Professional Documents
Culture Documents
Articles: Background
Articles: Background
Uploaded by
maleticjOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Articles: Background
Articles: Background
Uploaded by
maleticjCopyright:
Available Formats
Articles
5-year analysis of neoadjuvant pertuzumab and trastuzumab
in patients with locally advanced, inflammatory, or
early-stage HER2-positive breast cancer (NeoSphere):
a multicentre, open-label, phase 2 randomised trial
Luca Gianni, Tadeusz Pienkowski, Young-Hyuck Im, Ling-Ming Tseng, Mei-Ching Liu, Ana Lluch, Elżbieta Starosławska,
Juan de la Haba-Rodriguez, Seock-Ah Im, Jose Luiz Pedrini, Brigitte Poirier, Paolo Morandi, Vladimir Semiglazov, Vichien Srimuninnimit,
Giulia Valeria Bianchi, Domenico Magazzù, Virginia McNally, Hannah Douthwaite, Graham Ross, Pinuccia Valagussa
Summary
Background In the primary analysis of the NeoSphere trial, patients given neoadjuvant pertuzumab, trastuzumab, and Lancet Oncol 2016; 17: 791–800
docetaxel showed a significantly improved pathological complete response compared with those given trastuzumab Published Online
and docetaxel after surgery. Here, we report 5-year progression-free survival, disease-free survival, and safety. May 11, 2016
http://dx.doi.org/10.1016/
S1470-2045(16)00163-7
Methods In this multicentre, open-label, phase 2 randomised trial in hospitals and medical clinics, treatment-naive
See Comment page 693
adults with locally advanced, inflammatory, or early-stage HER2-positive breast cancer were randomly assigned (1:1:1:1)
Oncologia Medica, San Raffaele
to receive four neoadjuvant cycles of trastuzumab (8 mg/kg loading dose, followed by 6 mg/kg every 3 weeks) plus Cancer Centre, Milan, Italy
docetaxel (75 mg/m² every 3 weeks, increasing to 100 mg/m² from cycle 2 if tolerated; group A), pertuzumab (840 mg (Prof L Gianni MD);
loading dose, followed by 420 mg every 3 weeks) and trastuzumab plus docetaxel (group B), pertuzumab and Postgraduate Medical
trastuzumab (group C), or pertuzumab and docetaxel (group D). After surgery, patients received three cycles of FEC Education Centre, Warsaw,
Poland (Prof T Pienkowski MD);
(fluorouracil 600 mg/m², epirubicin 90 mg/m², and cyclophosphamide 600 mg/m²) every 3 weeks (patients in group Samsung Medical Centre,
C received four cycles of docetaxel prior to FEC), and trastuzumab 6 mg/kg every 3 weeks to complete 1 year’s treatment Seoul, South Korea
(17 cycles in total). Randomisation was done by a central centre using dynamic allocation, stratified by operable, locally (Prof Y-H Im MD);
advanced, and inflammatory breast cancer, and by oestrogen and/or progesterone receptor positivity. Safety analyses Taipei-Veterans General
Hospital, National Yang-Ming
were done according to treatment received. The primary endpoint (pathological complete response) was previously University, Taipei, Taiwan
reported; secondary endpoints reported here are 5-year progression-free survival (analysed in the intention-to-treat (L-M Tseng MD); Koo
population) and disease-free survival (analysed in patients who had surgery). Secondary and exploratory analyses were Foundation Sun Yat-Sen Cancer
Center, Taipei, Taiwan
not powered for formal statistical hypothesis testing, and therefore results are for descriptive purposes only. The study
(M-C Liu MD); Hospital Clínico
ended on Sept 22, 2014 (last patient, last visit). This study is registered with ClinicalTrials.gov, number NCT00545688. Universitario, INCLIVA Health
Research Institute, University
Findings Between Dec 17, 2007, and Dec 22, 2009, 417 eligible patients were randomly assigned to group A (107 patients), of Valencia, Valencia, Spain
(A Lluch MD); St John’s Cancer
group B (107 patients), group C (107 patients), or group D (96 patients). One patient in group A withdrew before
Centre, Lublin, Poland
treatment. One patient assigned to group D received group A treatment, one patient assigned to group D received (Prof E Starosławska MD);
group B treatment, and one patient assigned to group B received group C treatment. At clinical cutoff, 87 patients had Oncology Department,
progressed or died. 5-year progression-free survival rates were 81% (95% CI 71–87) for group A, 86% (77–91) for Maimonides Institute of
Biomedical Research, Reina
group B, 73% (64–81) for group C, and 73% (63–81) for group D (hazard ratios 0·69 [95% CI 0·34–1·40] group B vs
Sofía Hospital, University of
group A, 1·25 [0·68–2·30] group C vs group A, and 2·05 [1·07–3·93] group D vs group B). Disease-free survival results Córdoba, Córdoba, Spain
were consistent with progression-free survival results and were 81% (95% CI 72–88) for group A, 84% (72–91) for (J de la Haba-Rodriguez MD);
group B, 80% (70–86) for group C, and 75% (64–83) for group D. Patients who achieved total pathological complete Division of Hematology/
Medical Oncology, Department
response (all groups combined) had longer progression-free survival compared with patients who did not (85% [76–91]
of Internal Medicine, Cancer
in patients who achieved total pathological response vs 76% [71–81] in patients who did not achieve total pathological Research Institute, Seoul
response; hazard ratio 0·54 [95% CI 0·29–1·00]). There were no new or long-term safety concerns and tolerability was National University College of
similar across groups (neoadjuvant and adjuvant treatment periods combined). The most common grade 3 or worse Medicine, Seoul, South Korea
(Prof S-A Im MD); Hospital
adverse events were neutropenia (group A: 71 [66%] of 107 patients; group B: 59 [55%] of 107; group C: 40 [37%] of 108; Nossa Senhora da Conceição,
group D: 60 [64%] of 94), febrile neutropenia (group A: 10 [9%]; group B: 12 [11%]; group C: 5 [5%]; group D: 15 [16%]), Hospital Ernesto Dornelles,
and leucopenia (group A: 13 [12%]; group B: 6 [6%]; group C: 4 [4%]; group D: 8 [9%]). The number of patients with one Porto Alegre, Brazil
or more serious adverse event was similar across groups (19–22 serious adverse events per group in 18–22% of patients). (J L Pedrini MD); Hôpital du
Saint-Sacrément, Centre
Hospitalier Affilié Universitaire
Interpretation Progression-free survival and disease-free survival at 5-year follow-up show large and overlapping CIs, de Québec, Québec, Canada
but support the primary endpoint (pathological complete response) and suggest that neoadjuvant pertuzumab is (B Poirier MD); Medical
beneficial when combined with trastuzumab and docetaxel. Additionally, they suggest that total pathological complete Oncology Department,
Ospedale dell’Angelo Mestre,
response could be an early indicator of long-term outcome in early-stage HER2-positive breast cancer. Ospedale San Giovanni e Paolo
Venezia, Venice, Italy
Funding F Hoffmann-La Roche. (P Morandi MD); N N Petrov
www.thelancet.com/oncology Vol 17 June 2016 791
Articles
Research Institute of Oncology,
St Petersburg, Russia Research in context
(Prof V Semiglazov MD); Medical
Oncology Unit, Department of Evidence before this study shown that pathological complete response in the breast or total
Medicine, Siriraj Hospital, The addition of pertuzumab to trastuzumab and docetaxel for pathological complete response is likely to predict clinical benefit
Bangkok, Thailand the first-line treatment of patients with HER2-positive in patients with early-stage HER2-positive breast cancer.
(Prof V Srimuninnimit MD);
Oncologia Medica 1,
metastatic breast cancer significantly improved both
Added value of this study
Fondazione IRCCS Istituto progression-free survival and overall survival, and led to the
NeoSphere is the first neoadjuvant study of pertuzumab to
Nazionale Tumori, Milan, Italy approval of pertuzumab, in combination with trastuzumab and
(G V Bianchi MD); Fondazione report mature progression-free survival and disease-free
docetaxel, in this setting. The primary results of the NeoSphere
Michelangelo, Milan, Italy survival data. Furthermore, it adds to the body of evidence
(D Magazzù PhD,
study showed that pathological complete response in the breast
suggesting an association between pathological complete
P Valagussa BS); Roche Products was significantly improved by the addition of pertuzumab to
response in the breast or total pathological complete response
Limited, Welwyn, UK trastuzumab and docetaxel. NeoSphere’s results, in combination
(V McNally PhD, and improved long-term outcomes in early-stage
with the results from the neoadjuvant TRYPHAENA study, led the
H Douthwaite MSc, HER2-positive breast cancer.
