Download as pdf or txt
You might also like
- Business and Society Stakeholders Ethics Public Policy 17Th Edition Anne Lawrence Full ChapterDocument67 pagesBusiness and Society Stakeholders Ethics Public Policy 17Th Edition Anne Lawrence Full Chaptermichael.lynch15578% (9)
- Sakurai Solutions 5-1 5-2Document8 pagesSakurai Solutions 5-1 5-2Raza Ali RazaNo ratings yet
- PlasentaDocument4 pagesPlasentaLois YunikeNo ratings yet
- Laparoscopic Management of Cervical-Isthmic Pregnancy: A Proposal MethodDocument4 pagesLaparoscopic Management of Cervical-Isthmic Pregnancy: A Proposal MethodDinorah MarcelaNo ratings yet
- Normal Vaginal Delivery at Term After Expectant Management of Heterotopic Caesarean Scar Pregnancy: A Case ReportDocument3 pagesNormal Vaginal Delivery at Term After Expectant Management of Heterotopic Caesarean Scar Pregnancy: A Case Reportdiaaabdallah209No ratings yet
- Caesarean Scar Ectopic Pregnancy: Case ReportDocument3 pagesCaesarean Scar Ectopic Pregnancy: Case ReportDewi SaftariNo ratings yet
- Caso ClinicoDocument3 pagesCaso Clinicojohav91670No ratings yet
- Case Reports in Women's HealthDocument4 pagesCase Reports in Women's Healthowadokunquick3154No ratings yet
- Successful Conservative Treatment of Microinvasive Cervical Cancer During PregnancyDocument3 pagesSuccessful Conservative Treatment of Microinvasive Cervical Cancer During PregnancyEres TriasaNo ratings yet
- Research ArticlesDocument3 pagesResearch ArticlesKeeranmayeeishraNo ratings yet
- Ectopic Abdominal Pregnancies: About 2 CasesDocument10 pagesEctopic Abdominal Pregnancies: About 2 CasesIJAR JOURNALNo ratings yet
- Uterine VaricesDocument3 pagesUterine VaricesCindy AuliaNo ratings yet
- Barel 2019Document3 pagesBarel 2019Mariana González DíazNo ratings yet
- Interesting Case FinalDocument33 pagesInteresting Case Finalazenith dumlaoNo ratings yet
- Unavoidable Myomectomy During Cesarean Section: A Case ReportDocument3 pagesUnavoidable Myomectomy During Cesarean Section: A Case ReportGuia Nina DuranNo ratings yet
- Cesarean Scar Pregnancies and Their ManagementDocument7 pagesCesarean Scar Pregnancies and Their ManagementClinton SitanggangNo ratings yet
- Ectopic Pregnancy in Uncommon Implantation Sites: The Egyptian Journal of Radiology and Nuclear MedicineDocument10 pagesEctopic Pregnancy in Uncommon Implantation Sites: The Egyptian Journal of Radiology and Nuclear MedicinerezachandraNo ratings yet
- Case Report: Recurrent Cesarean Scar Ectopic Pregnancy Treated With Systemic MethotrexateDocument5 pagesCase Report: Recurrent Cesarean Scar Ectopic Pregnancy Treated With Systemic MethotrexatesaryindrianyNo ratings yet
- Placenta Increta Causing Um in The 26th Week of Pregnancy 2Document3 pagesPlacenta Increta Causing Um in The 26th Week of Pregnancy 2Kester ApostolNo ratings yet
- Anterior Cervical Wall Rupture As A Result of Induced AbortionDocument4 pagesAnterior Cervical Wall Rupture As A Result of Induced AbortionnawriirwanNo ratings yet
- 655 NKJDocument5 pages655 NKJEka AriasyahNo ratings yet
- Postpartum Hemorrhage With Associated Placenta PR 2024 International JournalDocument3 pagesPostpartum Hemorrhage With Associated Placenta PR 2024 International JournalRonald QuezadaNo ratings yet
