Download as pdf or txt
You might also like
- Madras Miscellany - The Father of Indian Botany - The HinduDocument4 pagesMadras Miscellany - The Father of Indian Botany - The Hindujoseph xavierNo ratings yet
- Fast Facts: CAR T-Cell Therapy in Diffuse Large B-Cell Lymphoma: A practical resource for nursesFrom EverandFast Facts: CAR T-Cell Therapy in Diffuse Large B-Cell Lymphoma: A practical resource for nursesNo ratings yet
- Ascp PointersDocument78 pagesAscp Pointersbaihern2467% (3)
- SIP5 7KE85 V07.80 Manual C018-6 en PDFDocument502 pagesSIP5 7KE85 V07.80 Manual C018-6 en PDFDoan Anh TuanNo ratings yet
- Renal Transplantation Into High Risk, Highly Sensitized Recipients: A Single Center ExperienceDocument44 pagesRenal Transplantation Into High Risk, Highly Sensitized Recipients: A Single Center ExperienceDwiyanti OktaviaNo ratings yet
- CCO Hematology 2020 4Document16 pagesCCO Hematology 2020 4amibabymbahNo ratings yet
- GVHD GVLDocument44 pagesGVHD GVLLuanaJBCNo ratings yet
- Digital PCR - A Sensitive and Precise Method For KIT D816V Quantification in MastocytosisDocument9 pagesDigital PCR - A Sensitive and Precise Method For KIT D816V Quantification in MastocytosisMagan AliNo ratings yet
- Blood TransfusionDocument36 pagesBlood TransfusionpedsoncoaiimsNo ratings yet
- TMP E572Document6 pagesTMP E572FrontiersNo ratings yet
- Keertan Dheda (3) TB Test PDFDocument48 pagesKeertan Dheda (3) TB Test PDFphuong mai leNo ratings yet
- 1 - Hodgkin's LymphomaDocument12 pages1 - Hodgkin's LymphomaDiana MitreaNo ratings yet
- Marrow Transplanted Patients Inhibits Cell-Mediated Cytolysis A Soluble Factor Released by CD8+CD57+ Lymphocytes From BoneDocument6 pagesMarrow Transplanted Patients Inhibits Cell-Mediated Cytolysis A Soluble Factor Released by CD8+CD57+ Lymphocytes From Bonecyahayue5554No ratings yet
- Crossmatch VarianteDocument5 pagesCrossmatch VarianteAlex StefanNo ratings yet
- Non-Hodgkin Lymphoma and Hodgkin's Disease: From The Transplantation's Point of ViewDocument46 pagesNon-Hodgkin Lymphoma and Hodgkin's Disease: From The Transplantation's Point of ViewFikri HariqiNo ratings yet
- Acute Rejection DR Sihir GangDocument38 pagesAcute Rejection DR Sihir GangwandaNo ratings yet
- Serology Testing 101: The BasicsDocument49 pagesSerology Testing 101: The Basicsdjf412No ratings yet
- Targeted Therapies in Hematology & Oncology: Mark B Juckett MD Section of Hematology/BMT University of WisconsinDocument61 pagesTargeted Therapies in Hematology & Oncology: Mark B Juckett MD Section of Hematology/BMT University of WisconsinihdaNo ratings yet
- Understanding Multiple Myeloma and Laboratory ValuesDocument25 pagesUnderstanding Multiple Myeloma and Laboratory ValuesMeena Tiwari100% (1)
- If HP Cancer Guide BMT ManualDocument363 pagesIf HP Cancer Guide BMT ManualZardar KNo ratings yet
- Il28b 2015Document7 pagesIl28b 2015Hafsa AzizNo ratings yet
- AW Diag Treat AR FinalDocument28 pagesAW Diag Treat AR FinalAnna DangNo ratings yet
- Therapy Tested Marker Predicted Response: Imatinib Sunitinib RegorafenibDocument11 pagesTherapy Tested Marker Predicted Response: Imatinib Sunitinib RegorafenibArif MehmoodNo ratings yet
- HepatomaDocument33 pagesHepatomaRozen RyuhaNo ratings yet
- Rev-Inhibitor Manado 2017Document37 pagesRev-Inhibitor Manado 2017Utari UbNo ratings yet
- 5image BBDocument44 pages5image BBCaleb Joshua MendozaNo ratings yet
- MGH Housestaff Manual 2023-2024 Page 146Document1 pageMGH Housestaff Manual 2023-2024 Page 146sr652dmx9tNo ratings yet
- Overview of Blood and Marrow TransplantationDocument45 pagesOverview of Blood and Marrow TransplantationManasa ChandruNo ratings yet
- A Longitudinal Study of Convalescent Plasma (CCP) DonorsDocument14 pagesA Longitudinal Study of Convalescent Plasma (CCP) DonorsANANo ratings yet
- Prezentare DFPP Chișinău 2018Document41 pagesPrezentare DFPP Chișinău 2018Mihai SavaNo ratings yet