G Ross FFPM); and AstraZeneca,
US Food and Drug Administration in 2013, and more recently the
Melbourn, Cambridge, UK European Medicines Agency in 2015, to grant pertuzumab Implications of all the available evidence
(G Ross) accelerated approval in the neoadjuvant setting, making The results from NeoSphere suggest that progression-free
Correspondence to: pertuzumab the first drug to be approved using pathological survival is improved when neoadjuvant pertuzumab is
Prof Luca Gianni, Department of complete response as an endpoint. We now report 5-year administered in combination with trastuzumab and
Medical Oncology, San Raffaele
Cancer Centre, Via Olgettina 60,
progression-free survival and disease-free survival results, docetaxel. It is also noteworthy that disease-free survival after
20132 Milan, Italy exploratory associations between total pathological complete four cycles of neoadjuvant pertuzumab, trastuzumab, and
gianni.luca@hsr.it response and progression-free survival, and long-term safety. docetaxel seemed to be better than disease-free survival after
To put the findings of NeoSphere into context with respect to neoadjuvant docetaxel and trastuzumab despite identical
associations between total pathological complete response and adjuvant therapy. However, these results must be intrepeted
clinical benefit, we searched PubMed plus abstracts from the with caution as NeoSphere is a phase 2 study, and was not
American Society of Clinical Oncology annual meetings, the designed or powered to detect differences in survival
San Antonio Breast Cancer Symposium annual meetings, outcomes. Further trials such as the phase 3 APHINITY trial
the European Society for Medical Oncology biennial meetings, (NCT01358877), which is assessing pertuzumab,
and the European Cancer Congress biennial meetings with the trastuzumab, and chemotherapy in the adjuvant setting, may
terms “breast cancer”, “HER2”, “long term”, and “pathologic(al) provide more information on the efficacy of this drug
complete response”, selecting relevant English-language combination in early-stage breast cancer.
publications from Dec 1, 2010, to Dec 1, 2015. Studies have
Introduction four cycles of neoadjuvant pertuzumab and trastuzumab
The clinical benefit of combining the HER2-directed plus docetaxel, had a significant improvement (16·8%) in
monoclonal antibodies pertuzumab and trastuzumab pathological complete response in the breast (defined as
was first shown in patients with HER2-positive absence of invasive cancer in the breast, regardless of
metastatic breast cancer whose disease had progressed ductal carcinoma in situ; 49 [46%] of 107 patients,
during previous trastuzumab therapy.1 On the basis 95% CI 36·1–55·7), compared with patients who received
of those results, pertuzumab, trastuzumab, and trastuzumab plus docetaxel (31 [29%] of 107 patients,
chemotherapy were tested in the HER2-positive 20·6–38·5; p=0·0141).2 Similarly, there was a 17·8%
neoadjuvant setting in the phase 2 NeoSphere2 and increase in total pathological complete response (defined
TRYPHAENA studies,3 and in the phase 3 CLEOPATRA as absence of invasive cancer in the breast and axillary
trial in metastatic breast cancer.4,5 In TRYPHAENA,3 a nodes, regardless of ductal carcinoma in situ) in patients
high proportion of patients achieved a pathological who received pertuzumab and trastuzumab plus
complete response (57·3–66·2%) with pertuzumab docetaxel (42 [39%] of 107 patients, 95% CI 30·0–49·2)
and trastuzumab in combination with standard compared with patients who received trastuzumab
anthracycline-based and non-anthracycline-based and docetaxel (23 [22%] of 107 patients, 14·1–30·5).2
neoadjuvant regimens.In CLEOPATRA,4,5 first-line NeoSphere also assessed neoadjuvant pertuzumab and
treatment with pertuzumab and trastuzumab plus trastuzumab without chemotherapy, and pertuzumab
docetaxel significantly improved progression-free plus docetaxel. Both combinations were active but were
survival and overall survival in patients with less so than trastuzumab plus docetaxel or than both
HER2-positive metastatic breast cancer, compared with antibodies plus docetaxel.2
placebo, trastuzumab, and docetaxel. After surgery, patients in NeoSphere received additional
The primary analysis of NeoSphere2 showed that chemotherapy and adjuvant trastuzumab to provide all
patients with locally advanced, inflammatory, or patients with optimal therapy for operable HER2-positive
early-stage HER2-positive breast cancer, who received breast cancer.
792 www.thelancet.com/oncology Vol 17 June 2016
Articles
In this second Article, we report prespecified secondary randomly assigned via a central centre (Almac Clinical
endpoints of progression-free survival, disease-free Technologies, Yardley, PA, USA), using an interactive
survival, and safety in NeoSphere, 5 years after voice response system and dynamic allocation, stratified
randomisation of the last patient. We also examined the by operable, locally advanced, and inflammatory breast
association between total pathological complete response cancer, and by oestrogen or progesterone receptor
and progression-free survival. Previous studies indicated positivity. The trial was open label.
that pathological complete response is likely to predict
clinical benefit in patients with early-stage HER2-positive Procedures
breast cancer.6–12 We used total pathological complete All treatment groups received four cycles of neo-
response rather than pathological complete response in adjuvant treatment. Neoadjuvant treatment was
the breast to align with the US Food and Drug given intravenously every 3 weeks and consisted of
Administration (FDA) and the European Medicines trastuzumab plus docetaxel (group A), pertuzumab and
Agency (EMA) guidance.13,14 trastuzumab plus docetaxel (group B), pertuzumab
and trastuzumab (group C), or pertuzumab plus
Methods docetaxel (group D). Trastuzumab was given at 8 mg/kg
Study design and participants loading dose followed by 6 mg/kg maintenance dose;
The study design and patient eligibility criteria have been pertuzumab was given at an 840 mg loading dose
reported previously.2 NeoSphere was a randomised, followed by 420 mg maintenance dose; and docetaxel
multicentre, international, open-label, phase 2 study. was given at 75 mg/m², increasing to 100 mg/m² from
Patients were recruited from 59 centres in 16 countries. cycle 2 onwards if tolerated. Eligible patients (ie, those
Eligible patients had operable (T2–3, N0–1, M0), locally who hadn’t withdrawn; appendix p 20) then had surgery See Online for appendix
advanced (T2–3, N2–N3, M0; T4a–c, any N, M0), or and assessment of pathological complete response,
inflammatory (T4d, any N, M0) HER2-positive breast followed by adjuvant treatment: three cycles of
cancer. Primary tumours were larger than 2 cm in intravenous FEC (fluorouracil 600 mg/m², epirubicin
diameter, as measured by mammogram and clinical 90 mg/m², and cyclophosphamide 600 mg/m²) every
breast examination, and HER2 positivity was centrally 3 weeks in all groups except for group C, in
confirmed (immunohistochemistry 3+, or 2+ and positive which patients received four cycles of docetaxel before
for fluorescence or chromogenic in-situ hybridisation). FEC. All patients received concomitant intravenous
Eligible patients were aged 18 years or older, had a trastuzumab 6 mg/kg every 3 weeks to complete 1 year’s
baseline left ventricular ejection fraction of 55% or more, treatment (17 cycles in total). Radiotherapy and hormone
and an Eastern Cooperative Oncology Group (ECOG) therapy, if indicated, were given in accordance with local
performance status of 0 or 1, and had not received any guidelines. Dose reductions were not permitted for
previous anti-cancer therapy. Key exclusion criteria were pertuzumab and trastuzumab. Delays to administration
metastatic disease (stage IV) or bilateral breast cancer, of pertuzumab and trastuzumab were permitted to
other malignancies, impaired liver function, inadequate assess or treat adverse events. During neoadjuvant
bone marrow or renal function, impaired cardiac treatment, only two dose delays of up to 2 weeks
function, uncontrolled hypertension, pregnancy, and each were permitted; during adjuvant treatment,
refusal to use contraception. There was no protocol- trastuzumab delays were permitted as required.
specified exclusion based on life expectancy. Pertuzumab and trastuzumab infusions could be
NeoSphere was conducted in accordance with Good slowed down (prespecified infusion rate decreased)
Clinical Practice guidelines and the Declaration of or interrupted (infusion temporarily stopped and
Helsinki. Approval for the protocol and any modifications subsequently restarted, usually on the same day but
was obtained from independent ethics committees. anytime within the same treatment cycle was permitted)
All patients provided written informed consent. for infusion-related symptoms (eg, fever or chills) and
The study protocol is available online. resumed once symptoms abated. Docetaxel dose could For the study protocol see
be reduced from 100 mg/m² to 75 mg/m² and then to http://www.roche-trials.com/
trialDetailsGet.
Randomisation and masking 60 mg/m² if non-haematological toxicities worse than action?studyNumber=WO20697
Randomisation methods have been reported previously.2 grade 2 occurred (excluding alopecia), after which dis-
Patients were randomly assigned (1:1:1:1) to one of continuation was required. A docetaxel dose delay of
four neoadjuvant treatment groups, in which patients 2 weeks was permitted per cycle (for myelosuppression,
received trastuzumab plus docetaxel (group A), hepatic dysfunction, and other dose-limiting toxicities),
pertuzumab and trastuzumab plus docetaxel (group B), with one further dose delay of 2 weeks allowed
pertuzumab and trastuzumab (group C), or pertuzumab before study discontinuation was required. Docetaxel
plus docetaxel (group D). infusions could be slowed down or interrupted for
Group D was added after 29 patients had been recruited minor symptoms such as flushing or local cutaneous
to the study to assess the activity of pertuzumab and reactions and resumed once symptoms abated.
docetaxel without trastuzumab. Eligible patients were FEC dose reductions were allowed in accordance with
www.thelancet.com/oncology Vol 17 June 2016 793
Articles
the relevant summary of product characteristics. Statistical analysis
Patients could withdraw from the study at any time for Patients who were enrolled but did not receive any
any reason. Investigators could also withdraw patients study treatment were not included in any analyses.
