Download as pdf or txt
You might also like
- Ways of Enhancing Pulp Preservation by Stepwise Excavation-A Systematic Review PDFDocument13 pagesWays of Enhancing Pulp Preservation by Stepwise Excavation-A Systematic Review PDFFabian ArangoNo ratings yet
- Caesars Sportsbook Prop Betting Menu - Super Bowl LVII - FinalDocument22 pagesCaesars Sportsbook Prop Betting Menu - Super Bowl LVII - FinalTony Garcia100% (1)
- The Biomimetic Concept (8 Online Lessons)Document14 pagesThe Biomimetic Concept (8 Online Lessons)Francesca MocanuNo ratings yet
- Manufacturing Process of SemiconductorDocument36 pagesManufacturing Process of SemiconductorMayank Agarwal100% (1)
- 2017 Article 178Document6 pages2017 Article 178Alaa Yasser AlautiNo ratings yet
- Comparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionDocument4 pagesComparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionShahrukh ali khanNo ratings yet
- Effectiveness of Different Denture Cleansing Methods On Removal of Biofilms Formed in VivoDocument6 pagesEffectiveness of Different Denture Cleansing Methods On Removal of Biofilms Formed in VivodanielNo ratings yet
- Adhesive Performance of A Multi-Mode Adhesive System - 1-Year in Vitro Study Lorenzo Breschi DDocument10 pagesAdhesive Performance of A Multi-Mode Adhesive System - 1-Year in Vitro Study Lorenzo Breschi DEliseu LucenaNo ratings yet
- Efficacy and Safety of Two Treatment Protocols For Dental FluorosisDocument7 pagesEfficacy and Safety of Two Treatment Protocols For Dental Fluorosissmile4DrNo ratings yet
- Journal of Prosthodontic Research: Yuya Baba, Yusuke Sato, Gaku Owada, Shunsuke MinakuchiDocument6 pagesJournal of Prosthodontic Research: Yuya Baba, Yusuke Sato, Gaku Owada, Shunsuke MinakuchiSayed RustiaNo ratings yet
- UA Gabriela Canali2018Document9 pagesUA Gabriela Canali2018selvaortho94No ratings yet
- Development of A Method in Situ To Study Toothpaste Abrasion of DentineDocument5 pagesDevelopment of A Method in Situ To Study Toothpaste Abrasion of DentineLuisaa DeCanela'No ratings yet
- (CarisolvTM) Efect Antimicrob.2008Document7 pages(CarisolvTM) Efect Antimicrob.2008Șenchea Crina ElenaNo ratings yet
- Sealing Effectiveness of Fissure Sealant Bonded With Universal Adhesive SystemsDocument6 pagesSealing Effectiveness of Fissure Sealant Bonded With Universal Adhesive SystemsJoseph EneroNo ratings yet
- Angle Orthod. 2020 90 1 100-108Document9 pagesAngle Orthod. 2020 90 1 100-108brookortontiaNo ratings yet
- Denture Cleansers: A ReviewDocument3 pagesDenture Cleansers: A ReviewInternational Organization of Scientific Research (IOSR)No ratings yet
- Tunaru Biodentine PDFDocument7 pagesTunaru Biodentine PDFBianca IovoaiaNo ratings yet
- Caries-Preventive Effect of Sealants Produced With Altered Glass-Ionomer Materials, After 2 YearsDocument7 pagesCaries-Preventive Effect of Sealants Produced With Altered Glass-Ionomer Materials, After 2 Yearsandres castroNo ratings yet
- Assessment of Clinical Success of Three Sealants: Embrace-Wetbond, Clinpro, and Helioseal-F in Permanent Molars: An in Vivo StudyDocument7 pagesAssessment of Clinical Success of Three Sealants: Embrace-Wetbond, Clinpro, and Helioseal-F in Permanent Molars: An in Vivo StudyABNo ratings yet
- 2010 - Amanda - Peracini - Effect Ofdenturecleansers On Physical Properties of Heat (Retrieved-2017!03!14)Document6 pages2010 - Amanda - Peracini - Effect Ofdenturecleansers On Physical Properties of Heat (Retrieved-2017!03!14)drmezzo68No ratings yet
