materials and Devices For Immersive Virtual RealityrushnaNo ratings yet
- Psychopathology of adults-CODocument17 pagesPsychopathology of adults-COrushnaNo ratings yet
- VR4Health: Personalized Teaching and Learning Anatomy Using VRDocument11 pagesVR4Health: Personalized Teaching and Learning Anatomy Using VRrushnaNo ratings yet
- What Are Research Objectives and How To Write ThemDocument9 pagesWhat Are Research Objectives and How To Write ThemrushnaNo ratings yet
- Disruptive DisorderDocument24 pagesDisruptive DisorderrushnaNo ratings yet
- BGT 2Document29 pagesBGT 2rushnaNo ratings yet
- Psychodiagnostic Assessment of ChildrenDocument26 pagesPsychodiagnostic Assessment of ChildrenrushnaNo ratings yet
- Research Methodology-CODocument5 pagesResearch Methodology-COrushnaNo ratings yet
- Neuropsychological AssessmentDocument35 pagesNeuropsychological AssessmentrushnaNo ratings yet
- Neuropsychological AssessmentDocument27 pagesNeuropsychological AssessmentrushnaNo ratings yet
- Psychosocial AssesmentDocument37 pagesPsychosocial AssesmentrushnaNo ratings yet
- Course Outline On Psychodiagnostic Assessment of ChildrenDocument5 pagesCourse Outline On Psychodiagnostic Assessment of ChildrenrushnaNo ratings yet
- Endocrinology LectureDocument40 pagesEndocrinology LecturerushnaNo ratings yet
- PsychopharmacologyDocument59 pagesPsychopharmacologyrushnaNo ratings yet
- NeurotransmittersDocument29 pagesNeurotransmittersrushnaNo ratings yet
- Antipsychotics PsychopharmacologyDocument15 pagesAntipsychotics PsychopharmacologyrushnaNo ratings yet
- ADHDDocument29 pagesADHDrushnaNo ratings yet
- Psychopathology-Multicultral UnderstandingDocument21 pagesPsychopathology-Multicultral UnderstandingrushnaNo ratings yet
- Pipe Bend RadiusDocument8 pagesPipe Bend RadiusAdagharaNo ratings yet
- Configurar Session-Ttl en FortigateDocument2 pagesConfigurar Session-Ttl en FortigatemasmisemNo ratings yet
- PC 2201Document12 pagesPC 2201Irwan SamtaniNo ratings yet
- SSC CGL 2 Dec 2022 Shift 3 Question PaperDocument27 pagesSSC CGL 2 Dec 2022 Shift 3 Question Papernakul yadavNo ratings yet
- Home Work Assignment - 1Document4 pagesHome Work Assignment - 1Agnivesh SharmaNo ratings yet
- Python Modules: What Is A Module?Document9 pagesPython Modules: What Is A Module?Krishnaprasad kNo ratings yet
- Oscillatory Motion: Multiple ChoiceDocument14 pagesOscillatory Motion: Multiple ChoiceCamilo ValenciaNo ratings yet
- Chemical Formula Writing Worksheet PDFDocument4 pagesChemical Formula Writing Worksheet PDFkezia0% (1)
- Pic16f84a PDFDocument88 pagesPic16f84a PDFBenjamin Michael LandisNo ratings yet
- Murray, Norris y BawendiDocument10 pagesMurray, Norris y BawendialkimiaNo ratings yet
- Proinert® Ig-55 Agent: Gaseous Suppression SystemDocument2 pagesProinert® Ig-55 Agent: Gaseous Suppression SystemMohammed SbeitanNo ratings yet
- Points, Pixels, and Gray Levels: Digitizing Image Data: James B. PawleyDocument22 pagesPoints, Pixels, and Gray Levels: Digitizing Image Data: James B. PawleyÖner AyhanNo ratings yet
- Full Paper IMPACT OF TEAMWORK ON ORGANIZATIONAL PRODUCTIVITY IN SOME SELECTED BASIC SCHOOLSDocument13 pagesFull Paper IMPACT OF TEAMWORK ON ORGANIZATIONAL PRODUCTIVITY IN SOME SELECTED BASIC SCHOOLSPrasad SirsangiNo ratings yet
- Updated NewDocument73 pagesUpdated NewAbhishek GaurNo ratings yet
- Linkedin Sales Automation Sequences That ConvertDocument53 pagesLinkedin Sales Automation Sequences That ConvertVictor BustillosNo ratings yet
- The Short-Form Revised Eysenck Personality Questionnaire A Hindi Edition (EPQRS-H)Document5 pagesThe Short-Form Revised Eysenck Personality Questionnaire A Hindi Edition (EPQRS-H)sashasaliny50% (2)
- HandyShare Install Guide EnglishDocument1 pageHandyShare Install Guide EnglishJulia AbrilNo ratings yet
- Therblig Chart (17 Motions)Document10 pagesTherblig Chart (17 Motions)Marianne Tajanlangit BebitNo ratings yet
- 0580 m24 Ms 32 (Provisional)Document10 pages0580 m24 Ms 32 (Provisional)Hassan HussainNo ratings yet
- Frank W Seeberger WWW - Educhem.Eu The Clausius-Clapeyron Equation 1 / 8Document8 pagesFrank W Seeberger WWW - Educhem.Eu The Clausius-Clapeyron Equation 1 / 8Ossama BohamdNo ratings yet
- Non Linear ProgrammingDocument109 pagesNon Linear ProgramminginftraNo ratings yet
- Workshop - Eleventh Grade - Week 6Document4 pagesWorkshop - Eleventh Grade - Week 6GustavoEcheverryNo ratings yet
- Pizza Ordering Python Project NewDocument25 pagesPizza Ordering Python Project NewUday TheNo ratings yet
- Adv Control & Robotic Lec 5Document31 pagesAdv Control & Robotic Lec 5key3hseNo ratings yet
- Ird ManualDocument44 pagesIrd ManualhcayetanoNo ratings yet
- Materi 7b Mohr CircleDocument35 pagesMateri 7b Mohr Circle17 / Imada Millatul KNo ratings yet
- Operations Manual For BMR 1000Document18 pagesOperations Manual For BMR 1000johnstn4544No ratings yet