- NIHMS13776 Supplement SuppDocument7 pagesNIHMS13776 Supplement Suppmaxence tricaudNo ratings yet
- AphmDocument46 pagesAphmapi-3750327No ratings yet
- Guidelines For Compatibility Procedures in Blood Transfusion LaboratoriesDocument16 pagesGuidelines For Compatibility Procedures in Blood Transfusion LaboratoriesErika SantiagoNo ratings yet
- A 1Document5 pagesA 1cikobernicaNo ratings yet
- Hepatitis B Case StudiesDocument26 pagesHepatitis B Case StudieswqmxmNo ratings yet
- Ijbsv 18 P 3470 S 1Document15 pagesIjbsv 18 P 3470 S 1李秀赫No ratings yet
- Kanaoka 1999Document6 pagesKanaoka 1999awdafeagega2r3No ratings yet
- Macrogenics-Identification of UnknownTarget Antigens Using Phynexus Technology-8099Document19 pagesMacrogenics-Identification of UnknownTarget Antigens Using Phynexus Technology-8099박지홍No ratings yet
- Improving Cytomegalovirus-Specific T Cell Reconstitution After Haploidentical Stem Cell TransplantationDocument13 pagesImproving Cytomegalovirus-Specific T Cell Reconstitution After Haploidentical Stem Cell TransplantationyaniraNo ratings yet
- Preclinical Development and Evaluation of Nanobody-Based CD70-specific CAR T Cells For The Treatment of Acute Myeloid LeukemiaDocument16 pagesPreclinical Development and Evaluation of Nanobody-Based CD70-specific CAR T Cells For The Treatment of Acute Myeloid LeukemiaMilan JovicNo ratings yet
- 2017 HepatologyDocument148 pages2017 HepatologyrdLuis1No ratings yet
- Analysis of Hepatitis in Murine Herpesvirus 68-Infected Mice Used As Epstein-Barr Virus Hepatitis ModelDocument9 pagesAnalysis of Hepatitis in Murine Herpesvirus 68-Infected Mice Used As Epstein-Barr Virus Hepatitis ModelRahmiati LaoNo ratings yet
- Journal Reading Nasopharyngeal Carcinoma: Current Treatment Options and Future DirectionsDocument28 pagesJournal Reading Nasopharyngeal Carcinoma: Current Treatment Options and Future DirectionsyuliNo ratings yet
- Epigenetics (Nilofer Saba Azad, M.D.)Document40 pagesEpigenetics (Nilofer Saba Azad, M.D.)National Press Foundation100% (2)
- Screening For Viral Hepatitis: Diagnostics (HBV and HCV) : Diana HardieDocument23 pagesScreening For Viral Hepatitis: Diagnostics (HBV and HCV) : Diana HardieWahyu PurnamaNo ratings yet
- Transfusion SupportDocument7 pagesTransfusion Supportparag fNo ratings yet
- Okamoto 1999Document7 pagesOkamoto 1999Araceli Enríquez OvandoNo ratings yet
- GVHDDocument35 pagesGVHDSaad KhanNo ratings yet
- Vidas HCV March 2012Document31 pagesVidas HCV March 2012Rao ImranNo ratings yet
- Cross-Match-Compatible Platelets Improve CorrectedDocument7 pagesCross-Match-Compatible Platelets Improve CorrectedKatherinne Alexandra Escárraga CorrealNo ratings yet
- Detection of Anti-Platelet Antibodies in Immune ThrombocytopeniaaaaaaaDocument4 pagesDetection of Anti-Platelet Antibodies in Immune ThrombocytopeniaaaaaaaKatherinne Alexandra Escárraga CorrealNo ratings yet
- Jurnal jvh.13489Document7 pagesJurnal jvh.13489Ei DrakorNo ratings yet
- 05 RosenbergDocument128 pages05 RosenbergEnrique GuerreroNo ratings yet
- The Role of Post-RT FDG PET in Neck Dissection For Regionally Advanced Head and Neck Cancer (PDFDrive)Document165 pagesThe Role of Post-RT FDG PET in Neck Dissection For Regionally Advanced Head and Neck Cancer (PDFDrive)Bianca DanielaNo ratings yet
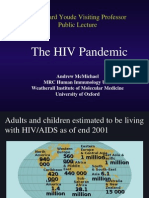
- The HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureDocument50 pagesThe HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureSanthosh SubramanianNo ratings yet
- CCO 2020 WCLC Downloadable 1Document106 pagesCCO 2020 WCLC Downloadable 1Florencia GuerraNo ratings yet
- HIV - ART Revisited 2024 Med - Guidelines - SPDocument50 pagesHIV - ART Revisited 2024 Med - Guidelines - SPdr.htetaung2017No ratings yet
- CD4 Easy Count Kit: Product Name Code No. ContentDocument2 pagesCD4 Easy Count Kit: Product Name Code No. ContentDinesh SreedharanNo ratings yet
