Download as pdf or txt
You might also like
- C Shape PDFDocument6 pagesC Shape PDFTrang VõNo ratings yet
- Management of C Shaped Canals: A Case Series: IOSR Journal of Dental and Medical Sciences March 2021Document7 pagesManagement of C Shaped Canals: A Case Series: IOSR Journal of Dental and Medical Sciences March 2021Prathiksha ShettyNo ratings yet
- Case Report A Rare Case of Single-Rooted Mandibular Second Molar With Single CanalDocument6 pagesCase Report A Rare Case of Single-Rooted Mandibular Second Molar With Single CanalKarissa NavitaNo ratings yet
- Management of C Shaped CanalsDocument4 pagesManagement of C Shaped CanalsJot KhalsaNo ratings yet
- Peters2004 PDFDocument9 pagesPeters2004 PDFNunoGonçalvesNo ratings yet
- Journal of Endodontics 2013 Ball - Henrik - Skjerven - 11!06!2013Document10 pagesJournal of Endodontics 2013 Ball - Henrik - Skjerven - 11!06!2013Marilyn GonzalesNo ratings yet
- Fan2008 PDFDocument6 pagesFan2008 PDFMarco CastroNo ratings yet
- Case Report: Management of Six Root Canals in Mandibular First MolarDocument6 pagesCase Report: Management of Six Root Canals in Mandibular First MolarArida Khoiruza Asy'ariNo ratings yet
- Influence of Contracted Endodontic Access On Root Canal Geometry An in Vitro StudyDocument7 pagesInfluence of Contracted Endodontic Access On Root Canal Geometry An in Vitro StudyLina SaadNo ratings yet
- Accidents in Endodontic A Case ReportDocument4 pagesAccidents in Endodontic A Case ReportDr.O.R.GANESAMURTHINo ratings yet
- Antonis Chaniotis Doble CurvaturaDocument8 pagesAntonis Chaniotis Doble CurvaturaVitall Dent Endodoncia Odontologia integralNo ratings yet
- Analysis of C-Shaped Canals by Panoramic Radiography and Cone-Beam Computed Tomography - Root-Type Specificity by Longitudinal DistributionDocument5 pagesAnalysis of C-Shaped Canals by Panoramic Radiography and Cone-Beam Computed Tomography - Root-Type Specificity by Longitudinal DistributionAnthony LiNo ratings yet
- 3 OK Iej-12-502Document6 pages3 OK Iej-12-502Ryanka Dizayani PutraNo ratings yet
- A Micro CT Study of The Mesiobuccal Root Canal Morphology of The Maxillary First Molar ToothDocument8 pagesA Micro CT Study of The Mesiobuccal Root Canal Morphology of The Maxillary First Molar ToothGisela De Souza PereiraNo ratings yet
- A C-Shaped Canal in A Maxillary Second Molar: Prexion 3D Cone-Beam Computed Tomography AnalysisDocument5 pagesA C-Shaped Canal in A Maxillary Second Molar: Prexion 3D Cone-Beam Computed Tomography AnalysisPuscas IulianaNo ratings yet
- Endodontic Managment of Curved CanalDocument3 pagesEndodontic Managment of Curved Canalfun timesNo ratings yet
- BIO C Repair With For Horizontal Root Fracture PDFDocument5 pagesBIO C Repair With For Horizontal Root Fracture PDFDaniel Vivas0% (1)
- Jurnal KasusDocument4 pagesJurnal KasusDena SeptianiNo ratings yet
- Endodontic Treatment of Curved Root Canal SystemsDocument8 pagesEndodontic Treatment of Curved Root Canal SystemsRoxana BotNo ratings yet
- Management of C Shaped Canals - A Case SeriesDocument6 pagesManagement of C Shaped Canals - A Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of The Cause of Failure in Nonsurgical Endodontic Tretament by Microscopic Inspection During Endodontic MicrosurgeryDocument4 pagesAnalysis of The Cause of Failure in Nonsurgical Endodontic Tretament by Microscopic Inspection During Endodontic MicrosurgeryAdeneusa Coelho100% (1)
- 2022 AiutoDocument7 pages2022 AiutovivianaNo ratings yet