- International Journal of Anesthetics and Anesthesiology Ijaa 6 095Document5 pagesInternational Journal of Anesthetics and Anesthesiology Ijaa 6 095daily of sinta fuNo ratings yet
- 10 1016@j Ijscr 2020 01 020Document4 pages10 1016@j Ijscr 2020 01 020ari naNo ratings yet
- 08 Re-LaparotomyaftercesareanDocument8 pages08 Re-LaparotomyaftercesareanFarhanNo ratings yet
- Delayed Interval Delivery in Twin Pregnancy Without Cerclage: CaseDocument2 pagesDelayed Interval Delivery in Twin Pregnancy Without Cerclage: Caselailatul husnaNo ratings yet
- BJSTR MS Id 003341Document4 pagesBJSTR MS Id 003341herryNo ratings yet
- Girija BS, Sudha TR: AbstractDocument4 pagesGirija BS, Sudha TR: AbstractALfuNo ratings yet
- Gynecology and Minimally Invasive Therapy: Shahul Hameed Mohamed Siraj, Bernard Su Min ChernDocument3 pagesGynecology and Minimally Invasive Therapy: Shahul Hameed Mohamed Siraj, Bernard Su Min ChernIrvin MarcelNo ratings yet
- Conservative Management of Placenta Accreta in A Multiparous WomanDocument10 pagesConservative Management of Placenta Accreta in A Multiparous WomanRobel Mae Lagos MontañoNo ratings yet
- Adenomyosis and Uterine Rupture During Labour in A Primigravida: An Unusual Obstetric Emergency in NigeriaDocument2 pagesAdenomyosis and Uterine Rupture During Labour in A Primigravida: An Unusual Obstetric Emergency in NigeriaMariam Carolina Viloria VargasNo ratings yet
- AkretaDocument7 pagesAkretaInna SeraLaratNo ratings yet
- A Rare Case of Puerperal Uterine Inversion and Literature ReviewDocument3 pagesA Rare Case of Puerperal Uterine Inversion and Literature ReviewIJAR JOURNALNo ratings yet
- Case Report Large Uterine Fibroids in Pregnancy With Successful Caesarean MyomectomyDocument4 pagesCase Report Large Uterine Fibroids in Pregnancy With Successful Caesarean MyomectomyChidimma VictoryNo ratings yet
- Poster T1BDocument1 pagePoster T1BHaris SetiaNo ratings yet
- Lactating Adenoma A Case ReportDocument3 pagesLactating Adenoma A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Kista Terpluntir NcbiDocument2 pagesKista Terpluntir NcbiFatimahNo ratings yet
- Rupture of The Cervix During Pregnancy After Cervical Pessary Insertion For Preventing Preterm BirthDocument4 pagesRupture of The Cervix During Pregnancy After Cervical Pessary Insertion For Preventing Preterm BirthNuril AzizahNo ratings yet
- 1 s2.0 S0090825804003610 Main PDFDocument3 pages1 s2.0 S0090825804003610 Main PDFRirin WahyuniNo ratings yet
- Katakam2009 PDFDocument1 pageKatakam2009 PDFandri anaNo ratings yet
- Case Report: Management of Cervical Fibroid During The Reproductive PeriodDocument4 pagesCase Report: Management of Cervical Fibroid During The Reproductive PeriodMetharisaNo ratings yet
- Adenomyosis Excision Followed by Successful Live Birth After Three Consecutive IVFDocument5 pagesAdenomyosis Excision Followed by Successful Live Birth After Three Consecutive IVFPyuzz RemakeNo ratings yet
- Case Report Rare Cesarean Section Scar Ectopic Pregnancy Successfully Treated by Methotrexate: A CaseDocument5 pagesCase Report Rare Cesarean Section Scar Ectopic Pregnancy Successfully Treated by Methotrexate: A Casemustafaali9711No ratings yet
