
Bassi, Attux - 2022
Bassi, Attux - 2022
You might also like
- Raphex 2001 QuestionsDocument56 pagesRaphex 2001 QuestionsFelipe FeijóNo ratings yet
- Kelvinator No Frost Wiring DiagramDocument3 pagesKelvinator No Frost Wiring DiagramLuis Pereira Peña100% (1)
- Raphex 2002 AnswersDocument30 pagesRaphex 2002 Answersapatz100% (2)
- Raphex 2003 AnswersDocument31 pagesRaphex 2003 Answersapatz100% (1)
- Principles of TurbomachineryDocument276 pagesPrinciples of TurbomachineryNavneet PAndeNo ratings yet
- ALD Additive Manufacturing VIGA-EIGA Broschure-1 PDFDocument4 pagesALD Additive Manufacturing VIGA-EIGA Broschure-1 PDFVenkateswaran KrishnamurthyNo ratings yet
- 1 s2.0 S0957417422016372 MainDocument14 pages1 s2.0 S0957417422016372 MainMd NahiduzzamanNo ratings yet
- Pneumonia Detection: Department of CSE, NITDocument17 pagesPneumonia Detection: Department of CSE, NITAkashNo ratings yet
- AP20110010028 (Preview)Document1 pageAP20110010028 (Preview)Sameer Thadimarri AP20110010028No ratings yet
- Covid-19 Detection From Chest X-RaysDocument7 pagesCovid-19 Detection From Chest X-RaysAman OsanNo ratings yet
- Detection of COVID-19 From X-Rays Using Hybrid Deep Learning ModelsDocument9 pagesDetection of COVID-19 From X-Rays Using Hybrid Deep Learning ModelsasdNo ratings yet
- Performance Analysis of Various Deep Learning Algorithms in COVID-19 Detection With Chest X-RAY ImagesDocument8 pagesPerformance Analysis of Various Deep Learning Algorithms in COVID-19 Detection With Chest X-RAY Imageslaxmi.slvNo ratings yet
- Covid-Densenet: A Deep Learning Architecture To Detect Covid-19 From Chest Radiology ImagesDocument5 pagesCovid-Densenet: A Deep Learning Architecture To Detect Covid-19 From Chest Radiology ImagesDhruv TNo ratings yet
- Application of Deep Learning Techniques For Detection of COVID-19 Casesusing Chest X-Ray Images A Comprehensive StudyDocument12 pagesApplication of Deep Learning Techniques For Detection of COVID-19 Casesusing Chest X-Ray Images A Comprehensive StudyHarshini N BNo ratings yet
- Anapub Paper TemplateDocument10 pagesAnapub Paper Templatebdhiyanu87No ratings yet
- Learning To Augment Incorporated Noise Robust Deep CNN - 2022 - Journal of CompuDocument14 pagesLearning To Augment Incorporated Noise Robust Deep CNN - 2022 - Journal of CompudeivisNo ratings yet
- CovidGAN Data Augmentation Using AuxiliaryDocument8 pagesCovidGAN Data Augmentation Using AuxiliaryPlacido Rogerio PinheiroNo ratings yet
- Covid-Densenet: A Deep Learning Architecture To Detect Covid-19 From Chest Radiology ImagesDocument11 pagesCovid-Densenet: A Deep Learning Architecture To Detect Covid-19 From Chest Radiology ImagesAriba Yusuf TubaNo ratings yet
- Comparison of Deep Learning Algorithms For Pneumonia DetectionDocument5 pagesComparison of Deep Learning Algorithms For Pneumonia DetectionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diagnosis of COVID-19 Using Deep Neural Networks andDocument12 pagesDiagnosis of COVID-19 Using Deep Neural Networks andsuman DasNo ratings yet
- Assessment of Convolutional Neural Networks For Automated Classification of Chest RadiographsDocument8 pagesAssessment of Convolutional Neural Networks For Automated Classification of Chest RadiographsFaisal AsadiNo ratings yet
- Proceedings of Spie: Transfer Learning Methods For Classification of COVID-19 Chest X-Ray ImagesDocument8 pagesProceedings of Spie: Transfer Learning Methods For Classification of COVID-19 Chest X-Ray ImagesAriba Yusuf TubaNo ratings yet
- A Deep Learning-Based COVID-19 Automatic Diagnostic Framework Using Chest X-Ray ImagesDocument16 pagesA Deep Learning-Based COVID-19 Automatic Diagnostic Framework Using Chest X-Ray ImagesEshaNo ratings yet
- Document3 TexDocument4 pagesDocument3 TexNavin M ANo ratings yet
- s12652 021 03075 2Document8 pagess12652 021 03075 2Wiena AviolitaNo ratings yet
- Using Deep Learning To Detect Pneumonia Caused by NCOV-19 From X-Ray Images - by Ayrton San Joaquin - Towards Data ScienceDocument7 pagesUsing Deep Learning To Detect Pneumonia Caused by NCOV-19 From X-Ray Images - by Ayrton San Joaquin - Towards Data ScienceECE BNo ratings yet