- Root-End Resection With or Without Retrograde Obturation After Orthograde Filling With Two Techniques: A Micro - CT StudyDocument8 pagesRoot-End Resection With or Without Retrograde Obturation After Orthograde Filling With Two Techniques: A Micro - CT StudyAndrés Castillo ChacónNo ratings yet
- 10.1007@s11282 020 00486 3Document8 pages10.1007@s11282 020 00486 3Andhi DavidNo ratings yet
- The Internal Root Canal Morphology of Single Rooted Mandibular Canines Revealed by Micro ComputedDocument4 pagesThe Internal Root Canal Morphology of Single Rooted Mandibular Canines Revealed by Micro Computedimran khanNo ratings yet
- C-Shaped Canals by Panoramic RadiographyDocument5 pagesC-Shaped Canals by Panoramic RadiographyAkriti GoelNo ratings yet
- !!! Root Canal Morphology and It's Relationship To Endodontic Procedures - Frank J. Vertucci !!!Document27 pages!!! Root Canal Morphology and It's Relationship To Endodontic Procedures - Frank J. Vertucci !!!Puscas Madalina100% (1)
- C Shaped Root Canals in Mandibular Second Molars in A SaudiDocument6 pagesC Shaped Root Canals in Mandibular Second Molars in A SaudiFatima SiddiquiNo ratings yet
- 3d C ShapedDocument4 pages3d C ShapedCarlos San MartinNo ratings yet
- Art EndoDocument6 pagesArt EndoVANESSA ALVITRESNo ratings yet
- Canal Configuration in The Mesiobuccal Root of The Maxillary First Molar and Its Endodontic SignificanceDocument7 pagesCanal Configuration in The Mesiobuccal Root of The Maxillary First Molar and Its Endodontic Significanceshamshuddin patelNo ratings yet
- Oke 4Document3 pagesOke 4Maika RatriNo ratings yet
- Jzusb15 1064Document8 pagesJzusb15 1064Irfan Cahya PermanaNo ratings yet
- Identification and Endodontic Management of Confluent Middle Mesial Canal in Mandibular First Molar A Case Report.20150306124240Document4 pagesIdentification and Endodontic Management of Confluent Middle Mesial Canal in Mandibular First Molar A Case Report.20150306124240dini anitaNo ratings yet
- A Micro-Computed Tomography Study of The Root Canal Morphology of The Mandibular First Premolar in A Population From Southwestern ChinaDocument10 pagesA Micro-Computed Tomography Study of The Root Canal Morphology of The Mandibular First Premolar in A Population From Southwestern ChinaNissaNo ratings yet
- Barreto 2012Document5 pagesBarreto 2012Claudia PerezNo ratings yet
- Digital Imaging in Trauma Part 2Document9 pagesDigital Imaging in Trauma Part 2Gaurav BasuNo ratings yet
- Repair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingDocument8 pagesRepair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingAhmad Ulil AlbabNo ratings yet
- Management of C Shaped Canals: 3 Case ReportsDocument3 pagesManagement of C Shaped Canals: 3 Case ReportsTaufiqurrahman Abdul Djabbar100% (1)
- Anatomical Variations and Various Techniques of Identification of Multiple Root Canals: A ReviewDocument5 pagesAnatomical Variations and Various Techniques of Identification of Multiple Root Canals: A ReviewIJAR JOURNALNo ratings yet
- Oral Surg Oral Med Oral Pathol Oral Radiol. 2012 - 113 2 260-7Document8 pagesOral Surg Oral Med Oral Pathol Oral Radiol. 2012 - 113 2 260-7Michelle GrynbergNo ratings yet
- Perawatan Saluran AkarDocument19 pagesPerawatan Saluran AkarBunga Erlita RosaliaNo ratings yet
- Chapter 7 Tooth Morphology and Access Cavity PreparationDocument232 pagesChapter 7 Tooth Morphology and Access Cavity Preparationusmanhameed8467% (3)