- Resultados Do Tratamento de Canal de Dentes Necróticos Com Periodontite Apical Preenchidos Com Selante À Base de BiocerâmicaDocument8 pagesResultados Do Tratamento de Canal de Dentes Necróticos Com Periodontite Apical Preenchidos Com Selante À Base de BiocerâmicadranayhaneoliveiraNo ratings yet
- Articulo Sellante InvasivoDocument7 pagesArticulo Sellante InvasivoJeannette BorreroNo ratings yet
- Kumar2017Document6 pagesKumar2017Andre KusoemoNo ratings yet
- Gingival: Waxed and Unwaxed Dental Floss HealthDocument4 pagesGingival: Waxed and Unwaxed Dental Floss HealthNujood AwadNo ratings yet
- 66-Blinded Manuscript-66-1-10-20151003Document8 pages66-Blinded Manuscript-66-1-10-20151003ajengwidyapyahoo.comNo ratings yet
- Gingival Margin Stability After Mucogingival Plastic Surgery. The Effect of Manual Versus Powered Toothbrushing: A Randomized Clinical TrialDocument13 pagesGingival Margin Stability After Mucogingival Plastic Surgery. The Effect of Manual Versus Powered Toothbrushing: A Randomized Clinical TrialMarco Antonio García LunaNo ratings yet
- TSWJ2023 9920850Document9 pagesTSWJ2023 9920850birkekocaunsalNo ratings yet
- Evaluation of The Efficacy of Mineral Trioxide Aggregate and Bioceramic PuttyDocument7 pagesEvaluation of The Efficacy of Mineral Trioxide Aggregate and Bioceramic PuttyMarta Torrubiano PérezNo ratings yet
- Effect of Sodium Hypochlorite and Ricinus Communis Solutions On Control of Denture Biofilm: A Randomized Crossover Clinical TrialDocument6 pagesEffect of Sodium Hypochlorite and Ricinus Communis Solutions On Control of Denture Biofilm: A Randomized Crossover Clinical TrialHelena VenanteNo ratings yet
- A Histopathologic Study On Pulp Response To Glass Ionomer Cements in Human TeethDocument8 pagesA Histopathologic Study On Pulp Response To Glass Ionomer Cements in Human Teethnahm17No ratings yet
- Effect of Etching The Coronal Dentin With The RubbDocument6 pagesEffect of Etching The Coronal Dentin With The Rubbmaroun ghalebNo ratings yet
- Nano Biofusion GelDocument8 pagesNano Biofusion GelChandra SekharNo ratings yet
- 1852-4834-Aol-33-3-174 FINAL DR HARRYDocument7 pages1852-4834-Aol-33-3-174 FINAL DR HARRYMarco Antonio García LunaNo ratings yet
- Jurnal 2 - IKGADocument6 pagesJurnal 2 - IKGANovita BerlianaNo ratings yet
- Smear LayerDocument14 pagesSmear Layersandra del pilarNo ratings yet
- Int J Dental Hygiene - 2021 - MensiDocument10 pagesInt J Dental Hygiene - 2021 - MensiMARTÍN EMILIO BENAVENTENo ratings yet
- Antimicrobial Effect of Endodontic Solutions Used As Final Irrigants On A Dentine Biofilm ModelDocument7 pagesAntimicrobial Effect of Endodontic Solutions Used As Final Irrigants On A Dentine Biofilm ModelHarini VenkatNo ratings yet
- Comparative Effect of Neemstick and Toothbrush On Plaque Removal and Gingival Health - A Clinical TrialDocument6 pagesComparative Effect of Neemstick and Toothbrush On Plaque Removal and Gingival Health - A Clinical TrialnavinlewisNo ratings yet
- Jurnal 2. Alkaline Peroxides Versus Sodium Hypochlorite For Removing Denture Biofilm A Crossover Randomized TrialDocument5 pagesJurnal 2. Alkaline Peroxides Versus Sodium Hypochlorite For Removing Denture Biofilm A Crossover Randomized Trialfitri dwi123No ratings yet