- Deep Learning Approach For Unprecedented Lung Disease PrognosisDocument5 pagesDeep Learning Approach For Unprecedented Lung Disease PrognosisMulla Abdul FaheemNo ratings yet
- Seminar Report Final Year CT ScanDocument13 pagesSeminar Report Final Year CT ScanKapil SidhpuriaNo ratings yet
- Covid 19Document18 pagesCovid 19AISHWARYA PANDITNo ratings yet
- Chest X Ray Detection Project ReportDocument45 pagesChest X Ray Detection Project ReportNikhil Sharma100% (1)
- COVID-19 DetectionDocument15 pagesCOVID-19 Detectionhamidnasiri1369No ratings yet
- Born PocovidDocument14 pagesBorn PocovidRani Henty NovitaNo ratings yet
- Deep Transfer Learning Based Classification Model For Covid-19 Using Chest CT-scansDocument7 pagesDeep Transfer Learning Based Classification Model For Covid-19 Using Chest CT-scansGeen LifeNo ratings yet
- 1 s2.0 S0208521621001303 MainDocument15 pages1 s2.0 S0208521621001303 MainShivam GuptaNo ratings yet
- Paper2 15pagesDocument15 pagesPaper2 15pagesCharlène Béatrice Bridge NduwimanaNo ratings yet
- Baltruschat Et Al. - 2019Document10 pagesBaltruschat Et Al. - 2019apatzNo ratings yet
- Research Article An Improved Covid-19 Detection Using Gan-Based Data Augmentation and Novel Qunet-Based ClassificationDocument9 pagesResearch Article An Improved Covid-19 Detection Using Gan-Based Data Augmentation and Novel Qunet-Based ClassificationNaoual NassiriNo ratings yet
- IJEET TemplateDocument5 pagesIJEET TemplateIgt SuryawanNo ratings yet
- Detecting COVID-19 in X-Ray Images With Deep Learning: Dev Burman July 2020Document5 pagesDetecting COVID-19 in X-Ray Images With Deep Learning: Dev Burman July 2020dev burmanNo ratings yet
- Deep Neural Network Ensemble For Pneumonia LocalizationDocument12 pagesDeep Neural Network Ensemble For Pneumonia LocalizationAmílcar CáceresNo ratings yet
- (IJCST-V11I2P5) :Dr.S.Selvakani, K.Vasumathi, M.GopiDocument5 pages(IJCST-V11I2P5) :Dr.S.Selvakani, K.Vasumathi, M.GopiEighthSenseGroupNo ratings yet
- Classification of COVID-19 in Chest X-Ray Images UDocument9 pagesClassification of COVID-19 in Chest X-Ray Images UMD. SAGAR HOSSAINNo ratings yet
- 1 s2.0 S2214785322034812 MainDocument7 pages1 s2.0 S2214785322034812 MainSantai JakNo ratings yet
- Measurement: Amit Kumar Jaiswal, Prayag Tiwari, Sachin Kumar, Deepak Gupta, Ashish Khanna, Joel J.P.C. RodriguesDocument8 pagesMeasurement: Amit Kumar Jaiswal, Prayag Tiwari, Sachin Kumar, Deepak Gupta, Ashish Khanna, Joel J.P.C. RodriguesDiego Alejandro Betancourt PradaNo ratings yet
- Shibu George Et Al. - 2023Document16 pagesShibu George Et Al. - 2023apatzNo ratings yet
- Diagnosis of Pneumonia From Chest X-Ray Images Using Deep LearningDocument5 pagesDiagnosis of Pneumonia From Chest X-Ray Images Using Deep LearningShoumik MuhtasimNo ratings yet
- Artificial Intelligence 1Document8 pagesArtificial Intelligence 1Andy BaiNo ratings yet
- Deepln: An Artificial Intelligence-Based Automated System For Lung Cancer ScreeningDocument12 pagesDeepln: An Artificial Intelligence-Based Automated System For Lung Cancer ScreeningNexgen TechnologyNo ratings yet
- Coronavirus COVID 19 Detection From Chest Radiology Images UsingDocument6 pagesCoronavirus COVID 19 Detection From Chest Radiology Images UsingHabiba AhmedNo ratings yet
- (IJCST-V11I3P1) :Dr.P.Bhaskar Naidu, P.Mary Harika, J.Pavani, B.Divyadhatri, J.ChandanaDocument4 pages(IJCST-V11I3P1) :Dr.P.Bhaskar Naidu, P.Mary Harika, J.Pavani, B.Divyadhatri, J.ChandanaEighthSenseGroupNo ratings yet
- Efficient Lung Infection Detection Using Machine Learning ApproachDocument9 pagesEfficient Lung Infection Detection Using Machine Learning ApproachIJRASETPublicationsNo ratings yet
- Expert Systems With ApplicationsDocument13 pagesExpert Systems With ApplicationsSUNDARAMAHALINGAM ANo ratings yet
- Covid-19 Detection Using Deep Learning With Transfer LearningDocument6 pagesCovid-19 Detection Using Deep Learning With Transfer LearningTJPRC PublicationsNo ratings yet