- Bodily Distalization of Molars With Absolute AnchorageDocument12 pagesBodily Distalization of Molars With Absolute AnchorageAnamika AttrishiNo ratings yet
- Root Canal Treatment of The Maxillary Second Molar With An Unusual MorphologyDocument8 pagesRoot Canal Treatment of The Maxillary Second Molar With An Unusual MorphologymarcelNo ratings yet
- Applied Sciences: Plywood Jig-A New Technique For Root Canal Curvature MeasurementDocument8 pagesApplied Sciences: Plywood Jig-A New Technique For Root Canal Curvature MeasurementKarissa NavitaNo ratings yet
- A Central Incisor With 4 Independent Root CanalsDocument4 pagesA Central Incisor With 4 Independent Root CanalsKiki Qurrotul Ayuni IINo ratings yet
- Art Yogesh SirDocument5 pagesArt Yogesh SirRuchi ShahNo ratings yet
- Management of Mandibular Canine With Two Roots and Two Root Canals: A Case ReportDocument4 pagesManagement of Mandibular Canine With Two Roots and Two Root Canals: A Case ReportUnlikely QuestionsNo ratings yet
- Prosthodontic Management of Dentate Maxillectomy Patient A Clinical Case ReportActa Marisiensis Seria MedicaDocument4 pagesProsthodontic Management of Dentate Maxillectomy Patient A Clinical Case ReportActa Marisiensis Seria MedicaSaniaNo ratings yet
- Rehability AssessmentsDocument8 pagesRehability AssessmentsDarianNo ratings yet
- Effect of Different CAD-CAM Materials On The Marginal and Internal Adaptation of Endocrown Restorations: An in Vitro StudyDocument7 pagesEffect of Different CAD-CAM Materials On The Marginal and Internal Adaptation of Endocrown Restorations: An in Vitro StudyNetra TaleleNo ratings yet
- Multidisciplinary Approach For The Treatment of Horizontal Root-Fractured Maxillary Anterior TeethDocument11 pagesMultidisciplinary Approach For The Treatment of Horizontal Root-Fractured Maxillary Anterior TeethGülbike DemirelNo ratings yet
- Three Root Canals in The Mesiobuccal Root of Maxillary Molars: Case Reports and Literature ReviewDocument8 pagesThree Root Canals in The Mesiobuccal Root of Maxillary Molars: Case Reports and Literature ReviewJing XueNo ratings yet
- Current Therapy in EndodonticsFrom EverandCurrent Therapy in EndodonticsPriyanka JainNo ratings yet
- Diagnosis and Treatment of Furcation-Involved TeethFrom EverandDiagnosis and Treatment of Furcation-Involved TeethLuigi NibaliNo ratings yet
- Minimally Invasive Periodontal Therapy: Clinical Techniques and Visualization TechnologyFrom EverandMinimally Invasive Periodontal Therapy: Clinical Techniques and Visualization TechnologyNo ratings yet
- Clinical Maxillary Sinus Elevation SurgeryFrom EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoNo ratings yet
- Fundamentals of Oral and Maxillofacial RadiologyFrom EverandFundamentals of Oral and Maxillofacial RadiologyRating: 4 out of 5 stars4/5 (1)
- Interceptive Orthodontics: A Practical Guide to Occlusal ManagementFrom EverandInterceptive Orthodontics: A Practical Guide to Occlusal ManagementNo ratings yet
- Week1 CombineDocument91 pagesWeek1 CombineraleyNo ratings yet
- Activity 6Document4 pagesActivity 6Junior SmithNo ratings yet
- License Plate RecognitionDocument3 pagesLicense Plate RecognitionSen PaiiNo ratings yet
- The Cost of Goods Sold For The Month of December: Excel Professional Services, IncDocument4 pagesThe Cost of Goods Sold For The Month of December: Excel Professional Services, IncmatildaNo ratings yet
- 1h 2019 Assessment1Document72 pages1h 2019 Assessment1api-406108641No ratings yet
- A VFP-SQL Server Application From The BeginingDocument38 pagesA VFP-SQL Server Application From The Beginingmohsin.computers3076No ratings yet