in the event of intercurrent illness, adverse events, We calculated pathological complete response for each
disease progression, protocol violation, cure, admin- group by dividing the number of patients achieving
istrative reasons, or any other reason. pathological complete response by the intention-to-treat
Clinical breast examinations were done every cycle up population (all randomly assigned patients). A pathological
to 7 days prior to dosing. Patients had a mammogram complete response of 25% was expected in group A and
and ultrasonography (if required by local practice) group D and 40% in group B or group C.17 A sample size
before surgery (cycle 4) and 28 days after their last study of 400 patients was planned to provide 80% power to
treatment. Physical examinations were done and vital detect an absolute difference in pathological complete
signs and ECOG performance status were measured response of 15% between groups. Three comparisons
every cycle and then every 3 months for 1 year, and every were planned for pathological complete response (group A
6 months for 3 years during follow-up. Left ventricular vs group B, group A vs group C, and group B vs group D)
ejection fraction was measured by echocardiography using a two-sided Cochran-Mantel-Haenszel test at an
(or multi-gated acquisition) every two cycles during α level of 0·2, stratified by operable, locally advanced,
neoadjuvant treatment and every two to three cycles and inflammatory breast cancer and hormone receptor
during adjuvant treatment, and then every 6 months positivity. Formal comparison of group D with group A
for 2 years. Blood counts and laboratory parameters was not prespecified because group D was added to the
were assessed every cycle and then as needed study after a protocol amendment.2
during follow-up (see study protocol for details). Chest NeoSphere was not designed or powered to detect
radiography, liver or skeletal ultrasonography, and bone treatment differences with respect to secondary efficacy
scans were done as needed during follow-up. Adverse endpoints; therefore, results cannot claim statistical
events and serious adverse events were monitored significance and are for descriptive purposes only. We did
continuously until 28 days after the last treatment progression-free survival analyses in the intention-to-treat
and were graded according to standard criteria.15,16 population and disease-free survival analyses on all
Related adverse events and serious adverse events, and patients who underwent surgery. We estimated 5-year
unrelated severe or life-threatening adverse events were progression-free survival and disease-free survival rates
still reportable after this period. Symptomatic left for each group using the Kaplan-Meier method. Patients
ventricular systolic dysfunction grade 3 or worse, who withdrew without documented progression were
reportable as congestive heart failure, was reportable censored at the date of the last assessment when they were
up to 2 years after treatment. Pathological complete known to be free from progressive disease or free from
response in the breast was assessed locally, and to disease. We used the Cox proportional hazard model,
ensure consistency, blinded data were reviewed by a stratified by operable, locally advanced, inflammatory
consultant pathologist at regular intervals.2 Primary breast cancer, and hormone receptor-positive disease, to
tumour samples were collected at study entry and at estimate hazard ratios (HRs), and corresponding 95% CIs.
surgery to assess biomarkers that could predict We analysed exploratory total pathological complete
response to treatment. response–progression-free survival associations using
multivariate Cox modelling. We used Statistical Analysis
Outcomes Software version 9.2 for analyses. The safety population
The primary endpoint (pathological complete response included all patients who received at least one dose of
in the breast) and the secondary endpoints of clinical study treatment and who had at least one safety assessment
response rate, time to clinical response, breast- done at baseline. For safety analyses patients were assigned
conserving surgery rate, and safety in the neoadjuvant to treatment groups as treated. This study is registered
period were reported in 2012.2 Biomarker analyses will with ClinicalTrials.gov, number NCT00545688.
be reported separately. In this Article, we report the
secondary endpoints of progression-free survival Role of the funding source
(defined as the time from the date of randomisation to F Hoffmann-La Roche funded the study, provided study
the first documentation of progressive disease or death; drugs, and was involved in study design, protocol
equivalent to event-free survival),13 disease-free survival development, regulatory and ethics approvals, safety
(time from the first date of no disease [ie, date of monitoring and reporting, data management, data analysis,
surgery] to the first documentation of progressive and interpretation. LG, PV, DM, GR, VM, and HD had
disease or death), and safety for the overall and access to the raw patient data. The corresponding author
adjuvant treatment periods. We did exploratory (LG) was directly involved in the design of the trial, had full
subgroup analyses for progression-free survival by access to all of the data, and had the final responsibility to
total pathological complete response and hormone submit for publication. The sponsor funded third-party
receptor status. writing assistance provided by Debbie Briggs.
794 www.thelancet.com/oncology Vol 17 June 2016
Articles
Results of 107 in group B, 27 (25%) of 107 in group C, and
Between Dec 17, 2007, and Dec 22, 2009, 417 patients 24 (25%) of 96 in group D. 5-year progression-free
were randomly assigned to treatment groups: 107 to survival rates were higher in group B (86% [95% CI
group A, 107 to group B, 107 to group C, and 96 to 77–91]) than in group A (81% [71–87]; HR 0·69
group D.2 Baseline characteristics were balanced across [95% CI 0·34–1·40]), lower in group C (73% [64–81]) than
groups (appendix p 9). Patient disposition (trial profile) in group A (HR 1·25 [0·68–2·30]), and lower in group D
is shown in the appendix (p 20). One patient randomly (73% [63–81]) than in group B (HR 2·05 [1·07–3·93];
assigned to group D received group A treatment, figure 1A). Disease-free survival analyses were done on
one patient assigned to group D received group B the 392 patients who underwent surgery. Disease-free
treatment, and one patient assigned to group B received
group C treatment in error. 392 (94%) of 417 patients had A
surgery as planned, and all those who did so had a valid 100
assessment of pathological response. Time on study was 90
balanced across groups, with most patients on study for 80
Progression-free survival (%)
48 months or longer (84 [79%] in group A, 88 [82%] in
70
group B, 86 [80%] in group C, and 69 [72% in group D).
60
At the final clinical cutoff (Oct 20, 2014), median
time on study, including post-treatment follow-up, was 50
Number of Number of 5-year progression-free Hazard ratio
approximately 60 months (group A: 60·5 months 40
patients events (%) survival (95% CI) (95% CI)
[IQR 53–62]; group B: 61·2 months [59–63], group C: 30
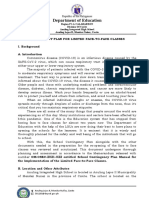
Group A 107 19 (18) 81% (71–87)
60·5 months [52–62]; group D: 62·3 [46–64]). 20 Group B 107 17 (16) 86% (77–91) 0·69 (0·34–1·40)
Detailed treatment exposure by group is provided in 10 Group C 107 27 (25) 73% (64–81) 1·25 (0·68–2·30)
Group D 96 24 (25) 73% (63–81) 2·05 (1·07–3·93)
the appendix (p 10). The median number of neoadjuvant 0
pertuzumab cycles received in groups B, C, and D was 0 12 24 36 48 60
4 (range 1–4, IQR 4–4). 290 (94%) of 309 patients Number at risk
Months after randomisation
completed the planned four cycles, with 101 (8%) of Group A 107 101 89 83 78 58
Group B 107 99 94 88 86 63
1203 cycles delayed, slowed down, interrupted, or Group C 107 93 86 80 77 55
discontinued. Most patients completed the planned Group D 96 85 76 72 69 57
17 trastuzumab cycles (98 [92%] of 107 in group A,
89 [83%] of 107 in group B, 88 [81%] of 108 in group C, B
100
and 73 [78%] of 94 in group D). The median number of
trastuzumab cycles received was 17 (range 1–18, IQR 17–17). 90
One patient in group B received an additional 80
Disease-free survival (%)
trastuzumab cycle because of a site administration error 70
(recorded as a major protocol violation). The percentage 60
of delayed, slowed down, interrupted, or discontinued 50
trastuzumab cycles was similar across groups 40
Number of Number of 5-year disease-free Hazard ratio
(4·7–5·4%). Most delays or interruptions were for patients events (%) survival (95% CI) (95% CI)
30
one cycle, and nearly all delays lasted 14 days or fewer. Group A 103 18 (18) 81% (72–88)
20 Group B 101 15 (15) 84% (72–91) 0·60 (0·28–1·27)
The median docetaxel intensity in group C during Group C 96 19 (20) 80% (70–86) 0·83 (0·42–1·64)
adjuvant treatment was 29·6 mg/m² per week 10
Group D 92 22 (24) 75% (64–83) 2·16 (1·08–4·32)
(range 19–33), close to the planned 31·25 mg/m² per 0
0 12 24 36 48 60
week, and similar to that received during neoadjuvant Months after surgery
treatment for groups A, B, and D. 81 (75%) of 108 patients Number at risk
Group A 103 92 85 79 77 12
in group C completed four cycles of docetaxel, compared Group B 101 96 92 88 85 17
with more than 94% in groups A, B, and D (appendix p 10). Group C 96 91 87 81 75 10
Group D 92 81 76 72 66 29
The percentage of delayed, slowed down, interrupted,
or discontinued docetaxel cycles was similar across Figure 1: Progression-free survival and disease-free survival
groups (13·7–19·6%). Adjuvant FEC was completed in (A) Kaplan-Meier estimates of progression-free survival in the intention-to-treat population, 5 years after random
103 (100%) of 103 patients in group A, 96 (94%) of 102 in assignment of the final patient. Three late events occurred in group B: two cases of progressive disease at 63 and
71 months, and one death due to an unrelated cerebrovascular accident without progressive disease at 76 months.
group B, 85 (90%) of 94 in group C, and 85 (97%) of
(B) Kaplan-Meier estimates of disease-free survival in all patients who underwent surgery, 5 years after random
88 in group D. The median number of cycles of FEC assignment of the final patient. The hazard ratio for groups B and C is with respect to group A, whereas the hazard
received was 3 (range 1–3, IQR 3–3). Radiotherapy to the ratio for group D is with respect to group B. Two late events occurred in group B: one case of progressive disease at
breast or axilla and adjuvant hormonal treatment were 67 months, and one death due to an unrelated cerebrovascular accident without progressive disease at 72 months.