- EMCNet Automated COVID-19 Diagnosis From X-Ray Images Using Convolutional Neural Network and Ensemble of Machine Learning ClassifiersDocument12 pagesEMCNet Automated COVID-19 Diagnosis From X-Ray Images Using Convolutional Neural Network and Ensemble of Machine Learning ClassifiersmodhafakaNo ratings yet
- 2023 An Improved Faster R-CNN Algorithm For Assisted Detection of Lung NodulesDocument9 pages2023 An Improved Faster R-CNN Algorithm For Assisted Detection of Lung NodulesgraythomasinNo ratings yet
- Automatic Detection of Pneumonia On Compressed Sensing Images Using Deep LearningDocument4 pagesAutomatic Detection of Pneumonia On Compressed Sensing Images Using Deep LearningRahul ShettyNo ratings yet
- Convolutional Neural Network Based Lungs Diseases PredictionDocument3 pagesConvolutional Neural Network Based Lungs Diseases Predictionshirsat.deep18No ratings yet
- B.Tech Project - I (7Th Semester 2020-2021) Synopsis: Generation of Covid-19 Chest CT Scan Images Using GansDocument4 pagesB.Tech Project - I (7Th Semester 2020-2021) Synopsis: Generation of Covid-19 Chest CT Scan Images Using Gans2K18/CO/330 SAVIOUR VIYADIS MINJNo ratings yet
- Classification of COVID-19 Chest X-Rays With Deep Learning: New Models or Fine Tuning?Document11 pagesClassification of COVID-19 Chest X-Rays With Deep Learning: New Models or Fine Tuning?codelover0007No ratings yet
- Çallı Et Al. - 2021Document29 pagesÇallı Et Al. - 2021apatzNo ratings yet
- Deep Learning Based Automated Chest X-Ray Abnormalities DetectionDocument12 pagesDeep Learning Based Automated Chest X-Ray Abnormalities DetectionTusher Kumar SahaNo ratings yet
- 项目论文2:美国有线电视新闻网医学影像诊断新冠肺炎感染综述Document8 pages项目论文2:美国有线电视新闻网医学影像诊断新冠肺炎感染综述lujunNo ratings yet
- 2020 08 24 20181339v2 FullDocument16 pages2020 08 24 20181339v2 Fullzaynab adeolaNo ratings yet
- GULMEZDocument25 pagesGULMEZmathiu ratataNo ratings yet
- Covi-Assist Automatic COVID-19 Detection From Chest X-RaysDocument10 pagesCovi-Assist Automatic COVID-19 Detection From Chest X-RaysIJRASETPublicationsNo ratings yet
- Thangaraj Et Al. - 2023Document14 pagesThangaraj Et Al. - 2023apatzNo ratings yet
- Bashar Et Al. - 2021Document18 pagesBashar Et Al. - 2021apatzNo ratings yet
- The Bibliometric Analysis of Scholarly Production How Great Is The ImpactDocument23 pagesThe Bibliometric Analysis of Scholarly Production How Great Is The ImpactapatzNo ratings yet
- The Top 100 Most Cited Articles On Artificial Intelligence in RadiologyDocument8 pagesThe Top 100 Most Cited Articles On Artificial Intelligence in RadiologyapatzNo ratings yet
- Bibliometric Methods Pitfalls and PossibilitiesDocument15 pagesBibliometric Methods Pitfalls and PossibilitiesapatzNo ratings yet
- Shibu George Et Al. - 2023Document16 pagesShibu George Et Al. - 2023apatzNo ratings yet
- Soundrapandiyan Et Al. - 2023Document18 pagesSoundrapandiyan Et Al. - 2023apatzNo ratings yet
- Nawaz Et Al. - 2023Document16 pagesNawaz Et Al. - 2023apatzNo ratings yet
- Sadeghi Et Al. - 2023Document18 pagesSadeghi Et Al. - 2023apatzNo ratings yet
- Paul Et Al. - 2023Document15 pagesPaul Et Al. - 2023apatzNo ratings yet
- Elbarougy Et Al. - 2023Document16 pagesElbarougy Et Al. - 2023apatzNo ratings yet
- Bhosale, Patnaik - 2023Document17 pagesBhosale, Patnaik - 2023apatzNo ratings yet
- Raphex 2005 QuestionsDocument54 pagesRaphex 2005 QuestionsapatzNo ratings yet
- Ahmad Et Al. - 2023Document19 pagesAhmad Et Al. - 2023apatzNo ratings yet
- Raphex 2004 QuestionsDocument55 pagesRaphex 2004 QuestionsapatzNo ratings yet
- Raphex 2001 AnswersDocument29 pagesRaphex 2001 AnswersapatzNo ratings yet
- Raphex 1998 AnswersDocument29 pagesRaphex 1998 AnswersapatzNo ratings yet
- Raphex 1998 QuestionsDocument53 pagesRaphex 1998 QuestionsapatzNo ratings yet
- Raphex 1996 AnswersDocument25 pagesRaphex 1996 AnswersapatzNo ratings yet
- Raphex 1996 QuestionsDocument47 pagesRaphex 1996 QuestionsapatzNo ratings yet
- SL - No Questions: MODULE 1: Discrete Fourier TransformDocument5 pagesSL - No Questions: MODULE 1: Discrete Fourier TransformarunNo ratings yet
