Download as pdf or txt
You might also like
- Art. FisuradosDocument11 pagesArt. FisuradosInma Coronado de la TorreNo ratings yet
- 300 Dental Anatomy Facts VEREY IMPORTNTDocument19 pages300 Dental Anatomy Facts VEREY IMPORTNTOsman SoormaNo ratings yet
- Bjork Facial Development and Tooth EruptionDocument45 pagesBjork Facial Development and Tooth EruptionNataly ComettaNo ratings yet
- Endodontic Retreatment Versus Dental Implants of Teeth With An Uncertain Endodontic Prognosis 3-Year Results From A Randomised Controlled TriaDocument16 pagesEndodontic Retreatment Versus Dental Implants of Teeth With An Uncertain Endodontic Prognosis 3-Year Results From A Randomised Controlled Triadrmezzo68No ratings yet
- Articulopos 2Document8 pagesArticulopos 2JuanitaEnriquezOrtizNo ratings yet
- 2022 Orto X PerioDocument9 pages2022 Orto X PerioKatia ValNo ratings yet
- Sopravvivenza Perioprotesi Di FeboDocument6 pagesSopravvivenza Perioprotesi Di FeboSadeer RiyadNo ratings yet
- Artigo BomDocument6 pagesArtigo BomCiro GassibeNo ratings yet
- Melissa ArticuloDocument11 pagesMelissa ArticuloGLADYS VALENCIANo ratings yet
- Endodontic Retreatment Vs Dental ImplantsDocument17 pagesEndodontic Retreatment Vs Dental ImplantsEstefania VargasNo ratings yet
- INTERDISCIPLINARY APPROACH IN THE TREATMENT OF IMPACTED CANINES - Review and A Case Report PDFDocument6 pagesINTERDISCIPLINARY APPROACH IN THE TREATMENT OF IMPACTED CANINES - Review and A Case Report PDFNingombam Robinson SinghNo ratings yet
- Manfredini Et Al 2016 Orthodontics Is TM PDFDocument6 pagesManfredini Et Al 2016 Orthodontics Is TM PDFKinjal SharmaNo ratings yet
- Laser en OrtodonciaDocument7 pagesLaser en OrtodonciaDiana ElíasNo ratings yet
- Study of Signs and Symptoms of Temporomandibular Disorders in Patients Who Received Orthodontic Treatment in ChildhoodDocument6 pagesStudy of Signs and Symptoms of Temporomandibular Disorders in Patients Who Received Orthodontic Treatment in ChildhoodSage GrimNo ratings yet
- Research Article: Guey-Lin HouDocument8 pagesResearch Article: Guey-Lin HouLouis HutahaeanNo ratings yet
- TMD Before and After Correction of Dentofacial Deformities by Orthodontic and Orthognathic TreatmentDocument7 pagesTMD Before and After Correction of Dentofacial Deformities by Orthodontic and Orthognathic Treatmentcd.brendasotofloresNo ratings yet
- Nuevo 3Document4 pagesNuevo 3Salma FaNo ratings yet
- IVOJI-Contemporary Management of AnDocument8 pagesIVOJI-Contemporary Management of AnivojiNo ratings yet
- 6.14 - EN Relação Entre Tratamento Ortodôntico e Saúde Gengival-Um Estudo Retrospectivo.Document8 pages6.14 - EN Relação Entre Tratamento Ortodôntico e Saúde Gengival-Um Estudo Retrospectivo.JOHNNo ratings yet
- Microbiologic Changes in Subgingival Plaque Before and During The Early Period of Orthodontic TreatmentDocument7 pagesMicrobiologic Changes in Subgingival Plaque Before and During The Early Period of Orthodontic TreatmentargeliaNo ratings yet
- 1clinical Evaluation of Failures of Removable Partial Dentures PDFDocument7 pages1clinical Evaluation of Failures of Removable Partial Dentures PDFcsmalxNo ratings yet
- Post Insertion Complaints of Removable Dental Prostheses: Original ArticleDocument4 pagesPost Insertion Complaints of Removable Dental Prostheses: Original ArticleAhmed KnaniNo ratings yet
- Cre2 10Document15 pagesCre2 10jhonatan gaspariNo ratings yet
- Profile Changes of Patients Treated With and Without Premolar ExtractionsDocument8 pagesProfile Changes of Patients Treated With and Without Premolar Extractionsblogger bloggerNo ratings yet
- Comm Dent Oral Epid - 2002 - Hirotomi - Longitudinal Study On Periodontal Conditions in Healthy Elderly People in JapanDocument9 pagesComm Dent Oral Epid - 2002 - Hirotomi - Longitudinal Study On Periodontal Conditions in Healthy Elderly People in JapanCarlianny EvoletNo ratings yet
- ARAIDocument10 pagesARAILibia LuriNo ratings yet
- Clinical Evaluation of Failures in Removable Partial DenturesDocument6 pagesClinical Evaluation of Failures in Removable Partial DenturesAlina AlexandraNo ratings yet
- Tendência 2021Document7 pagesTendência 2021ludovicoNo ratings yet
- Association Between Trauma From OcclusioDocument6 pagesAssociation Between Trauma From OcclusioClaudia BarbosaNo ratings yet
- Mandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticDocument9 pagesMandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticPAOLA IVETTE MARTINEZ RODRIGUEZNo ratings yet
- 1 s2.0 S0099239913011345 MainDocument5 pages1 s2.0 S0099239913011345 Maindrvivek reddyNo ratings yet
- Denture Stomatitis and Its Predisposing Factors in Denture WearersDocument6 pagesDenture Stomatitis and Its Predisposing Factors in Denture WearersSiti Fatimah Khaerun NisaNo ratings yet
- Current Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDocument10 pagesCurrent Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDONGXU LIUNo ratings yet
- The Philippine Journal of Orthodontics: ISSN: 0115-3498Document42 pagesThe Philippine Journal of Orthodontics: ISSN: 0115-3498Thomas Karl Anthony QUILANGNo ratings yet
- MainDocument11 pagesMainDentist HereNo ratings yet
- Interdisciplinary Orthodontics - A ReviewDocument5 pagesInterdisciplinary Orthodontics - A ReviewGauri KhadeNo ratings yet
- Orto Paro 2Document6 pagesOrto Paro 2adk eijfNo ratings yet
- Oral Health Status in Patients With Fixed OrthodonDocument5 pagesOral Health Status in Patients With Fixed OrthodonMitha Ari CahayaNo ratings yet
- The Impact of The Loss of FRST PermanentDocument9 pagesThe Impact of The Loss of FRST PermanentemadNo ratings yet
- 2019 Orthodontic Management of Traumatized TeethDocument10 pages2019 Orthodontic Management of Traumatized TeethbaridinoNo ratings yet
- Evaluation of Periodontal Parameters On Removable Partial Denture Abutment Teeth With Direct and Indirect Retainers: A 48-Month Follow-UpDocument8 pagesEvaluation of Periodontal Parameters On Removable Partial Denture Abutment Teeth With Direct and Indirect Retainers: A 48-Month Follow-UpGhina AdilahNo ratings yet
- Caninos RetenidosDocument9 pagesCaninos RetenidosNayely MiguelNo ratings yet
- Hindrance of Tooth Eruption and Orthodontic Tooth Movement by Focal Idiopathic Osteosclerosis in The MandibleDocument3 pagesHindrance of Tooth Eruption and Orthodontic Tooth Movement by Focal Idiopathic Osteosclerosis in The MandiblerachmadyNo ratings yet
- 7.mineral Trioxide Aggregate and FormocresolDocument6 pages7.mineral Trioxide Aggregate and FormocresolMihaela TuculinaNo ratings yet
- Biomecanica en Protesis Parcial RemovibleDocument6 pagesBiomecanica en Protesis Parcial RemovibleAyumi MonikNo ratings yet
- Kindelan 2008Document11 pagesKindelan 2008DIANA PAOLA FONTECHA GONZÁLEZNo ratings yet
- Maxillary Dentoalveolar Assessment Following Retraction of Maxillary Incisors: A Preliminary StudyDocument8 pagesMaxillary Dentoalveolar Assessment Following Retraction of Maxillary Incisors: A Preliminary StudyAndrea TokumotoNo ratings yet
- 5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal OcclusionsDocument5 pages5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal Occlusionsthiên lữNo ratings yet
- J Clinic Periodontology - 2021 - Martin - Effect of Orthodontic Therapy in Periodontitis and Non Periodontitis Patients ADocument30 pagesJ Clinic Periodontology - 2021 - Martin - Effect of Orthodontic Therapy in Periodontitis and Non Periodontitis Patients Apaulina becerraNo ratings yet
- Tratamiento Inicial Fase IVDocument6 pagesTratamiento Inicial Fase IVFernando CordovaNo ratings yet
- J Odw 2016 11 006Document6 pagesJ Odw 2016 11 006Ahmed ElsharkawyNo ratings yet
- 9618 Digital Analysis of Occlusion in Adult Post Orthodontic Subjects Using T Scan III and Bioemg III A Pilot StudyDocument9 pages9618 Digital Analysis of Occlusion in Adult Post Orthodontic Subjects Using T Scan III and Bioemg III A Pilot StudyRimNo ratings yet
- Magneticfields PDFDocument5 pagesMagneticfields PDFSergio Di VitantonioNo ratings yet
- Probing Pocket Depth Reduction After Non Surgical Periodontal TherapyDocument11 pagesProbing Pocket Depth Reduction After Non Surgical Periodontal Therapymartesebastian081No ratings yet
- Extrusion Splint Technique in Management of Dental Trauma: A Case ReportDocument5 pagesExtrusion Splint Technique in Management of Dental Trauma: A Case ReportdrvarunmalhotraNo ratings yet
- Association Between Incisor Positions and Amount of Interdental Stripping in Patients Undergoing Orthodontic TreatmentDocument10 pagesAssociation Between Incisor Positions and Amount of Interdental Stripping in Patients Undergoing Orthodontic TreatmentJean-Philippe MercierNo ratings yet