Tick marks indicate the times at which events were recorded. The Kaplan-Meier curves are truncated at 60 months
evenly distributed across groups.
(the end of scheduled follow-up). However, summary statistics shown here take into account all follow-up.
At clinical cutoff (5 years), 87 (21%) of 417 patients had Patients in group A received trastuzumab and docetaxel; group B, pertuzumab, trastuzumab, and docetaxel;
progressed or died: 19 (18%) of 107 in group A, 17 (16%) group C, pertuzumab and trastuzumab; and group D, pertuzumab and docetaxel.
www.thelancet.com/oncology Vol 17 June 2016 795
Articles
survival results were consistent with progression-free had a progression-free survival event, compared with
survival results (figure 1B). 73 (23%) of 323 patients who did not achieve total
Exploratory subgroup analyses suggested an association pathological complete response (figure 2A). 5-year
between total pathological complete response and progression-free survival rates were 85% (95% CI 76–91)
progression-free survival when all treatment groups were for patients who achieved total pathological complete
combined (figure 2A). 94 (23%) of 417 patients achieved response, compared with 76% (95% CI 71–81) in patients
total pathological complete response. Of these, 14 (15%) who did not achieve total pathological complete response
(HR 0·54, 95% CI 0·29–1·00; figure 2A).
Results were consistent in each group (figure 2B) and
A
100
for hormone receptor-negative and hormone receptor-
positive disease (figure 2C).
90
Subgroup analyses of progression-free survival for
80
group B compared with group A were consistent with the
Progression-free survival (%)
70
findings in the overall population, although the small
60 number of events limits their interpretation (appendix
50 p 22).
40 Most patients (409 [98%] of 416) had at least one adverse
Number Number 5-year Hazard ratio
30 of of progression-free (95% CI)
event, of which 403 [97%] of 416 were deemed related to
20 patients events (%) survival (95% CI) study treatment. The most commonly reported adverse
10 tpCR 94 14 (15) 85% (76–91) events during the overall treatment period (neoadjuvant
0·54 (0·29–1·00)
No tpCR 323 73 (23) 76% (71–81) plus adjuvant periods) are shown in table 1 and are
0
0 12 24 36 48 60 generally consistent with those reported for the neoadjuvant
Months after randomisation period.2 The most common adverse events for the adjuvant
Number at risk
tpCR 94 91 83 79 76 55 period alone are provided in the appendix (p 12), as is a
No tpCR 323 287 262 244 234 178 detailed description of adverse events for the overall
treatment period (appendix pp 14–18). Adverse events
B
Events n (%) Hazard ratio (95% CI) grade 3 and worse that occurred during overall treatment
showed the expected chemotherapy toxicity profile (table 1).
Overall (n=417) 87 (21) 0·54 (0·29–1·00)
During adjuvant treatment, adverse events at grade 3 and
Group A (n=107) 19 (18) 0·67 (0·21–2·07)
worse were highest in group C, probably as a result of
Group B (n=107) 17 (16) 0·77 (0·23–2·56)
docetaxel followed by FEC administration (appendix p 12).
Group C (n=107) 27 (25) 0·26 (0·03–2·01)
Group D (n=96) 24 (25) 0·68 (0·19–2·41)
After adjuvant chemotherapy (ie, during single-agent
trastuzumab), the incidence of adverse events of grade 3
0·1 1 10·0 and worse was reduced to 7·8–10·6% across all groups,
tpCR better No tpCR better with none of these adverse events reported in more than
5% of patients. During post-treatment follow-up, adverse
C events were reported in few patients (seven [7%] of 107 in
100 group A, 11 [10%] of 107 in group B, eight [7%] of 108 in
90 group C, and seven [7%] of 94 in group D).
80 The incidence of serious adverse events during overall
Progression-free survival (%)
70 treatment was balanced across groups (table 1), but was
Number Number 5-year Hazard ratio
60 of of progression-free (95% CI)
slightly higher in group C during adjuvant treatment
50 patients events (%) survival (95% CI)
40 Hormone tpCR 72 12 (17) 84% (72–91) Figure 2: Exploratory subgroup analyses of progression-free survival
0·54 (0·28–1·06)
receptor- No tpCR 147 38 (26) 72% (64–79) according to tpCR
30 negative (A) Kaplan-Meier estimates of progression-free survival according to tpCR for all
20 Hormone tpCR 22 2 (9) 90% (67–98) treatment groups combined. The tick marks indicate the times at which events
0·54 (0·13–2·27) were recorded. The Kaplan-Meier curves are truncated at 60 months (the end of
10 receptor- No tpCR 175 34 (19) 80% (73–86)
positive scheduled follow-up). However, summary statistics shown here take into
0 account all follow-up. One late event occurred in the no total pathological
0 12 24 36 48 60 complete response group due to progressive disease at 71 months; one late
Months after randomisation event occurred in the tpCR group, a death due to an unrelated cerebrovascular
Number at risk
tpCR hormone 72 69 64 60 58 43 accident without progressive disease at 76 months. (B) Hazard ratios and
receptor-negative 95% CIs for progression-free survival according to tpCR for each individual
No tpCR hormone 147 125 108 102 97 82 group. (C) Kaplan-Meier estimates of progresssion-free survival according to
receptor-negative tpCR and hormone receptor status. One late event occurred in the tpCR
tpCR hormone 22 22 19 19 18 12 hormone receptor-negative group, a death due to an unrelated cerebrovascular
receptor-positive
accident without progressive disease at 76 months; two late events in the no
No tpCR hormone 175 161 153 142 137 96
receptor-positive
tpCR hormone receptor-positive group due to progressive disease at 63 and
71 months. tpCR=total pathological complete response.
796 www.thelancet.com/oncology Vol 17 June 2016
Articles
(appendix p 12). Neutropenia and febrile neutropenia
Trastuzumab Pertuzumab, Pertuzumab plus Pertuzumab
were reported most frequently. Two serious adverse plus docetaxel trastuzumab, trastuzumab plus docetaxel
events were reported during post-treatment follow-up: (group A; n=107) and docetaxel (group C; n=108) (group D; n=94)
myeloproliferative disorder and a cerebrovascular accident (group B; n=107)
resulting in death (considered unrelated to treatment). Any adverse event 107 (100%) 105 (98%) 103 (95%) 94 (100%)
31 deaths were reported during the study (appendix p 19). Alopecia 75 (70%) 73 (68%) 59 (55%) 65 (69%)
One death occurred during the neoadjuvant period Neutropenia 80 (75%) 68 (64%) 47 (44%) 69 (73%)
(fulminant hepatitis)2 and was considered possibly related Nausea 70 (65%) 71 (66%) 52 (48%) 61 (65%)
to study treatment; the remaining 30 occurred during Diarrhoea 41 (38%) 55 (51%) 46 (43%) 53 (56%)
follow-up and were assessed as either unrelated to study Fatigue 35 (33%) 35 (33%) 34 (31%) 37 (39%)
treatment or not known. 23 deaths were due to disease Vomiting 31 (29%) 39 (36%) 31 (29%) 37 (39%)
progression or breast cancer, two were due to colon or Mucosal inflammation 28 (26%) 33 (31%) 18 (17%) 29 (31%)
colorectal cancer, one due to cerebrovascular accident, and Rash 26 (24%) 30 (28%) 22 (20%) 30 (32%)
four had no cause reported. Myalgia 24 (22%) 25 (23%) 29 (27%) 22 (23%)
18 patients discontinued treatment because of study Asthenia 22 (21%) 29 (27%) 19 (18%) 23 (25%)
drug-related adverse events: no patients in group A, Any grade 3 or worse 87 (81%) 78 (73%) 65 (60%) 74 (79%)
five (5%) of 107 patients in group B (three from left adverse event
ventricular dysfunction, one from drug hypersensitivity, Neutropenia 71 (66%) 59 (55%) 40 (37%) 60 (64%)
and one from abdominal strangulated hernia), eight (7%) Febrile neutropenia 10 (9%) 12 (11%) 5 (5%) 15 (16%)
of 108 in group C (one from congestive cardiac failure, Leucopenia 13 (12%) 6 (6%) 4 (4%) 8 (9%)
three from drug hypersensitivity, one from asthenia, Menstruation irregular 6 (6%) 4 (4%) 7 (6%) 6 (6%)
one from chest discomfort, one from septic shock, and Diarrhoea 4 (4%) 7 (7%) 3 (3%) 5 (5%)
one due to pregnancy), and five (5%) of 94 in group D Granulocytopenia 1 (1%) 1 (1%) 5 (5%) 2 (2%)
(two from left ventricular dysfunction, one from biliary Vomiting 3 (3%) 0 1 (1%) 4 (4%)
cirrhosis, one from ulcerative colitis, and one from Asthenia 1 (1%) 2 (2%) 3 (3%) 3 (3%)
neutropenia). Urinary tract infection 2 (2%) 2 (2%) 1 (1%) 1 (1%)
Few patients (22 [5%] of 416) had cardiac events during Radiation skin injury 2 (2%) 2 (2%) 2 (2%) 0
the study (table 2). Aside from the previously reported Total number of serious 25 31 24 26
case of congestive heart failure in group C in the adverse events
neoadjuvant period (that resolved without sequelae Number of patients 21 (20%) 22 (21%) 19 (18%) 21 (22%)