- Civil Design That Puts You in The Passing LaneDocument4 pagesCivil Design That Puts You in The Passing Lanebbutros_317684077No ratings yet
- MT 226:partial Differential EquationsDocument75 pagesMT 226:partial Differential EquationsPaul ObadiahNo ratings yet
- QJAR's Robot CatalogueDocument6 pagesQJAR's Robot CatalogueVioleta Marinkovic Ex SavicicNo ratings yet
- Magnesium Sterate Mixing in V BlenderDocument12 pagesMagnesium Sterate Mixing in V Blendermaneshdixit4312No ratings yet
- Winac RTX 2010 Manual en-US en-US 0123Document296 pagesWinac RTX 2010 Manual en-US en-US 0123Riki PermanaNo ratings yet
- Open-Ocean Barrier Islands: Global in Uence of Climatic, Oceanographic, and Depositional SettingsDocument17 pagesOpen-Ocean Barrier Islands: Global in Uence of Climatic, Oceanographic, and Depositional SettingsMicheleFontanaNo ratings yet
- 03-03-14 Functionality BRAUMAT ClassicDocument0 pages03-03-14 Functionality BRAUMAT ClassicDo Van TuNo ratings yet
- Principles of Database and Knowledge Base Systems Volume 1 1 PDFDocument654 pagesPrinciples of Database and Knowledge Base Systems Volume 1 1 PDFJoaquín ValleNo ratings yet
- Pure Maths Formula SheetDocument20 pagesPure Maths Formula SheetSaifur Rahman Raffael100% (1)
- Kuis NPV Vs IRR (CH 5 and 6)Document4 pagesKuis NPV Vs IRR (CH 5 and 6)Imelda HotmariaNo ratings yet
- Music Theory (Jason Allen) (Summarized by Elve)Document28 pagesMusic Theory (Jason Allen) (Summarized by Elve)elveNo ratings yet
- MODULE 5 - PRS Handling - UTMDocument32 pagesMODULE 5 - PRS Handling - UTMgavin.vedder1980No ratings yet
- Applications of Algebra To A Problem in Topology - by Michael HopkinsDocument49 pagesApplications of Algebra To A Problem in Topology - by Michael HopkinsThe Simons Foundation100% (1)
- (PDF) 1996 - Goodridge - Comments On Regional Simulations of Greenhouse Warming Including Natural VariabilityDocument2 pages(PDF) 1996 - Goodridge - Comments On Regional Simulations of Greenhouse Warming Including Natural Variabilitybafuncio100% (1)
- Podar International School Chinchwad STD Xi - (I Unit Test) Subject: Computer Science Date: 8-9-2020 Marks: 40Document3 pagesPodar International School Chinchwad STD Xi - (I Unit Test) Subject: Computer Science Date: 8-9-2020 Marks: 40Shriniwas KulkarniNo ratings yet
- 2014 ForesterDocument7,222 pages2014 ForesterMykhail KubasovNo ratings yet
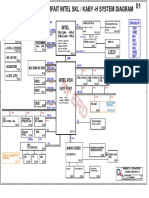
- Power Pavilion Parfait Intel SKL / Kaby - H System DiagramDocument52 pagesPower Pavilion Parfait Intel SKL / Kaby - H System DiagramAbnesis NesisNo ratings yet
- Butt Kicker Concert User GuideDocument8 pagesButt Kicker Concert User GuideJorge Balladares PesantesNo ratings yet
- Comparison of Dissolved Air Flotation and Sedimentation PDFDocument5 pagesComparison of Dissolved Air Flotation and Sedimentation PDFPrie TeaNo ratings yet
- Accurex, Model XXEW-10.0 Wall-Mounted Canopy Exhaust Hood Performance ReportDocument23 pagesAccurex, Model XXEW-10.0 Wall-Mounted Canopy Exhaust Hood Performance ReportProingmeca CANo ratings yet
- Least Learned Skills 4TH Q 2019 2020Document1 pageLeast Learned Skills 4TH Q 2019 2020Arben Joy UrmatanNo ratings yet
- Automation 2 Topic 1: Design A Simple Process Control SystemDocument12 pagesAutomation 2 Topic 1: Design A Simple Process Control SystemChriscarl De LimaNo ratings yet
- CE023 LABORATORY MANUAL 2nd RevisionDocument72 pagesCE023 LABORATORY MANUAL 2nd RevisionernestNo ratings yet
- L L L L L L: Answer The Following Questions. Answer The Following Questions. Answer The Following QuestionsDocument1 pageL L L L L L: Answer The Following Questions. Answer The Following Questions. Answer The Following QuestionsBasappaSarkarNo ratings yet
- Nptel: Power Electronics Applications To Power Systems - Video CourseDocument2 pagesNptel: Power Electronics Applications To Power Systems - Video Courseprafful666No ratings yet
- Chapter 7 Shell Tube Heat ExchangerDocument138 pagesChapter 7 Shell Tube Heat ExchangerPHƯƠNG ĐẶNG YẾNNo ratings yet














































































