- Higiene Protesica Revision CriticaDocument9 pagesHigiene Protesica Revision CriticaMonicaNo ratings yet
- Brushing Associated With Oral Irrigation in Maintaining ImplantsDocument11 pagesBrushing Associated With Oral Irrigation in Maintaining ImplantsDanny MartínezNo ratings yet
- PerioDocument6 pagesPeriohusenahNo ratings yet
- Jced 11 E1012Document6 pagesJced 11 E1012Caroline AngoneseNo ratings yet
- 14-Minimum Intervention (Part 2)Document27 pages14-Minimum Intervention (Part 2)Sara MohamedNo ratings yet
- A Clinical Evaluation of A Bleaching Agent Used With and Without Reservoirs Matis Et Al, 2002 IIDocument7 pagesA Clinical Evaluation of A Bleaching Agent Used With and Without Reservoirs Matis Et Al, 2002 IIEugenioNo ratings yet
- Effectiveness OzoneDocument7 pagesEffectiveness OzoneSeptina Anggun PNo ratings yet
- 888 - 019 Florentina RADUDocument7 pages888 - 019 Florentina RADURodica IlincaNo ratings yet
- 888 - 019 Florentina RADUDocument7 pages888 - 019 Florentina RADURodica IlincaNo ratings yet
- Sterilisation of Extracted Human Teeth For Educational Use: Brief CommunicationDocument3 pagesSterilisation of Extracted Human Teeth For Educational Use: Brief CommunicationFebe GracewithaNo ratings yet
- Ijcpd 15 304 (1 4)Document4 pagesIjcpd 15 304 (1 4)Shirley MolinaNo ratings yet
- The Effect of Toothbrushing and Flossing Sequence On Interdental Plaque Reduction and Fluoride RetentionDocument11 pagesThe Effect of Toothbrushing and Flossing Sequence On Interdental Plaque Reduction and Fluoride RetentionMargarita Damas PérezNo ratings yet
- Three MouthwashDocument12 pagesThree MouthwashrashmitanayakNo ratings yet
- Preventive Effect of An Orthodontic Compomer Against Enamel Demineralization Around Bonded BracketsDocument5 pagesPreventive Effect of An Orthodontic Compomer Against Enamel Demineralization Around Bonded BracketsAsep J PermanaNo ratings yet
- Burbridge2007 NoDocument6 pagesBurbridge2007 NoKatherine VilchezNo ratings yet
- Comparative Evaluation of Marginal Integrity of GlassDocument7 pagesComparative Evaluation of Marginal Integrity of Glassbodas de plata Odontologia UNFVNo ratings yet
- Secuencia Del Cepillado Dental PresentacionDocument9 pagesSecuencia Del Cepillado Dental PresentacionElizabeth MartinezNo ratings yet
- Traitrement Non RestorateurDocument19 pagesTraitrement Non Restorateurfz.elgasmi.fzNo ratings yet
- Int J Dental Hygiene - 2023 - Adam - Brushing Behaviour Changes and Plaque Removal With An Electric Toothbrush A ClinicalDocument8 pagesInt J Dental Hygiene - 2023 - Adam - Brushing Behaviour Changes and Plaque Removal With An Electric Toothbrush A Clinicalsarahbening.2No ratings yet
- Cleaning of Removable Dental Prostheses - A Systematic ReviewDocument12 pagesCleaning of Removable Dental Prostheses - A Systematic Reviewandres schlosserNo ratings yet
- 04-April 28-PPC-FissureSealant-Rachma Dewi-20184020019Document7 pages04-April 28-PPC-FissureSealant-Rachma Dewi-20184020019RachmaDewiNo ratings yet
- An 8-Week Randomized Controlled Trial Comparing The Effect of A Novel Oscillating-Rotating Toothbrush Versus A Manual Toothbrush On Plaque ADocument9 pagesAn 8-Week Randomized Controlled Trial Comparing The Effect of A Novel Oscillating-Rotating Toothbrush Versus A Manual Toothbrush On Plaque AMihaiNo ratings yet
- Management of Deep Carious LesionsFrom EverandManagement of Deep Carious LesionsFalk SchwendickeNo ratings yet