following study treatment discontinuation and cardiac with one or more
drugs),2 only one other case of left ventricular serious adverse events
dysfunction of grade 3 or worse was reported (in group B Febrile neutropenia 10 (9%) 8 (7%) 4 (4%) 12 (13%)
during the adjuvant period; the patient was Neutropenia 1 (1%) 6 (6%) 3 (3%) 6 (6%)
asymptomatic). Asymptomatic left ventricular ejection Pyrexia 1 (1%) 1 (1%) 2 (2%) 1 (1%)
fraction declines of 10% or more from baseline to less Diarrhoea 2 (2%) 0 0 1 (1%)
than 50% were observed in 20 (5%) of 416 patients Left ventricular 0 3 (3%) 0 0
dysfunction
(some patients had events in more than one period;
Appendicitis 1 (1%) 0 1 (1%) 0
table 2). Most events occurred in the adjuvant period,
Neutropenic infection 1 (1%) 1 (1%) 1 (1%) 0
when patients were receiving trastuzumab. All patients
with asymptomatic cardiac events recovered to left Drug hypersensitivity 0 1 (1%) 1 (1%) 0
ventricular ejection fraction of 50% or more without Metrorrhagia 1 (1%) 0 1 (1%) 0
intervention, except for one patient with an Pyelonephritis, acute 0 2 (2%) 0 0
asymptomatic left ventricular dysfunction event in Wound infection 2 (2%) 0 0 0
group C, who developed this event during follow-up and Other 6 (6%) 9 (8%) 11 (10%) 6 (6%)
had not recovered at clinical cutoff. Death 0 1 (1%)* 0 0
Data are n (%). The ten most common adverse events, ten most common adverse events of grade 3 or worse, and
Discussion serious adverse events in two or more patients are reported. *Death in the neoadjuvant period from fulminant
In this 5-year follow-up of NeoSphere, the combination of hepatitis. Discrepancy with previously published data; one patient in group D withdrew from the study due to disease
progression in the neoadjuvant period, not due to death resulting from an adverse event as previously reported.2
neoadjuvant pertuzumab and trastuzumab plus docetaxel
(group B) seemed to improve long-term outcomes for Table 1: Most common adverse events, grade 3 or worse adverse events, and serious adverse events
patients compared with trastuzumab plus docetaxel during the overall treatment period (neoadjuvant and adjuvant)
(group A). Although these analyses are not powered for
formal statistical hypothesis testing and the results response in the breast. However, it is important to note
cannot claim statistical significance, the HR estimates for that the wide CIs allow for the possibility that group B is
progression-free survival and disease-free survival are not superior to group A. The combination of neoadjuvant
supportive of the primary results of pathological complete pertuzumab and docetaxel (group D) was associated
www.thelancet.com/oncology Vol 17 June 2016 797
Articles
In NeoSphere, all patients received the same
Trastuzumab Pertuzumab, Pertuzumab plus Pertuzumab
plus docetaxel trastuzumab, trastuzumab plus docetaxel chemotherapy drugs before and after surgery, with the
(group A; and docetaxel (group C; n=108) (group D; n=94) exception of patients in group C, who received all
n=107) (group B; chemotherapy after surgery. All patients received
n=107)
conventional adjuvant trastuzumab to complete 1 year
Neoadjuvant period n=107 n=107 n=108 n=94 of treatment. Improved disease-free survival after
Left ventricular dysfunction or 1 (1%) 3 (3%) 1 (1%) 1 (1%) four cycles of neoadjuvant pertuzumab and trastuzumab,
congestive heart failure
(any grade)
plus docetaxel (group B), might suggest a carry-over
Left ventricular dysfunction or 0 0 1 (1%)* 0
therapeutic effect that persisted after pertuzumab
congestive heart failure discontinuation and surgery, and that is unique to the
(grade 3 or worse) regimen of pertuzumab, trastuzumab, and docetaxel
LVEF decline to less than 50% 1 (1%) 3 (3%) 1 (1%) 1 (1%) because a similar effect was not observed in the other
and by 10% or more points treatment groups. The enhanced activity of the dual
from baseline
blockade of pertuzumab and trastuzumab might arise
Adjuvant period n=103 n=102 n=94 n=88
from complementary and different mechanisms of
Left ventricular dysfunction or 1 (1%) 5 (5%) 2 (2%) 5 (6%)
congestive heart failure
action of both antibodies, although the exact mechanism
(any grade) of action is currently unknown.
Left ventricular dysfunction or 0 1 (1%)† 0 0 Exploratory subgroup analyses were consistent with the
congestive heart failure overall results. Addition of pertuzumab to trastuzumab
(grade 3 or worse) and docetaxel improved progression-free survival
LVEF decline to less than 50% 1 (1%) 6 (6%) 0 5 (6%) irrespective of total pathological complete response and
and by 10% or more points
from baseline hormone receptor status. As expected, the magnitude of
Post-treatment follow-up period n=98 n=102 n=98 n=87 improvement was greater for patients with hormone
Left ventricular dysfunction or 0 3 (3%) 2 (2%) 2 (2%) receptor-negative disease, in line with the primary
congestive heart failure outcome results2 and the CTNeoBC meta-analysis.7
(any grade) FDA guidance13 states that a large improvement in
Left ventricular dysfunction or 0 0 0 0 pathological complete response is likely to predict
congestive heart failure
clinical benefit. Both the FDA and the EMA advise that
(grade 3 or worse)
approval based on pathological complete response
LVEF decline to less than 50% 0 3 (3%) 2 (2%) 2 (2%)
and by 10% or more points might be acceptable in the neoadjuvant setting under
from baseline specific circumstances.13,14 In NeoSphere, exploratory
Overall treatment and n=107 n=107 n=108 n=94 subgroup analyses found that, for all groups combined,
post-treatment follow-up patients who achieved total pathological complete
periods combined
response had improved progression-free survival.
Left ventricular dysfunction or 2 (2%) 9 (8%) 4 (4%)‡ 7 (7%)
congestive heart failure
Furthermore, this improvement was seen within each
(any grade) treatment group and occurred irrespective of hormone
Left ventricular dysfunction or 0 1 (1%)† 1 (1%)* 0 receptor status. However, these results must be
congestive heart failure interpreted with caution because there were few events
(grade 3 or worse) in each group, leading to large variability (wide CIs)
LVEF decline to less than 50% 2 (2%) 9 (8%) 2 (2%) 7 (7%) around the HR estimates. These results are consistent
and by 10% or more points
from baseline with the CTNeoBC meta-analysis,7 and with several
studies reporting an association between neoadjuvant
Data are n (%). Cardiac event codes to an adverse event of left ventricular dysfunction and congestive heart failure, or HER2 therapy and improved long-term outcomes,6,8–12
LVEF decline. Seven patients experienced LVEF declines in more than one treatment period. All patients who
experienced LVEF declines also had an adverse event of left ventricular dysfunction (asymptomatic) or congestive heart
including long-term analysis of the HannaH study18
failure reported during the study. LVEF=left ventricular ejection fraction. *Neoadjuvant period: congestive heart failure (neoadjuvant–adjuvant trastuzumab), in which total
grade 3, New York Heart Association class III. †Adjuvant period: reported as grade 3 but asymptomatic. ‡Post-treatment pathological complete response was associated
follow-up period: asymptomatic left ventricular dysfunction event which was ongoing at final analysis.
with improved event-free survival for both oestrogen
Table 2: Cardiac events for neoadjuvant, adjuvant, and post-treatment follow-up periods and for all receptor-positive and oestrogen receptor-negative or
periods combined unknown disease.
The results from these previous studies have led to the
with slightly worse long-term outcomes for patients expectation that positive results in the neoadjuvant
(24 progression-free survival events) compared with setting will be substantiated by large randomised
trastuzumab plus docetaxel (group A, 19 events) and adjuvant studies. However, this was apparently not
pertuzumab and trastuzumab plus docetaxel (group B, achieved in the tandem neoadjuvant NeoALTTO19 and
17 events). It is important to note that the statistical adjuvant ALTTO20 trials. Results from NeoALTTO19
comparison of group D with group A was not prespecified, showed a significant increase in pathological complete
and is therefore descriptive only. response with neoadjuvant lapatinib plus trastuzumab
798 www.thelancet.com/oncology Vol 17 June 2016
Articles
versus trastuzumab alone; however, results from 1·2
ALTTO20 did not support the benefit: there was no
significant improvement in disease-free survival with
Hazard ratio for event-free survival
1·0
the same treatment regimen in the adjuvant setting.