Download as pdf or txt
You might also like
- Raphex 2001 QuestionsDocument56 pagesRaphex 2001 QuestionsFelipe FeijóNo ratings yet
- Kelvinator No Frost Wiring DiagramDocument3 pagesKelvinator No Frost Wiring DiagramLuis Pereira Peña100% (1)
- Raphex 2002 AnswersDocument30 pagesRaphex 2002 Answersapatz100% (2)
- Raphex 2003 AnswersDocument31 pagesRaphex 2003 Answersapatz100% (1)
- Principles of TurbomachineryDocument276 pagesPrinciples of TurbomachineryNavneet PAndeNo ratings yet
- ALD Additive Manufacturing VIGA-EIGA Broschure-1 PDFDocument4 pagesALD Additive Manufacturing VIGA-EIGA Broschure-1 PDFVenkateswaran KrishnamurthyNo ratings yet
- 1 s2.0 S0957417422016372 MainDocument14 pages1 s2.0 S0957417422016372 MainMd NahiduzzamanNo ratings yet
- Pneumonia Detection: Department of CSE, NITDocument17 pagesPneumonia Detection: Department of CSE, NITAkashNo ratings yet
- AP20110010028 (Preview)Document1 pageAP20110010028 (Preview)Sameer Thadimarri AP20110010028No ratings yet
- Covid-19 Detection From Chest X-RaysDocument7 pagesCovid-19 Detection From Chest X-RaysAman OsanNo ratings yet
- Detection of COVID-19 From X-Rays Using Hybrid Deep Learning ModelsDocument9 pagesDetection of COVID-19 From X-Rays Using Hybrid Deep Learning ModelsasdNo ratings yet
- Performance Analysis of Various Deep Learning Algorithms in COVID-19 Detection With Chest X-RAY ImagesDocument8 pagesPerformance Analysis of Various Deep Learning Algorithms in COVID-19 Detection With Chest X-RAY Imageslaxmi.slvNo ratings yet
- Covid-Densenet: A Deep Learning Architecture To Detect Covid-19 From Chest Radiology ImagesDocument5 pagesCovid-Densenet: A Deep Learning Architecture To Detect Covid-19 From Chest Radiology ImagesDhruv TNo ratings yet
- Application of Deep Learning Techniques For Detection of COVID-19 Casesusing Chest X-Ray Images A Comprehensive StudyDocument12 pagesApplication of Deep Learning Techniques For Detection of COVID-19 Casesusing Chest X-Ray Images A Comprehensive StudyHarshini N BNo ratings yet
- Anapub Paper TemplateDocument10 pagesAnapub Paper Templatebdhiyanu87No ratings yet
- Learning To Augment Incorporated Noise Robust Deep CNN - 2022 - Journal of CompuDocument14 pagesLearning To Augment Incorporated Noise Robust Deep CNN - 2022 - Journal of CompudeivisNo ratings yet
- CovidGAN Data Augmentation Using AuxiliaryDocument8 pagesCovidGAN Data Augmentation Using AuxiliaryPlacido Rogerio PinheiroNo ratings yet
- Covid-Densenet: A Deep Learning Architecture To Detect Covid-19 From Chest Radiology ImagesDocument11 pagesCovid-Densenet: A Deep Learning Architecture To Detect Covid-19 From Chest Radiology ImagesAriba Yusuf TubaNo ratings yet
- Comparison of Deep Learning Algorithms For Pneumonia DetectionDocument5 pagesComparison of Deep Learning Algorithms For Pneumonia DetectionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diagnosis of COVID-19 Using Deep Neural Networks andDocument12 pagesDiagnosis of COVID-19 Using Deep Neural Networks andsuman DasNo ratings yet
- Assessment of Convolutional Neural Networks For Automated Classification of Chest RadiographsDocument8 pagesAssessment of Convolutional Neural Networks For Automated Classification of Chest RadiographsFaisal AsadiNo ratings yet
- Proceedings of Spie: Transfer Learning Methods For Classification of COVID-19 Chest X-Ray ImagesDocument8 pagesProceedings of Spie: Transfer Learning Methods For Classification of COVID-19 Chest X-Ray ImagesAriba Yusuf TubaNo ratings yet
- A Deep Learning-Based COVID-19 Automatic Diagnostic Framework Using Chest X-Ray ImagesDocument16 pagesA Deep Learning-Based COVID-19 Automatic Diagnostic Framework Using Chest X-Ray ImagesEshaNo ratings yet
- Document3 TexDocument4 pagesDocument3 TexNavin M ANo ratings yet
- s12652 021 03075 2Document8 pagess12652 021 03075 2Wiena AviolitaNo ratings yet