- Origin 12 ManualDocument34 pagesOrigin 12 ManualKenshironokenNo ratings yet
- 7 Day Ruqyah Detox Programme - Shaykh 'Adil Ibn Tahir Al-Muqbil - FacebookDocument2 pages7 Day Ruqyah Detox Programme - Shaykh 'Adil Ibn Tahir Al-Muqbil - FacebookR.RNo ratings yet
- PNLE NursingDocument631 pagesPNLE NursingLenaj Ebron50% (2)
- Ten Million Trees Later - First ChapterDocument14 pagesTen Million Trees Later - First ChapterLarsNo ratings yet
- Does Social Class Affect Your Mental Health - PPTX 1Document16 pagesDoes Social Class Affect Your Mental Health - PPTX 1karah13No ratings yet
- 13 - Photosynthesis AQA BookletDocument28 pages13 - Photosynthesis AQA BookletSevilay CaferogluNo ratings yet
- The Health Anxiety Inventory Development and Validation of Scales For The Measurement of Health Anxiety and HypochondriasisDocument11 pagesThe Health Anxiety Inventory Development and Validation of Scales For The Measurement of Health Anxiety and HypochondriasisJan LAWNo ratings yet
- FDSS CARES Meals Assistance Gift Card Application FormDocument1 pageFDSS CARES Meals Assistance Gift Card Application FormFauquier NowNo ratings yet
- PolymerDocument2 pagesPolymermmmd.krmv.00No ratings yet
- Madworx Rate ProposalDocument3 pagesMadworx Rate ProposalNoriega LaneeNo ratings yet
- From The Rest: Read The Passage and Choose The Best Answer For Each Blank. The DolphinDocument3 pagesFrom The Rest: Read The Passage and Choose The Best Answer For Each Blank. The DolphinHa TranNo ratings yet
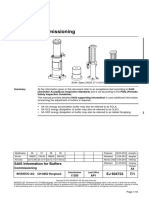
- Commissioning: SAIS Information For BuffersDocument16 pagesCommissioning: SAIS Information For BuffersAli DiabNo ratings yet
- Suspended Ceiling 401Document4 pagesSuspended Ceiling 401johnking5555No ratings yet
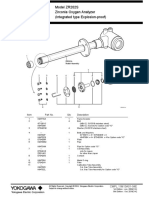
- CELL OxigenoDocument1 pageCELL OxigenopedrogutizNo ratings yet
- 10ME6307 Advanced Thermodynamics and Combustion IA 2 QPDocument2 pages10ME6307 Advanced Thermodynamics and Combustion IA 2 QPDeepakNo ratings yet
- Bomba SKC 222 ManualDocument11 pagesBomba SKC 222 ManualEderson GuimaraesNo ratings yet
- Precios Febrero SocofarDocument9 pagesPrecios Febrero SocofarAdidaspuma ReplicasNo ratings yet
- AP GIS GO NO 131 W.E.F Oct 2018 - 30-06-2019Document6 pagesAP GIS GO NO 131 W.E.F Oct 2018 - 30-06-2019Sivareddy50% (2)
- Rooftop Fish FarmsDocument4 pagesRooftop Fish FarmsbobsraineyNo ratings yet
- Utilization of Garlic (Allium Sativum), Sand, Pebbles and Corn Cob Charcoal For Greywater TreatmentDocument65 pagesUtilization of Garlic (Allium Sativum), Sand, Pebbles and Corn Cob Charcoal For Greywater TreatmentRed AngelNo ratings yet
- AUBF - Lec Chapter 3 4 5 COMPLETE - Transes 1Document18 pagesAUBF - Lec Chapter 3 4 5 COMPLETE - Transes 1Princess Eve OlowanNo ratings yet
- T3 User Manual PDFDocument11 pagesT3 User Manual PDFrudy wibisonoNo ratings yet
- 2 Kind of Carts. 3 Colors. 6 SizeDocument16 pages2 Kind of Carts. 3 Colors. 6 SizeAlesioNo ratings yet
- Failure of Eruption of Posterior TeethDocument5 pagesFailure of Eruption of Posterior TeethSara SaedNo ratings yet
- STA002 - FAEO and RelatedDocument6 pagesSTA002 - FAEO and RelatedpierrebkkNo ratings yet
- Corken CompressorI100Document16 pagesCorken CompressorI100adriansya7No ratings yet
- Agua Mineral NaturalDocument4 pagesAgua Mineral NaturalSara SánNo ratings yet
- TOS in PE 10Document3 pagesTOS in PE 10Aljon Cainto OperarioNo ratings yet