- Bethesda Handbook of HematologyDocument5 pagesBethesda Handbook of HematologyjosephNo ratings yet
- Gene Xpert Ultra JC Sayan FinalDocument40 pagesGene Xpert Ultra JC Sayan FinalmeghaNo ratings yet
- Annrheumdis 2017 March 76 3 566 Inline Supplementary Material 1 PDFDocument20 pagesAnnrheumdis 2017 March 76 3 566 Inline Supplementary Material 1 PDFniajaplaniNo ratings yet
- Cancer Gene Therapy by Viral and Non-viral VectorsFrom EverandCancer Gene Therapy by Viral and Non-viral VectorsMalcolm BrennerNo ratings yet
- B-Housing and Living - 1Document2 pagesB-Housing and Living - 1Štěpánka OndrůškováNo ratings yet
- CitoVac EnglishDocument32 pagesCitoVac EnglishJulio C. Sierra PalominoNo ratings yet
- Payable Salary Paid SalaryDocument2 pagesPayable Salary Paid SalaryAhmed AmmanNo ratings yet
- Maryland Route 214 - WikipediaDocument9 pagesMaryland Route 214 - WikipediadwrreNo ratings yet
- Course Title:-Advanced Computer Networking Group Presentation On NFV FunctionalityDocument18 pagesCourse Title:-Advanced Computer Networking Group Presentation On NFV FunctionalityRoha CbcNo ratings yet
- MATH 5 Q4 Module 2 Vizualizing Volume of Cube and Rectangular PrismDocument21 pagesMATH 5 Q4 Module 2 Vizualizing Volume of Cube and Rectangular PrismAnj De Guzman75% (4)
- Entrep 1st PerioDocument5 pagesEntrep 1st PerioMargarette FajardoNo ratings yet
- Siskyou Bombing RangeDocument114 pagesSiskyou Bombing RangeCAP History LibraryNo ratings yet
- Saturn Quad QSDSSDocument1 pageSaturn Quad QSDSSniall.godleyNo ratings yet
- Introduction To Ipgcl & PPCLDocument31 pagesIntroduction To Ipgcl & PPCLSahil SethiNo ratings yet
- TLE 8 - Handicraft Production Lesson 2: Elements of Design: Information SectionDocument9 pagesTLE 8 - Handicraft Production Lesson 2: Elements of Design: Information SectionMarist ChefNo ratings yet
- Computational Methods: Test Program For Chasing Method Developed in MatlabDocument6 pagesComputational Methods: Test Program For Chasing Method Developed in MatlabMujtaba MujahidNo ratings yet
- L-s20 Specification For Road Lighting InstallationDocument82 pagesL-s20 Specification For Road Lighting Installationzamanhuri junidNo ratings yet
- Fan Basics and Selection CriteriaDocument6 pagesFan Basics and Selection CriteriaSangamesh WaranNo ratings yet
- أساسيات الاتصالات الرقمية PDFDocument230 pagesأساسيات الاتصالات الرقمية PDFAbdulssalam Mohammed Hussein Khako StudentNo ratings yet
- 19 Fingal Development Plan 2017-2023 - Strategic Environmental Assessment Statement PDFDocument110 pages19 Fingal Development Plan 2017-2023 - Strategic Environmental Assessment Statement PDFdi TalapaniniNo ratings yet
- A Review On Rasamanjari: It's Contribution in Pharmaceutical ScienceDocument3 pagesA Review On Rasamanjari: It's Contribution in Pharmaceutical ScienceEditor IJTSRDNo ratings yet
- Vanilla Icebox CookiesDocument2 pagesVanilla Icebox CookiesmadduxdavidNo ratings yet
- Tabletop Gaming - Best Games of 2019Document198 pagesTabletop Gaming - Best Games of 2019Paulina Barszez100% (1)
- Logg 4000Document7 pagesLogg 4000Stjepan FrljicNo ratings yet
- Firearms in America 1600 - 1899Document310 pagesFirearms in America 1600 - 1899Mike100% (3)
- Beyond The Brain - Text 1Document5 pagesBeyond The Brain - Text 1ivona0mati0No ratings yet
- (M. J. Edwards) The ''Epistle To Rheginus'' ValenDocument17 pages(M. J. Edwards) The ''Epistle To Rheginus'' ValenGlebMatveevNo ratings yet
- Growth and DevelopmentDocument57 pagesGrowth and DevelopmentKelvin kipkuruiNo ratings yet
- Chap 11Document3 pagesChap 11Flia Diaz ZunigaNo ratings yet
- Technological Institute of The Philippines-ManilaDocument17 pagesTechnological Institute of The Philippines-ManilaRoscarl GorospeNo ratings yet
- 11thMachAutoExpo 2022Document112 pages11thMachAutoExpo 2022Priyanka KadamNo ratings yet
- '21.8월 논문게재 윤인복Document10 pages'21.8월 논문게재 윤인복윤인복No ratings yet