- Using Deep Learning To Detect Pneumonia Caused by NCOV-19 From X-Ray Images - by Ayrton San Joaquin - Towards Data ScienceDocument7 pagesUsing Deep Learning To Detect Pneumonia Caused by NCOV-19 From X-Ray Images - by Ayrton San Joaquin - Towards Data ScienceECE BNo ratings yet
- Deep Learning Approach For Unprecedented Lung Disease PrognosisDocument5 pagesDeep Learning Approach For Unprecedented Lung Disease PrognosisMulla Abdul FaheemNo ratings yet
- Seminar Report Final Year CT ScanDocument13 pagesSeminar Report Final Year CT ScanKapil SidhpuriaNo ratings yet
- Covid 19Document18 pagesCovid 19AISHWARYA PANDITNo ratings yet
- Chest X Ray Detection Project ReportDocument45 pagesChest X Ray Detection Project ReportNikhil Sharma100% (1)
- COVID-19 DetectionDocument15 pagesCOVID-19 Detectionhamidnasiri1369No ratings yet
- Born PocovidDocument14 pagesBorn PocovidRani Henty NovitaNo ratings yet
- Deep Transfer Learning Based Classification Model For Covid-19 Using Chest CT-scansDocument7 pagesDeep Transfer Learning Based Classification Model For Covid-19 Using Chest CT-scansGeen LifeNo ratings yet
- 1 s2.0 S0208521621001303 MainDocument15 pages1 s2.0 S0208521621001303 MainShivam GuptaNo ratings yet
- Paper2 15pagesDocument15 pagesPaper2 15pagesCharlène Béatrice Bridge NduwimanaNo ratings yet
- Baltruschat Et Al. - 2019Document10 pagesBaltruschat Et Al. - 2019apatzNo ratings yet
- Research Article An Improved Covid-19 Detection Using Gan-Based Data Augmentation and Novel Qunet-Based ClassificationDocument9 pagesResearch Article An Improved Covid-19 Detection Using Gan-Based Data Augmentation and Novel Qunet-Based ClassificationNaoual NassiriNo ratings yet
- IJEET TemplateDocument5 pagesIJEET TemplateIgt SuryawanNo ratings yet
- Detecting COVID-19 in X-Ray Images With Deep Learning: Dev Burman July 2020Document5 pagesDetecting COVID-19 in X-Ray Images With Deep Learning: Dev Burman July 2020dev burmanNo ratings yet
- Deep Neural Network Ensemble For Pneumonia LocalizationDocument12 pagesDeep Neural Network Ensemble For Pneumonia LocalizationAmílcar CáceresNo ratings yet
- (IJCST-V11I2P5) :Dr.S.Selvakani, K.Vasumathi, M.GopiDocument5 pages(IJCST-V11I2P5) :Dr.S.Selvakani, K.Vasumathi, M.GopiEighthSenseGroupNo ratings yet
- Classification of COVID-19 in Chest X-Ray Images UDocument9 pagesClassification of COVID-19 in Chest X-Ray Images UMD. SAGAR HOSSAINNo ratings yet
- 1 s2.0 S2214785322034812 MainDocument7 pages1 s2.0 S2214785322034812 MainSantai JakNo ratings yet
- Measurement: Amit Kumar Jaiswal, Prayag Tiwari, Sachin Kumar, Deepak Gupta, Ashish Khanna, Joel J.P.C. RodriguesDocument8 pagesMeasurement: Amit Kumar Jaiswal, Prayag Tiwari, Sachin Kumar, Deepak Gupta, Ashish Khanna, Joel J.P.C. RodriguesDiego Alejandro Betancourt PradaNo ratings yet
- Shibu George Et Al. - 2023Document16 pagesShibu George Et Al. - 2023apatzNo ratings yet
- Diagnosis of Pneumonia From Chest X-Ray Images Using Deep LearningDocument5 pagesDiagnosis of Pneumonia From Chest X-Ray Images Using Deep LearningShoumik MuhtasimNo ratings yet
- Artificial Intelligence 1Document8 pagesArtificial Intelligence 1Andy BaiNo ratings yet
- Deepln: An Artificial Intelligence-Based Automated System For Lung Cancer ScreeningDocument12 pagesDeepln: An Artificial Intelligence-Based Automated System For Lung Cancer ScreeningNexgen TechnologyNo ratings yet
- Coronavirus COVID 19 Detection From Chest Radiology Images UsingDocument6 pagesCoronavirus COVID 19 Detection From Chest Radiology Images UsingHabiba AhmedNo ratings yet
- (IJCST-V11I3P1) :Dr.P.Bhaskar Naidu, P.Mary Harika, J.Pavani, B.Divyadhatri, J.ChandanaDocument4 pages(IJCST-V11I3P1) :Dr.P.Bhaskar Naidu, P.Mary Harika, J.Pavani, B.Divyadhatri, J.ChandanaEighthSenseGroupNo ratings yet
- Efficient Lung Infection Detection Using Machine Learning ApproachDocument9 pagesEfficient Lung Infection Detection Using Machine Learning ApproachIJRASETPublicationsNo ratings yet
- Expert Systems With ApplicationsDocument13 pagesExpert Systems With ApplicationsSUNDARAMAHALINGAM ANo ratings yet
- Covid-19 Detection Using Deep Learning With Transfer LearningDocument6 pagesCovid-19 Detection Using Deep Learning With Transfer LearningTJPRC PublicationsNo ratings yet