- Medical Treatment of Tubar Ectopic Pregnancy With Living EmbrioDocument4 pagesMedical Treatment of Tubar Ectopic Pregnancy With Living EmbrioMuhammad Aji SantosoNo ratings yet
- Yan 2007Document3 pagesYan 2007Agustin LindaNo ratings yet
- Third Trimester Fetoscopic Laser Ablation of Type II Vasa PreviaDocument5 pagesThird Trimester Fetoscopic Laser Ablation of Type II Vasa PreviaSol MancipeNo ratings yet
- Clinical Medicine Insights: Case ReportsDocument4 pagesClinical Medicine Insights: Case ReportsJer KelNo ratings yet
- Gynecologic Oncology Reports: Natsuki Tsuji, Yusuke Butsuhara, Hiroko Yoshikawa, Koichi Terakawa, Tadayoshi NaganoDocument3 pagesGynecologic Oncology Reports: Natsuki Tsuji, Yusuke Butsuhara, Hiroko Yoshikawa, Koichi Terakawa, Tadayoshi NaganofujimeisterNo ratings yet
- Labor Epidural Analgesia With Severe ThrombocytopeniaDocument2 pagesLabor Epidural Analgesia With Severe Thrombocytopeniasand52525No ratings yet
- Hioerplasia Mamaria GestacionalDocument9 pagesHioerplasia Mamaria GestacionalOctavio LeyvaNo ratings yet
- Wright 2013Document3 pagesWright 2013cristian vivasNo ratings yet
- 1 s2.0 S1028455922002935 MainDocument4 pages1 s2.0 S1028455922002935 Mainmodacasper056No ratings yet
- Liao 2016Document4 pagesLiao 2016cristian vivasNo ratings yet
- Hysteroscopic Management of Omentum Incarceration (Ingles)Document6 pagesHysteroscopic Management of Omentum Incarceration (Ingles)silviadmcastellanNo ratings yet
- A Rare Case of Morbidly Adherent Placenta in A Young - 2024 - International JouDocument4 pagesA Rare Case of Morbidly Adherent Placenta in A Young - 2024 - International JouRonald QuezadaNo ratings yet
- Emergency Peripartum Hysterectomy As Life Saving Surgery For Postpartum Haemorrhage in Women With Single Kidney - A CaseReportDocument5 pagesEmergency Peripartum Hysterectomy As Life Saving Surgery For Postpartum Haemorrhage in Women With Single Kidney - A CaseReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Case Report: Postpartum Uterine Wound Dehiscence Leading To Secondary PPH: Unusual SequelaeDocument4 pagesCase Report: Postpartum Uterine Wound Dehiscence Leading To Secondary PPH: Unusual SequelaemelisaberlianNo ratings yet
- Torsion OvarianDocument6 pagesTorsion Ovarianrg2fpgqnc8No ratings yet
- A New Facilitating Technique For Postpartum Hysterectomy at Full Dilatation: Cervical ClampDocument4 pagesA New Facilitating Technique For Postpartum Hysterectomy at Full Dilatation: Cervical ClampJani SheNo ratings yet
- Uncomplicated Term Vaginal Delivery Following Magnetic Resonance-Guided Focused Ultrasound Surgery For Uterine FibroidsDocument4 pagesUncomplicated Term Vaginal Delivery Following Magnetic Resonance-Guided Focused Ultrasound Surgery For Uterine FibroidsMangku Liong GuanNo ratings yet
- Gynecology and Minimally Invasive Therapy: Case ReportDocument5 pagesGynecology and Minimally Invasive Therapy: Case Reportsexit47234No ratings yet
- PSC Unit 3Document18 pagesPSC Unit 3Santosh ReddyNo ratings yet
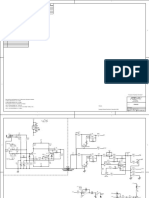
- Peavey Xr8000 SCHDocument12 pagesPeavey Xr8000 SCHLisandro Orrego SalvadorNo ratings yet
- Bending Stresses in BeamsDocument25 pagesBending Stresses in Beamsrajatapc12007No ratings yet