Of note, the trial designs were different and there were 0·8
substantial differences in the patient populations. 0·6
Furthermore, an analysis of the two trials using the Chemotherapy trials
FDA’s meta-analysis method7 found no discordance 0·4 HER2-directed therapy trials
between NeoALTTO and ALTTO and showed that the
results of ALTTO are supportive of the relationship 0·2
between pathological complete response and event-free
0
survival.21 0 0·4 0·8 1·2 1·6 2·0 2·4 2·8 3·2 3·6
An illustration of the power of the neoadjuvant Odds ratio for pathological complete response
approach in estimating the benefit of new therapies
GeparTrio: DAC 6 cycles vs DAC 4 cycles in responders
might be derived from the relationship between the GeparQuattro: EC→docetaxel+capecitabine vs EC→docetaxel
odds ratio for pathological complete response of NOAH: neoadjuvant trastuzumab→chemotherapy→ adjuvant trastuzumab vs chemotherapy
NeoALTTO: lapatinib vs trastuzumab
different treatments and the HR for event-free survival, GeparTrio: vinorelbine+capecitabine 4 cycles vs DAC 4 cycles in non-responders
as originally proposed in the CTNeoBC meta-analysis.7 GeparQuattro: EC→docetaxel then capecitabine vs EC→docetaxel
NeoALTTO: lapatinib+trastuzumab vs trastuzumab
Results from various trials—including GeparTrio, NeoSphere: trastuzumab+pertuzumab+chemotherapy vs trastuzumab+chemotherapy
GeparQuattro, NOAH (Cortazar P, Genentech, personal
communication), NeoALTTO,8,19 and NeoSphere, which Figure 3: Association between the effect of chemotherapy and chemotherapy plus HER2-directed therapies
reported proportions of patients with pathological on pathological complete response and event-free survival
Data derived from CTNeoBC (Cortazar P, Genentech, personal communication) and from NeoALTTO.8,19 The sizes of
complete response and event-free survival—showed that the circles are proportional to the analysed population sizes. DAC=docetaxel, doxorubicin, and cyclophosphamide.
the odds ratio for pathological complete response might EC=epirubicin and cyclophosphamide.
be associated with the HR for event-free survival
(r²=0·25; figure 3). This potential association becomes during the neoadjuvant period did not seem to result in
more pronounced when considering only trials that any additional or long-term cardiotoxicity.
included HER2-targeted therapies (r²=0·77) and In summary, the long-term results of NeoSphere are
excluding the cluster of empirical chemotherapy trials. encouraging. Although for descriptive purposes only, they
Thus, a thorough comparison of pathological complete support the primary analysis of pathological complete
response in the appropriate setting would be informative response in the breast and suggest that four cycles of
and might validate pathological complete response as a neoadjuvant pertuzumab is also beneficial in terms of
surrogate marker of efficacy. long-term efficacy, when combined with trastuzumab and
Although achievement of total pathological complete docetaxel, despite the use of identical adjuvant therapy.
response was associated with improved long-term The neoadjuvant safety profile was maintained with
outcomes, most patients (77%) in NeoSphere did not long-term follow-up. The ongoing phase 3 APHINITY
achieve total pathological complete response. However, trial (NCT01358877) will assess pertuzumab, in com-
residual disease is not necessarily a marker of failure of bination with trastuzumab and chemotherapy, in the
any neoadjuvant treatment. The 9-year analysis of the adjuvant setting. Overall, the results of NeoSphere provide
National Surgical Adjuvant Breast and Bowel Project22 new insight into the association between total pathological
Protocol B-18 showed that clinical response (complete or complete response and long-term outcomes and support
partial response) correlated with long-term outcomes. the use of total pathological complete response as a
It is therefore important to note that patients who did not primary endpoint and early indicator of benefit in future
achieve total pathological complete response but received neoadjuvant studies of HER2-targeted agents.13,23
pertuzumab seemed to have longer progression-free Contributors
survival than those who did not achieve total pathological LG was involved in study design, protocol development, recruitment and
complete response and did not receive pertuzumab management of patients, data collection, analysis, and interpretation,
and writing of the report. PV was involved in study design, protocol
(appendix p 22). The data suggest that pathological development, data analysis and interpretation, and writing of the report.
complete response is a non-exclusive measure of efficacy GR was involved in study design, protocol development, data analysis
of neoadjuvant therapy, and it is not the only measure of and interpretation, and writing of the report. VM was involved in
benefit of pertuzumab. protocol development, review and management of clinical data, data
analysis and interpretation, and writing of the report. HD was involved
There were no new or long-term safety concerns with in data collection, figure generation, data analysis and interpretation,
5 years of follow-up. The overall tolerability profile was and writing of the report. DM was involved in data analysis and
similar across treatment groups and was consistent with interpretation and writing of the report. TP, Y-HI, L-MT, M-CL, AL, ES,
that previously reported for the neoadjuvant period2 and JdlH-R, S-AI, JLP, BP, PM, VSe, VSr, and GVB were involved in the
discussion of the protocol, recruitment and management of patients,
similar to that observed in TRYPHAENA.3 Importantly, and data collection and interpretation. All authors reviewed and
the addition of pertuzumab to trastuzumab and docetaxel approved the manuscript for submission.
www.thelancet.com/oncology Vol 17 June 2016 799
Articles
Declaration of interests 10 von Minckwitz G, Rezai M, Fasching PA, et al. Survival after
LG is an advisory board member for Roche, Genentech, Tahio, Novartis, adding capecitabine and trastuzumab to neoadjuvant
Synthon, Pfizer, Tiziana Life Sciences, Genomic Health, Medivation, anthracycline-taxane-based chemotherapy for primary breast
Boehringer Ingelheim, and Celegene. VM is a current employee of Roche, cancer (GBG 40--GeparQuattro). Ann Oncol 2014; 25: 81–89.
and reports Roche stock ownership interests. HD is a current employee of 11 Gonzalez-Angulo AM, Parinyanitikul N, Lei X, et al. Effect of
Roche. GR was a full-time employee of Roche during the design and adjuvant trastuzumab among patients treated with anti-HER2-based
conduct of NeoSphere. TP reports grants and personal fees from Roche. neoadjuvant therapy. Br J Cancer 2015; 112: 630–35.
S-AI reports grants from AstraZeneca. AL reports personal fees from 12 Loibl S, von Minckwitz G, Blohmer JU, et al. pCR as a surrogate in
Novartis, Roche, and Pfizer. PV reports grant from Roche. Y-HI, L-MT, HER2-positive patients treated with trastuzumab. Cancer Res 2011;
71: S5-4 (abstr).
M-CL, ES, JdlH-R, JLP, BP, PM, VSe, GVB, VSr, and DM declare no
13 US Food and Drug Administration (FDA). Guidance for Industry.
competing interests.
Pathological Complete Response in Neoadjuvant Treatment of
Acknowledgments High-Risk Early-Stage Breast Cancer: Use as an Endpoint to
This was a collaborative study between Fondazione Michelangelo and Support Accelerated Approval. Draft Guidance. http://www.fda.gov/
F Hoffmann-La Roche. Support for third-party writing assistance for this downloads/drugs/guidancecomplianceregulatoryinformation/
manuscript, furnished by Debbie Briggs, was provided by guidances/ucm305501.pdf (accessed Jan 28, 2016).
F Hoffmann-La Roche. A full list of NeoSphere investigators is provided 14 European Medicines Agency (EMA) & Committee for Medicinal
in the appendix. We thank all patients and investigators who participated Products for Human Use (CHMP). Appendix 4 to the guideline on
the evaluation of anticancer medicinal products in man. EMA/
in this trial and also the central testing laboratories: Targos Molecular
CHMP/703715/2012 Revised July 1, 2015. http://www.ema.europa.
Pathology GmbH, Kassel, Germany, and Roche TRS DNS and protein
eu/docs/en_GB/document_library/Scientific_guideline/2015/10/
laboratories, Basel, Switzerland. WC500195215.pdf (accessed Jan 28, 2016).
References 15 Cancer Therapy Evaluation Program (CTEP). Common Terminology
1 Baselga J, Gelmon KA, Verma S, et al. Phase II trial of pertuzumab Criteria for Adverse Events (CTCAE), Version 3.0. DCTD, NCI, NIH,
and trastuzumab in patients with human epidermal growth factor DHHS. http://ctep.cancer.gov/protocolDevelopment/electronic_
receptor 2-positive metastatic breast cancer that progressed during applications/docs/ctcaev3.pdf (accessed Jan 28, 2016).
prior trastuzumab therapy. J Clin Oncol 2010; 28: 1138–44. 16 The Criteria Committee for the New York Heart Association.
2 Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of Nomenclature and Criteria for Diagnosis of Diseases of the Heart
neoadjuvant pertuzumab and trastuzumab in women with locally and Great Vessels. 9th edn. In: Dolgin M, ed. Boston, MA, USA:
advanced, inflammatory, or early HER2-positive breast cancer Little, Brown and Company, 1994: 253–55.
(NeoSphere): a randomised multicentre, open-label, phase 2 trial. 17 Bianchi G, Albanell J, Eiermann W, et al. Pilot trial of trastuzumab
Lancet Oncol 2012; 13: 25–32. starting with or after the doxorubicin component of a doxorubicin
3 Schneeweiss A, Chia S, Hickish T, et al. Pertuzumab plus plus paclitaxel regimen for women with HER2-positive advanced
trastuzumab in combination with standard neoadjuvant breast cancer. Clin Cancer Res 2003; 9 (16 Pt 1): 5944–51.
anthracycline-containing and anthracycline-free chemotherapy 18 Jackisch C, Hegg R, Stroyakovskiy D, et al. Total pathologic
regimens in patients with HER2-positive early breast cancer: complete response (tpCR) and event-free survival (EFS) with
a randomized phase II cardiac safety study (TRYPHAENA). subcutaneous (SC) or intravenous (IV) trastuzumab in
Ann Oncol 2013; 24: 2278–84. HER2-positive early breast cancer (EBC): The HannaH Phase III
4 Baselga J, Cortés J, Kim SB, et al. Pertuzumab plus trastuzumab plus study. J Clin Oncol 2015; 13 (suppl): 585 (abstr).
docetaxel for metastatic breast cancer. N Engl J Med 2012; 366: 109–19. 19 Baselga J, Bradbury I, Eidtmann H, et al. Lapatinib with
5 Swain SM, Baselga J, Kim SB, et al. Pertuzumab, trastuzumab, and trastuzumab for HER2-positive early breast cancer (NeoALTTO):
docetaxel in HER2-positive metastatic breast cancer. N Engl J Med a randomised, open-label, multicentre, phase 3 trial. Lancet 2012;
2015; 372: 724–34. 379: 633–40.