- In Uence of Removable Partial Dentures On Plaque AccumulationDocument8 pagesIn Uence of Removable Partial Dentures On Plaque Accumulationlian liaanNo ratings yet
- UntitledDocument25 pagesUntitledpritasya handayaniNo ratings yet
- A Survey of Orthodontic Treatment in Team Care For Patients With Syndromic Craniosynostosis in JapanDocument8 pagesA Survey of Orthodontic Treatment in Team Care For Patients With Syndromic Craniosynostosis in Japansaja IssaNo ratings yet
- The Influence of Removable Partial Dentures On The Periodontal Health of Abutment and Non Abutment TeethDocument5 pagesThe Influence of Removable Partial Dentures On The Periodontal Health of Abutment and Non Abutment TeethAnthony OrtegaNo ratings yet
- Minimally Invasive Approaches in Endodontic PracticeFrom EverandMinimally Invasive Approaches in Endodontic PracticeGianluca PlotinoNo ratings yet
- Clinical and Radiographic Evaluation of Pulpal and Periradicular Tissue, JR 2016Document5 pagesClinical and Radiographic Evaluation of Pulpal and Periradicular Tissue, JR 20163Racha supremacyNo ratings yet
- D.sign Primarne PloheDocument8 pagesD.sign Primarne PloheGoranNo ratings yet
- ICD 10 Penyakit Gigi Dan MulutDocument5 pagesICD 10 Penyakit Gigi Dan MulutnisrinaqotrunNo ratings yet
- Diagnosis and Treatment Planning in FPDDocument46 pagesDiagnosis and Treatment Planning in FPDSujanaNo ratings yet
- Deep Bite (Dental Update)Document9 pagesDeep Bite (Dental Update)Faisal H RanaNo ratings yet
- OrthoDocument3 pagesOrthohegarNo ratings yet
- The CementumDocument10 pagesThe CementumYousef KhallafNo ratings yet
- Lingualied OcclDocument7 pagesLingualied Occlsiddu76No ratings yet
- Good Occlusal Practice in Restorative DentistryDocument3 pagesGood Occlusal Practice in Restorative DentistryCarmen Breban CirțiuNo ratings yet
- PBL Oral BiologyDocument12 pagesPBL Oral BiologyhusunasanNo ratings yet
- 06 Grenga pp28-29Document2 pages06 Grenga pp28-29OMAR NOLBERTO DIAZ SANCHEZNo ratings yet
- 2020 Naldeman Premature Loss of Primary Anterior TeethDocument26 pages2020 Naldeman Premature Loss of Primary Anterior TeethDiego Andres Hincapie HerreraNo ratings yet
- Guidelines For Maxillary Incisal Edge Position A Pilot Study The Key Is The Canine J Prosthodont 2007Document5 pagesGuidelines For Maxillary Incisal Edge Position A Pilot Study The Key Is The Canine J Prosthodont 2007Iulia Florina SimaNo ratings yet
- Construction Bite of Twin BlockDocument8 pagesConstruction Bite of Twin BlockchaitreeNo ratings yet
- Carta de Formas de Dientes GeneralDocument16 pagesCarta de Formas de Dientes Generaldachu_64No ratings yet
- Occulsal Morphology DeterminantsDocument38 pagesOcculsal Morphology DeterminantsrusschallengerNo ratings yet
- Choosing A Pre-Adjusted Orthodontic Appliance Prescription For Anterior TeethDocument7 pagesChoosing A Pre-Adjusted Orthodontic Appliance Prescription For Anterior TeethAadhirai GopinathNo ratings yet
- Delayed Eruption PDFDocument6 pagesDelayed Eruption PDFIsharajini Prasadika Subhashni GamageNo ratings yet
- Delayed Replantation of Avulsed Tooth - A Case ReportDocument8 pagesDelayed Replantation of Avulsed Tooth - A Case ReportIJAR JOURNALNo ratings yet
- DPP Dental Terms PDFDocument15 pagesDPP Dental Terms PDFana dizonNo ratings yet
- Master Dentistry 2Document5 pagesMaster Dentistry 2Laili Nurul IslamiNo ratings yet
- Extraction ForcepsDocument3 pagesExtraction ForcepsShift UallNo ratings yet
- Development of OcclusionDocument18 pagesDevelopment of OcclusionAshis BiswasNo ratings yet
- Orthodontic Pearls PDFDocument2 pagesOrthodontic Pearls PDFortho123No ratings yet
- Dental AnatomyDocument2 pagesDental AnatomyDN NLLNo ratings yet
- KEY RPD Design ExerciseDocument3 pagesKEY RPD Design ExerciseMichelleNo ratings yet
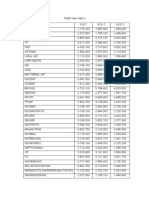
- Tarif Ina CBGDocument2 pagesTarif Ina CBGoctavia tri wulandariNo ratings yet
- Biomechanics of Extra-Alveolar Mini-Implant Use in The Infrazygomatic Crest Area For Asymmetrical Correction of Class II Subdivision MalocclusionDocument9 pagesBiomechanics of Extra-Alveolar Mini-Implant Use in The Infrazygomatic Crest Area For Asymmetrical Correction of Class II Subdivision MalocclusionhabeebNo ratings yet