- Straight Line Equation of A Straight Line 3x - 4y 7: Answer All Questions. For Examiner' S UseDocument22 pagesStraight Line Equation of A Straight Line 3x - 4y 7: Answer All Questions. For Examiner' S UseDavinAvalaniNo ratings yet
- Kine 2p90 l19Document9 pagesKine 2p90 l19baileyschaefer28No ratings yet
- Ricky C. Alfon: - Individual Differences - (Prof Ed 6) Facilitating Learner-Centered TeachingDocument8 pagesRicky C. Alfon: - Individual Differences - (Prof Ed 6) Facilitating Learner-Centered TeachingMark Joseph DacubaNo ratings yet
- Car Sticker Policy PDFDocument11 pagesCar Sticker Policy PDFMohsin KhanNo ratings yet
- Zosi Wireless NVR & Monitor SystemDocument60 pagesZosi Wireless NVR & Monitor SystemJose RamirezNo ratings yet
- CCBoot Manual - Server SettingsDocument89 pagesCCBoot Manual - Server SettingsHasnan IbrahimNo ratings yet
- Plagiarism Prevention Software: TurnitinDocument24 pagesPlagiarism Prevention Software: TurnitinJoshua QuayeNo ratings yet
- Chapter 4 - Braking System 4.1 Brake LinesDocument14 pagesChapter 4 - Braking System 4.1 Brake LinesEmanuel VidalNo ratings yet
- ISO 2597-2 - 2019 - Iron Ores Determination of Total Iron Content - Part 2 Titrimetric Methods After Titanium (III) Chloride ReductionDocument20 pagesISO 2597-2 - 2019 - Iron Ores Determination of Total Iron Content - Part 2 Titrimetric Methods After Titanium (III) Chloride ReductionMetal deptNo ratings yet
- AP 5902 Liability Supporting NotesDocument6 pagesAP 5902 Liability Supporting NotesMeojh Imissu100% (1)
- Chapter No. 25 Maintenance of Canals & DrainsDocument4 pagesChapter No. 25 Maintenance of Canals & DrainsMANJEET SINGHNo ratings yet
- Brochure Leaching 4824 01 23 en MNGDocument8 pagesBrochure Leaching 4824 01 23 en MNGOsamaNo ratings yet
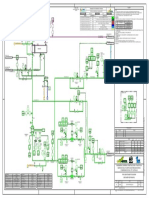
- HE-210 P-2604A-B - DEBUTANIZER FEED PREHEATING - Rev 0CxDocument1 pageHE-210 P-2604A-B - DEBUTANIZER FEED PREHEATING - Rev 0CxMariaNo ratings yet
- CNotice LogDocument15 pagesCNotice LogAzertyuioptotoNo ratings yet
- Sepharial - The Science of Foreknowledge Cd13 Id 1928069166 Size603Document114 pagesSepharial - The Science of Foreknowledge Cd13 Id 1928069166 Size603makarandmone100% (9)
- The Fox Project, A ReappraisalDocument22 pagesThe Fox Project, A ReappraisalZemin OonNo ratings yet
- Electrical and Chemical Diagnostics of Transformer InsulationDocument33 pagesElectrical and Chemical Diagnostics of Transformer InsulationVikas Vooturi100% (1)
- Secure QR Code System: Raed M. Bani-Hani Yarub A. Wahsheh Mohammad B. Al-SarhanDocument6 pagesSecure QR Code System: Raed M. Bani-Hani Yarub A. Wahsheh Mohammad B. Al-SarhanAnonymous HeroNo ratings yet
- D-Series Trailer EBS: RSS Installation Requirements In/Out2 PowerDocument1 pageD-Series Trailer EBS: RSS Installation Requirements In/Out2 PowerDenisNo ratings yet
- Ch06 Solations Brigham 10th EDocument32 pagesCh06 Solations Brigham 10th ERafay HussainNo ratings yet
- SamsungLTE Table - RAN Call Release Causes 1.5Document137 pagesSamsungLTE Table - RAN Call Release Causes 1.5gargee502No ratings yet
- Query ManualDocument37 pagesQuery ManualstraNo ratings yet
- Kalimat Simple Present Tense Aktif Kalimat Simple Past Tense AktifDocument2 pagesKalimat Simple Present Tense Aktif Kalimat Simple Past Tense AktifRestu PamujiNo ratings yet
- Catabas Darlene - Orbital Core NotationDocument9 pagesCatabas Darlene - Orbital Core Notationapi-233267698No ratings yet