6 Untch M, Fasching PA, Konecny GE, et al. Pathologic complete 20 Piccart-Gebhart MJ, Holmes AP, Baselga J, et al. First results from
response after neoadjuvant chemotherapy plus trastuzumab predicts the phase III ALTTO trial (BIG 2-06; NCCTG [Alliance] N063D)
favorable survival in human epidermal growth factor receptor comparing one year of anti-HER2 therapy with lapatinib alone (L),
2-overexpressing breast cancer: results from the TECHNO trial of trastuzumab alone (T), their sequence (T->L), or their combination
the AGO and GBG study groups. J Clin Oncol 2011; 29: 3351–57. (T+L) in the adjuvant treatment of HER2-positive early breast
7 Cortazar P, Zhang L, Untch M, et al. Pathological complete cancer (EBC). J Clin Oncol 2014; 32: LBA4 (abstr).
response and long-term clinical benefit in breast cancer: 21 DeMichele A, Yee D, Berry DA, et al. The neoadjuvant model is still
the CTNeoBC pooled analysis. Lancet 2014; 384: 164–72. the future for drug development in breast cancer. Clin Cancer Res
8 de Azambuja E, Holmes AP, Piccart-Gebhart M, et al. 2015; 21: 2911–15.
Lapatinib with trastuzumab for HER2-positive early breast cancer 22 Wolmark N, Wang J, Mamounas E, Bryant J, Fisher B. Preoperative
(NeoALTTO): survival outcomes of a randomised, open-label, chemotherapy in patients with operable breast cancer: nine-year
multicentre, phase 3 trial and their association with pathological results from National Surgical Adjuvant Breast and Bowel Project
complete response. Lancet Oncol 2014; 15: 1137–46. B-18. J Natl Cancer Inst Monogr 2001; 30: 96–102.
9 Gianni L, Eiermann W, Semiglazov V, et al. Neoadjuvant and 23 Prowell TM, Pazdur R. Pathological complete response and
adjuvant trastuzumab in patients with HER2-positive locally accelerated drug approval in early breast cancer. N Engl J Med 2012;
advanced breast cancer (NOAH): follow-up of a randomised 366: 2438–41.
controlled superiority trial with a parallel HER2-negative cohort.
Lancet Oncol 2014; 15: 640–47.
800 www.thelancet.com/oncology Vol 17 June 2016
You might also like
- Pathophysiology - CholedocholithiasisDocument1 pagePathophysiology - CholedocholithiasisMark OrculloNo ratings yet
- Rubi Li v. Sps. SolimanDocument1 pageRubi Li v. Sps. SolimanJennifer OceñaNo ratings yet
- cs2 NCPDocument1 pagecs2 NCPapi-251084195No ratings yet
- Lancet 2021 Mesoth PleuralDocument12 pagesLancet 2021 Mesoth PleuralJeanne LahogueNo ratings yet
- PIIS014067361261900XDocument10 pagesPIIS014067361261900X呂鍇東No ratings yet
- Swain 2020Document12 pagesSwain 2020NicolásPGNo ratings yet
- Lancet Oncol 2013 VermorkenDocument14 pagesLancet Oncol 2013 Vermorkens007972No ratings yet
- Aparicio 2011Document5 pagesAparicio 2011Bruno AlanNo ratings yet
- Annonc mdw587.026Document1 pageAnnonc mdw587.026Aaron Paul BernasNo ratings yet
- CTP6 Biosimilar Trastuzumab Lancet Oncol 2017Document12 pagesCTP6 Biosimilar Trastuzumab Lancet Oncol 2017AS Ngọc ÁnhNo ratings yet
- Recurrent Glioblastoma Treated With Recombinant Poliovirus: Original ArticleDocument12 pagesRecurrent Glioblastoma Treated With Recombinant Poliovirus: Original ArticleTrinanda ChoirunissaNo ratings yet
- 38 Pertuzumab UslessDocument13 pages38 Pertuzumab Uslessbawoji1763No ratings yet
- CheckMate 238Document12 pagesCheckMate 238PeyepeyeNo ratings yet
- Sciencedirect: Original ResearchDocument10 pagesSciencedirect: Original ResearchchubyXDNo ratings yet
- Abdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceDocument8 pagesAbdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceWitrisyah PutriNo ratings yet
- Inotozumab OzogamicinDocument14 pagesInotozumab OzogamicinTaraNo ratings yet
- Keynote 054Document12 pagesKeynote 054PeyepeyeNo ratings yet
- Elective Versus Therapeutic Neck Dissection in Node-Negative Oral Cancer PDFDocument9 pagesElective Versus Therapeutic Neck Dissection in Node-Negative Oral Cancer PDFluxmansrikanthaNo ratings yet
- 1 s2.0 S0140673623020330 Main 2Document12 pages1 s2.0 S0140673623020330 Main 2Uriel EnriquezNo ratings yet
- 9Document13 pages9Osama BakheetNo ratings yet
- Nej Mo A 1905287Document12 pagesNej Mo A 1905287Ari KurniawanNo ratings yet
- Tumour-Agnostic Efficacy and Safety of Selpercatinib in Patients With RET Fusion-Positive Solid Tumours Other Than Lung or Thyroid Tumours (LIBRETTO-001)Document13 pagesTumour-Agnostic Efficacy and Safety of Selpercatinib in Patients With RET Fusion-Positive Solid Tumours Other Than Lung or Thyroid Tumours (LIBRETTO-001)Milan JovicNo ratings yet
- DTG VS RTGDocument9 pagesDTG VS RTGThanawan TippayamongkolkulNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: BackgroundDita Putri DamayantiNo ratings yet
- Kim 2015Document9 pagesKim 2015Ke XuNo ratings yet
- Jurnal Anestesi "RCT"Document9 pagesJurnal Anestesi "RCT"Feri AprizalNo ratings yet
- Articles: BackgroundDocument9 pagesArticles: Background111No ratings yet
- Articles: BackgroundDocument11 pagesArticles: BackgroundOncología CdsNo ratings yet
- Goal-Directed Resuscitation For Patients With Early Septic ShockDocument11 pagesGoal-Directed Resuscitation For Patients With Early Septic ShockArariwaMoralesNo ratings yet
- Nejmoa 2032125Document13 pagesNejmoa 2032125CARLOS DURANNo ratings yet
- Jo Howard Long TermDocument11 pagesJo Howard Long TermKuliah Semester 4No ratings yet
- TraztuzumabDocument8 pagesTraztuzumabArlina Wiyata GamaNo ratings yet
- He 2021 Icotinib Versus Chemotherapy As Adjuvant Treatment For Stage II-IIIA EGFR-mutant Non-Small-Cell Lung Cancer (EVIDENCE) A Randomised, Open-Label, Phase 3 TrialDocument9 pagesHe 2021 Icotinib Versus Chemotherapy As Adjuvant Treatment For Stage II-IIIA EGFR-mutant Non-Small-Cell Lung Cancer (EVIDENCE) A Randomised, Open-Label, Phase 3 TriallutfiaNo ratings yet
- Is It Safe To Discharge Intussusception Patients After Successful Hydrostatic Reduction?Document5 pagesIs It Safe To Discharge Intussusception Patients After Successful Hydrostatic Reduction?DaGiTrVel'zNo ratings yet
- Provenge 2Document12 pagesProvenge 2api-675909478No ratings yet
- Abdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceDocument8 pagesAbdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceWitrisyah PutriNo ratings yet
- Impact of Time From Completion of Neoadjuvant Chemotherapy To Surgery On Survival Outcomes in Breast Cancer PatientsDocument7 pagesImpact of Time From Completion of Neoadjuvant Chemotherapy To Surgery On Survival Outcomes in Breast Cancer PatientsPani lookyeeNo ratings yet
- Chemo & Radio in NPC - MAC NPC UpdateDocument11 pagesChemo & Radio in NPC - MAC NPC UpdatezanNo ratings yet
- Pazopanib Tumor Fibroso SolitarioDocument11 pagesPazopanib Tumor Fibroso SolitariocarolinapolotorresNo ratings yet
- Ceftaroline Vs Ceftriaxone in Asian PatientsDocument11 pagesCeftaroline Vs Ceftriaxone in Asian PatientsJohn MolinaNo ratings yet
- UveitisDocument10 pagesUveitisUtomo FemtomNo ratings yet
- Sciencedirect: Original ResearchDocument9 pagesSciencedirect: Original Researchfaris nagibNo ratings yet
- Nejmoa 1112088Document11 pagesNejmoa 1112088Med MedNo ratings yet
- Trastuzumab Deruxtecan (DS-8201a) in Patients With Advanced HER2-positive Gastric Cancer: A Dose-Expansion, Phase 1 StudyDocument10 pagesTrastuzumab Deruxtecan (DS-8201a) in Patients With Advanced HER2-positive Gastric Cancer: A Dose-Expansion, Phase 1 Studybawoji1763No ratings yet
- Ou 2016Document8 pagesOu 2016tami widiatul azahraNo ratings yet