- EMCNet Automated COVID-19 Diagnosis From X-Ray Images Using Convolutional Neural Network and Ensemble of Machine Learning ClassifiersDocument12 pagesEMCNet Automated COVID-19 Diagnosis From X-Ray Images Using Convolutional Neural Network and Ensemble of Machine Learning ClassifiersmodhafakaNo ratings yet
- 2023 An Improved Faster R-CNN Algorithm For Assisted Detection of Lung NodulesDocument9 pages2023 An Improved Faster R-CNN Algorithm For Assisted Detection of Lung NodulesgraythomasinNo ratings yet
- Automatic Detection of Pneumonia On Compressed Sensing Images Using Deep LearningDocument4 pagesAutomatic Detection of Pneumonia On Compressed Sensing Images Using Deep LearningRahul ShettyNo ratings yet
- Convolutional Neural Network Based Lungs Diseases PredictionDocument3 pagesConvolutional Neural Network Based Lungs Diseases Predictionshirsat.deep18No ratings yet
- B.Tech Project - I (7Th Semester 2020-2021) Synopsis: Generation of Covid-19 Chest CT Scan Images Using GansDocument4 pagesB.Tech Project - I (7Th Semester 2020-2021) Synopsis: Generation of Covid-19 Chest CT Scan Images Using Gans2K18/CO/330 SAVIOUR VIYADIS MINJNo ratings yet
- Classification of COVID-19 Chest X-Rays With Deep Learning: New Models or Fine Tuning?Document11 pagesClassification of COVID-19 Chest X-Rays With Deep Learning: New Models or Fine Tuning?codelover0007No ratings yet
- Çallı Et Al. - 2021Document29 pagesÇallı Et Al. - 2021apatzNo ratings yet
- Deep Learning Based Automated Chest X-Ray Abnormalities DetectionDocument12 pagesDeep Learning Based Automated Chest X-Ray Abnormalities DetectionTusher Kumar SahaNo ratings yet
- 项目论文2:美国有线电视新闻网医学影像诊断新冠肺炎感染综述Document8 pages项目论文2:美国有线电视新闻网医学影像诊断新冠肺炎感染综述lujunNo ratings yet
- 2020 08 24 20181339v2 FullDocument16 pages2020 08 24 20181339v2 Fullzaynab adeolaNo ratings yet
- GULMEZDocument25 pagesGULMEZmathiu ratataNo ratings yet
- Covi-Assist Automatic COVID-19 Detection From Chest X-RaysDocument10 pagesCovi-Assist Automatic COVID-19 Detection From Chest X-RaysIJRASETPublicationsNo ratings yet
- Thangaraj Et Al. - 2023Document14 pagesThangaraj Et Al. - 2023apatzNo ratings yet
- Bashar Et Al. - 2021Document18 pagesBashar Et Al. - 2021apatzNo ratings yet
- The Bibliometric Analysis of Scholarly Production How Great Is The ImpactDocument23 pagesThe Bibliometric Analysis of Scholarly Production How Great Is The ImpactapatzNo ratings yet
- The Top 100 Most Cited Articles On Artificial Intelligence in RadiologyDocument8 pagesThe Top 100 Most Cited Articles On Artificial Intelligence in RadiologyapatzNo ratings yet
- Bibliometric Methods Pitfalls and PossibilitiesDocument15 pagesBibliometric Methods Pitfalls and PossibilitiesapatzNo ratings yet
- Shibu George Et Al. - 2023Document16 pagesShibu George Et Al. - 2023apatzNo ratings yet
- Soundrapandiyan Et Al. - 2023Document18 pagesSoundrapandiyan Et Al. - 2023apatzNo ratings yet
- Nawaz Et Al. - 2023Document16 pagesNawaz Et Al. - 2023apatzNo ratings yet
- Sadeghi Et Al. - 2023Document18 pagesSadeghi Et Al. - 2023apatzNo ratings yet
- Paul Et Al. - 2023Document15 pagesPaul Et Al. - 2023apatzNo ratings yet
- Elbarougy Et Al. - 2023Document16 pagesElbarougy Et Al. - 2023apatzNo ratings yet
- Bhosale, Patnaik - 2023Document17 pagesBhosale, Patnaik - 2023apatzNo ratings yet
- Raphex 2005 QuestionsDocument54 pagesRaphex 2005 QuestionsapatzNo ratings yet
- Ahmad Et Al. - 2023Document19 pagesAhmad Et Al. - 2023apatzNo ratings yet
- Raphex 2004 QuestionsDocument55 pagesRaphex 2004 QuestionsapatzNo ratings yet
- Raphex 2001 AnswersDocument29 pagesRaphex 2001 AnswersapatzNo ratings yet
- Raphex 1998 AnswersDocument29 pagesRaphex 1998 AnswersapatzNo ratings yet
- Raphex 1998 QuestionsDocument53 pagesRaphex 1998 QuestionsapatzNo ratings yet
- Raphex 1996 AnswersDocument25 pagesRaphex 1996 AnswersapatzNo ratings yet
- Raphex 1996 QuestionsDocument47 pagesRaphex 1996 QuestionsapatzNo ratings yet