- Quantitative Interpretation of The Response of Surface Plasmon Resonance Sensors To Adsorbed FilmsDocument13 pagesQuantitative Interpretation of The Response of Surface Plasmon Resonance Sensors To Adsorbed FilmsKaren Régules MedelNo ratings yet
- Abstracts: IAFRI Metaldehyde Conference - 13 September - Fera Science LTD, York YO41 1LZDocument6 pagesAbstracts: IAFRI Metaldehyde Conference - 13 September - Fera Science LTD, York YO41 1LZbendel_boyNo ratings yet
- Euca FBB - Jiangxi MillDocument1 pageEuca FBB - Jiangxi MillBill King0% (1)
- Full Download Strategies For Teaching Learners With Special Needs 11th Edition Polloway Test BankDocument36 pagesFull Download Strategies For Teaching Learners With Special Needs 11th Edition Polloway Test Banklevidelpnrr100% (30)
- Total Result 2594 Total Result 2583Document2,897 pagesTotal Result 2594 Total Result 2583anjali shilpa kajalNo ratings yet
- Valorisation of Spent Coffee Grounds Production of Biodiesel Via Enzimatic Catalisis With Ethanol and Co-SolventDocument14 pagesValorisation of Spent Coffee Grounds Production of Biodiesel Via Enzimatic Catalisis With Ethanol and Co-SolventAline GonçalvesNo ratings yet
- Up ListDocument200 pagesUp Listprashant guptaNo ratings yet
- BIOL207 Open GeneticsDocument182 pagesBIOL207 Open GeneticsBi Anh100% (1)
- Module 2 (People and The Earth's Ecosystem)Document11 pagesModule 2 (People and The Earth's Ecosystem)chris ian0% (2)
- 5th Fancy BreadDocument7 pages5th Fancy BreadMera Funportal0% (1)
- CBSE Class 10 Revision WorksheetDocument13 pagesCBSE Class 10 Revision WorksheetEdward DevisNo ratings yet
- Samsung Galaxy S22 Ultra 5G - Full Phone SpecificationsDocument13 pagesSamsung Galaxy S22 Ultra 5G - Full Phone SpecificationsAb BossNo ratings yet
- CPS - Data Intensive Distributed ComputingDocument11 pagesCPS - Data Intensive Distributed ComputingManoj KavediaNo ratings yet
- Basic Monte Carlo TechniquesDocument10 pagesBasic Monte Carlo TechniquesMobeen AhmadNo ratings yet
- STRUCTURE Magazine - Condition Assessment of Old Stone Retaining Walls PDFDocument8 pagesSTRUCTURE Magazine - Condition Assessment of Old Stone Retaining Walls PDFShabbir LokhandwalaNo ratings yet
- Digsi4 DisplayDocument81 pagesDigsi4 Displaymohammed youisfNo ratings yet
- General Twin Seal 06Document24 pagesGeneral Twin Seal 06Gk GaneshNo ratings yet
- Class 9 - ScienceDocument228 pagesClass 9 - ScienceYashwanth KasturiNo ratings yet
- Global Stability Analysis of Eccentric Taylor Couette FlowDocument28 pagesGlobal Stability Analysis of Eccentric Taylor Couette FlowSreekanth MenonNo ratings yet
- Soal Latihan US Bahasa InggrisDocument5 pagesSoal Latihan US Bahasa Inggrispikri18120No ratings yet
- PPM Schedule Anmol Feeds PVT LTD - PanchlaDocument1 pagePPM Schedule Anmol Feeds PVT LTD - PanchlaSatyajit DasNo ratings yet
- BusDocument24 pagesBusSyed Noman AhmedNo ratings yet
- Cryolite JM File 2011Document5 pagesCryolite JM File 2011mutemuNo ratings yet
- Cancer and Its Easy Treatment in Homeopathy - Bashir Mahmud ElliasDocument5 pagesCancer and Its Easy Treatment in Homeopathy - Bashir Mahmud ElliasBashir Mahmud ElliasNo ratings yet
- Raychem Molded PartsDocument28 pagesRaychem Molded PartsAMNo ratings yet