- CrizotinibDocument10 pagesCrizotinibLuca StamerraNo ratings yet
- Tofacitinib As Induction and Maintenance Therapy For Ulcerative ColitisDocument14 pagesTofacitinib As Induction and Maintenance Therapy For Ulcerative Colitismichal ben meronNo ratings yet
- Nej Mo A 1113216Document11 pagesNej Mo A 1113216daypranitaNo ratings yet
- Sun 2016Document12 pagesSun 2016trifamonika23No ratings yet
- Intravenous Tenecteplase Compared With Alteplase For Acute IschaemicDocument9 pagesIntravenous Tenecteplase Compared With Alteplase For Acute IschaemicVictoria JacoboNo ratings yet
- Nej Mo A 0908806Document11 pagesNej Mo A 0908806dimazerrorNo ratings yet
- Surgical Outcome Results From SWOG S1505: Asa PDocument6 pagesSurgical Outcome Results From SWOG S1505: Asa PElianaNo ratings yet
- 2003-Academic Emergency MedicineDocument154 pages2003-Academic Emergency MedicinealiceNo ratings yet
- Schöffski Et Al. - 2016 - Eribulin Versus Dacarbazine in Previously TreatedDocument9 pagesSchöffski Et Al. - 2016 - Eribulin Versus Dacarbazine in Previously TreatedM.No ratings yet
- Me Hanna 2016Document11 pagesMe Hanna 2016eswarNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofJoão AugustoNo ratings yet
- Jon Ker 2018Document8 pagesJon Ker 2018WilliamYañezRojasNo ratings yet
- Genética Clínica 2Document10 pagesGenética Clínica 2Victor MarquesNo ratings yet
- Eddy 2007Document8 pagesEddy 2007Mimsy Quiñones TafurNo ratings yet
- Jgo 29 E76Document12 pagesJgo 29 E76hanifigaNo ratings yet
- Kemoterapi THT 5Document8 pagesKemoterapi THT 5Niko Nofian NugrohoNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Ranibizumab Lucentis Versus Bevacizumab Avastin For The Treatment of Age Related Macular Degeneration An Economic Disparity of Eye HealthDocument8 pagesRanibizumab Lucentis Versus Bevacizumab Avastin For The Treatment of Age Related Macular Degeneration An Economic Disparity of Eye HealthmaleticjNo ratings yet
- Compound Options Numerical Valuation MethodsDocument47 pagesCompound Options Numerical Valuation MethodsmaleticjNo ratings yet
- Updates On The Epidemiology of Age Related Macular.5Document5 pagesUpdates On The Epidemiology of Age Related Macular.5maleticjNo ratings yet
- Persistance Amound DMARDSDocument8 pagesPersistance Amound DMARDSmaleticjNo ratings yet
- Compliance To FingolimodDocument9 pagesCompliance To FingolimodmaleticjNo ratings yet
- MIT Machine Learning Trial OutcomesDocument71 pagesMIT Machine Learning Trial OutcomesmaleticjNo ratings yet
- Real World Experiences Pirfenidone and Nintedanib Are Effective and Well Tolerated Treatments For Idiopathic Pulmonary FibrosisDocument12 pagesReal World Experiences Pirfenidone and Nintedanib Are Effective and Well Tolerated Treatments For Idiopathic Pulmonary FibrosismaleticjNo ratings yet
- Pirfenidone and Nintedanib Compliance and Persistence in A Real World SettingDocument2 pagesPirfenidone and Nintedanib Compliance and Persistence in A Real World SettingmaleticjNo ratings yet
- Measuring The Return From Pharmaceutical Innovation 2020 - Deloitte - Life Sciences and HealthcareDocument3 pagesMeasuring The Return From Pharmaceutical Innovation 2020 - Deloitte - Life Sciences and HealthcaremaleticjNo ratings yet
- An Investigation of The False Discovery Rate and The Misinterpretation of P-ValuesDocument16 pagesAn Investigation of The False Discovery Rate and The Misinterpretation of P-ValuesmaleticjNo ratings yet
- Commercializing Biomedical Research Through SecuriDocument12 pagesCommercializing Biomedical Research Through SecurimaleticjNo ratings yet
- Convicted On Statistics - Understanding UncertaintyDocument9 pagesConvicted On Statistics - Understanding UncertaintymaleticjNo ratings yet
- How To Understand Degrees of FreedomDocument8 pagesHow To Understand Degrees of FreedommaleticjNo ratings yet
- Combinatorial Treatment For Spinal Muscular AtrophyDocument4 pagesCombinatorial Treatment For Spinal Muscular AtrophymaleticjNo ratings yet
- A. Nursing Practice: Introduction To PharmacologyDocument2 pagesA. Nursing Practice: Introduction To Pharmacologyyssa deliNo ratings yet
- Name Generic Class of Drug Patient'S Dose and Route Usual Dose Recommended Target Symptoms Drug Is Intended To Address Top 3-5 Nursing ImplicationsDocument3 pagesName Generic Class of Drug Patient'S Dose and Route Usual Dose Recommended Target Symptoms Drug Is Intended To Address Top 3-5 Nursing ImplicationsJay VillasotoNo ratings yet
- Introduction To CVSDocument3 pagesIntroduction To CVSapi-3829364No ratings yet
- Liver CirrhosisDocument42 pagesLiver CirrhosisMariejoy YadaoNo ratings yet
- CDF SPC All LOB Except HL LevelDocument2 pagesCDF SPC All LOB Except HL LevelSRIKANTA ROUTNo ratings yet
- MCQ in General Surgery For UndergraduatesDocument259 pagesMCQ in General Surgery For UndergraduatesBadri Kobalava100% (5)
- Fracture Colles Rehabilitation Advice Following WristDocument4 pagesFracture Colles Rehabilitation Advice Following WristfaprilisaNo ratings yet
- A Glimpse Into How Greg Roskopf Developed MATDocument20 pagesA Glimpse Into How Greg Roskopf Developed MATrobertobarron100% (2)
- ICU AlgorithmsDocument45 pagesICU AlgorithmsHashimIdreesNo ratings yet
- Sarah Dyaanggari Akip 22010111140188 Lap - Kti Bab ViiiDocument26 pagesSarah Dyaanggari Akip 22010111140188 Lap - Kti Bab ViiiHaikal FauzieNo ratings yet
- BenzodiazepinesDocument7 pagesBenzodiazepinesRully B ChristinaNo ratings yet
- Final Quality Assurance ProgramDocument4 pagesFinal Quality Assurance ProgramGanie Mar BiasonNo ratings yet
- Classification of Handicapped ConditionsDocument23 pagesClassification of Handicapped ConditionsVaishakhi BaisaneNo ratings yet
- Rationalization of AWC Wcdpo SiwanDocument17 pagesRationalization of AWC Wcdpo SiwanAK ContinentalNo ratings yet
- CONTINGENCY PLAN For Limited Face To FaceDocument15 pagesCONTINGENCY PLAN For Limited Face To FaceMaricar Dimas100% (3)
- Catch Up FridayDocument4 pagesCatch Up FridayMa. Phoebe AlleoNo ratings yet
- Benign and Malignant Tumors of Oral CavityDocument56 pagesBenign and Malignant Tumors of Oral CavityPawan Kumar83% (6)
- Anesthesiology Quick Reference (Adult) : Intubating MaintenanceDocument2 pagesAnesthesiology Quick Reference (Adult) : Intubating Maintenanceanestesi unpadNo ratings yet
- Style Guide - NCDJDocument11 pagesStyle Guide - NCDJVaishnavi JayakumarNo ratings yet
- Comminuted Patella Fracture in Elderly Patients - A Systematic Review and Case ReportDocument10 pagesComminuted Patella Fracture in Elderly Patients - A Systematic Review and Case ReportAldrovando JrNo ratings yet
- 77.18 Shen Guan and Three Emperors - Master Kidney PointDocument3 pages77.18 Shen Guan and Three Emperors - Master Kidney Pointalbar ismuNo ratings yet
- The Effectiveness of Pre-Operative Deep BreathingDocument5 pagesThe Effectiveness of Pre-Operative Deep BreathingJulenda CintarinovaNo ratings yet
- Maternal and Early-Life Nutrition and HealthDocument4 pagesMaternal and Early-Life Nutrition and HealthTiffani_Vanessa01No ratings yet
- Stroke (Bisaya and English)Document4 pagesStroke (Bisaya and English)AnaNo ratings yet
- Treatment ModalitiesDocument5 pagesTreatment ModalitiesMichelleIragAlmarioNo ratings yet
- Injury and Overuse Injury.: Classification of Sports InjuriesDocument2 pagesInjury and Overuse Injury.: Classification of Sports InjuriesVladGrosuNo ratings yet
- NCP Nursing Care Plans For Aplastic AnemiaDocument3 pagesNCP Nursing Care Plans For Aplastic AnemiaTahir Ali0% (1)