- SL - No Questions: MODULE 1: Discrete Fourier TransformDocument5 pagesSL - No Questions: MODULE 1: Discrete Fourier TransformarunNo ratings yet
- Civil Design That Puts You in The Passing LaneDocument4 pagesCivil Design That Puts You in The Passing Lanebbutros_317684077No ratings yet
- MT 226:partial Differential EquationsDocument75 pagesMT 226:partial Differential EquationsPaul ObadiahNo ratings yet
- QJAR's Robot CatalogueDocument6 pagesQJAR's Robot CatalogueVioleta Marinkovic Ex SavicicNo ratings yet
- Magnesium Sterate Mixing in V BlenderDocument12 pagesMagnesium Sterate Mixing in V Blendermaneshdixit4312No ratings yet
- Winac RTX 2010 Manual en-US en-US 0123Document296 pagesWinac RTX 2010 Manual en-US en-US 0123Riki PermanaNo ratings yet
- Open-Ocean Barrier Islands: Global in Uence of Climatic, Oceanographic, and Depositional SettingsDocument17 pagesOpen-Ocean Barrier Islands: Global in Uence of Climatic, Oceanographic, and Depositional SettingsMicheleFontanaNo ratings yet
- 03-03-14 Functionality BRAUMAT ClassicDocument0 pages03-03-14 Functionality BRAUMAT ClassicDo Van TuNo ratings yet
- Principles of Database and Knowledge Base Systems Volume 1 1 PDFDocument654 pagesPrinciples of Database and Knowledge Base Systems Volume 1 1 PDFJoaquín ValleNo ratings yet
- Pure Maths Formula SheetDocument20 pagesPure Maths Formula SheetSaifur Rahman Raffael100% (1)
- Kuis NPV Vs IRR (CH 5 and 6)Document4 pagesKuis NPV Vs IRR (CH 5 and 6)Imelda HotmariaNo ratings yet
- Music Theory (Jason Allen) (Summarized by Elve)Document28 pagesMusic Theory (Jason Allen) (Summarized by Elve)elveNo ratings yet
- MODULE 5 - PRS Handling - UTMDocument32 pagesMODULE 5 - PRS Handling - UTMgavin.vedder1980No ratings yet
- Applications of Algebra To A Problem in Topology - by Michael HopkinsDocument49 pagesApplications of Algebra To A Problem in Topology - by Michael HopkinsThe Simons Foundation100% (1)
- (PDF) 1996 - Goodridge - Comments On Regional Simulations of Greenhouse Warming Including Natural VariabilityDocument2 pages(PDF) 1996 - Goodridge - Comments On Regional Simulations of Greenhouse Warming Including Natural Variabilitybafuncio100% (1)
- Podar International School Chinchwad STD Xi - (I Unit Test) Subject: Computer Science Date: 8-9-2020 Marks: 40Document3 pagesPodar International School Chinchwad STD Xi - (I Unit Test) Subject: Computer Science Date: 8-9-2020 Marks: 40Shriniwas KulkarniNo ratings yet
- 2014 ForesterDocument7,222 pages2014 ForesterMykhail KubasovNo ratings yet
- Power Pavilion Parfait Intel SKL / Kaby - H System DiagramDocument52 pagesPower Pavilion Parfait Intel SKL / Kaby - H System DiagramAbnesis NesisNo ratings yet
- Butt Kicker Concert User GuideDocument8 pagesButt Kicker Concert User GuideJorge Balladares PesantesNo ratings yet
- Comparison of Dissolved Air Flotation and Sedimentation PDFDocument5 pagesComparison of Dissolved Air Flotation and Sedimentation PDFPrie TeaNo ratings yet
- Accurex, Model XXEW-10.0 Wall-Mounted Canopy Exhaust Hood Performance ReportDocument23 pagesAccurex, Model XXEW-10.0 Wall-Mounted Canopy Exhaust Hood Performance ReportProingmeca CANo ratings yet
- Least Learned Skills 4TH Q 2019 2020Document1 pageLeast Learned Skills 4TH Q 2019 2020Arben Joy UrmatanNo ratings yet
- Automation 2 Topic 1: Design A Simple Process Control SystemDocument12 pagesAutomation 2 Topic 1: Design A Simple Process Control SystemChriscarl De LimaNo ratings yet
- CE023 LABORATORY MANUAL 2nd RevisionDocument72 pagesCE023 LABORATORY MANUAL 2nd RevisionernestNo ratings yet
- L L L L L L: Answer The Following Questions. Answer The Following Questions. Answer The Following QuestionsDocument1 pageL L L L L L: Answer The Following Questions. Answer The Following Questions. Answer The Following QuestionsBasappaSarkarNo ratings yet
- Nptel: Power Electronics Applications To Power Systems - Video CourseDocument2 pagesNptel: Power Electronics Applications To Power Systems - Video Courseprafful666No ratings yet
- Chapter 7 Shell Tube Heat ExchangerDocument138 pagesChapter 7 Shell Tube Heat ExchangerPHƯƠNG ĐẶNG YẾNNo ratings yet