Download as docx, pdf, or txt
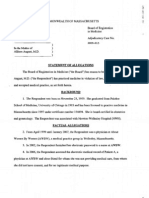
Woods & Water Medical Center
1019 S Knowles Avenue
New Richmond, WI 54017
(715) 246- 6561
www. WWMC.com
AUTHORIZATION FOR RELEASE OF MEDICAL INFORMATION
______________________________________________________________________________
Physician or Medical Group
To release the following information contained in my records, including information about
Human Immune Deficiency Virus Positivity (HIV+), Acquired Immune Deficiency Syndrome
(AIDS), and AIDS-Related Complex (ARC), as defined by the Ohio Department of Public Health.
Patient Name: Darwin Brown Date of Birth
6/7/1983
History and Physical X-ray/MRI-Reports
Laboratory Reports Surgery Report
x Pathology Reports Progress Report
x Audiology Reports x All Medical Records
Discharge Summary Treatment Summary
Others
To: Stanley Leonard, MD
Address: 233 North Smith Ave
Madison, WI 55731
I understand that I may revoke this authorization at any time and that it automatically expires
once the purpose for which it was intended is accomplished. My signature means that I have
read this form and/or have had it read to me and explained in a language that I can
understand.
Signature of Patient, Parent, or Guardian Today’s Date: 4/3/2024
You might also like
- Quiz Hospital DocumentationDocument5 pagesQuiz Hospital DocumentationJessica EdiosNo ratings yet
- Prior Authorization Request FormDocument3 pagesPrior Authorization Request FormvanessaNo ratings yet
- Briettavasser Job 33 Form 3Document1 pageBriettavasser Job 33 Form 3api-669728207No ratings yet
- Jordynkeller Job 33 Form 3Document1 pageJordynkeller Job 33 Form 3api-667709631No ratings yet
- Mama Nov 10, 2022Document1 pageMama Nov 10, 2022Little DreamcatcherNo ratings yet
- Kerriewing Job33 Form3Document1 pageKerriewing Job33 Form3api-749630850No ratings yet
- MRRF 11.10.2020Document2 pagesMRRF 11.10.2020oijewNo ratings yet
- Ohio Voter Rights CoalitionDocument19 pagesOhio Voter Rights CoalitionsrichardsonNo ratings yet
- Release MedicalInfo TODocument1 pageRelease MedicalInfo TOChristinah Tamby LewanikaNo ratings yet
- Attending Physicians Statement Crisis Cover Renal Failure - 041222Document2 pagesAttending Physicians Statement Crisis Cover Renal Failure - 041222max leeNo ratings yet
- Med ReleaseDocument1 pageMed ReleaseMatt SolheimNo ratings yet
- Ijpccr 2022 21Document3 pagesIjpccr 2022 21egabr322No ratings yet
- Authorization For Release of Medical InformationDocument1 pageAuthorization For Release of Medical Informationcig3fNo ratings yet
- Attending Physicians Statement Crisis Cover Muscular Dystrophy - 041222Document2 pagesAttending Physicians Statement Crisis Cover Muscular Dystrophy - 041222laraNo ratings yet
- If HP Maid Combined Assessor Provider Form ElectronicDocument10 pagesIf HP Maid Combined Assessor Provider Form ElectronicdawnNo ratings yet
- Informed Consent 5-2007Document2 pagesInformed Consent 5-2007Shanty AnitaNo ratings yet
- Patient Admission Hospital Admission ChecklistDocument6 pagesPatient Admission Hospital Admission ChecklistSweetly MamukoNo ratings yet
- 2015 1st Quarter JournalDocument32 pages2015 1st Quarter JournalAmberZeNo ratings yet
- GO Health Information StopDocument2 pagesGO Health Information StopNixZ Teruel2No ratings yet
- For Print - PADocument4 pagesFor Print - PAJU DYNo ratings yet
- Attending Physicians Statement Crisis Cover Major Organ Transplant - 041222Document2 pagesAttending Physicians Statement Crisis Cover Major Organ Transplant - 041222max leeNo ratings yet
- New York Health Opens New Office in Forest HillsDocument3 pagesNew York Health Opens New Office in Forest HillsPR.comNo ratings yet
- C107e Disclosure and Consent For Medical Surgical Diagnostic ProcedureTexasDocument5 pagesC107e Disclosure and Consent For Medical Surgical Diagnostic ProcedureTexaseverleighmae98No ratings yet
- Appendix A - FDocument54 pagesAppendix A - Fbakson college gr. noidaNo ratings yet
- State and Federal Regulations Governing The Release of Protected Health InformationDocument11 pagesState and Federal Regulations Governing The Release of Protected Health InformationIsabella SydneyNo ratings yet
- DetailsDocument21 pagesDetailskanthavelNo ratings yet
- Health Assessment-JaniDocument4 pagesHealth Assessment-Janijanijannahh17No ratings yet
- Medical Records Format - Riverside SBHC WVADocument4 pagesMedical Records Format - Riverside SBHC WVAnoto susantoNo ratings yet
- Activity On Hospital Documentation - HospPharmLab Act 1Document4 pagesActivity On Hospital Documentation - HospPharmLab Act 1Jan Aerielle AzulNo ratings yet
- Serial Procalcitonin Predicts Mortality in Severe Sepsis Patients Results From The Multicenter Procalcitonin MOnitoring SEpsis (MOSES) StudyDocument9 pagesSerial Procalcitonin Predicts Mortality in Severe Sepsis Patients Results From The Multicenter Procalcitonin MOnitoring SEpsis (MOSES) StudyNestor AmaroNo ratings yet
- Patient Authorization PDFDocument2 pagesPatient Authorization PDFTanessa WilliamsNo ratings yet
- Medical Record General Admission ConsentDocument1 pageMedical Record General Admission ConsentMohammedNo ratings yet
- Yale-New Haven Hospital Application For Physician GuestsDocument22 pagesYale-New Haven Hospital Application For Physician GuestsEsteban García EcheverryNo ratings yet
- Sample - Patient Consent FormDocument2 pagesSample - Patient Consent FormStudyBuddy - CondensedNotes CoolCatsNo ratings yet
- 22 States Petition CMS To End Vaccine MandateDocument39 pages22 States Petition CMS To End Vaccine MandateAssociation of American Physicians and SurgeonsNo ratings yet
- Ringland Ruling On Doctors' Testimony in Brooke Skylar Richardson CaseDocument11 pagesRingland Ruling On Doctors' Testimony in Brooke Skylar Richardson CaseWCPO 9 NewsNo ratings yet
- August ReprimandDocument7 pagesAugust ReprimandreprimandNo ratings yet
- Guide to Intellectual Disabilities: A Clinical HandbookFrom EverandGuide to Intellectual Disabilities: A Clinical HandbookJulie P. GentileNo ratings yet
- QR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Document1 pageQR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Yel BNo ratings yet
- Public Health Surveillance Sep 22 2011 (1) 1694196599Document42 pagesPublic Health Surveillance Sep 22 2011 (1) 1694196599Komal RamzaanNo ratings yet
- Medical Certificate XL Insurance Company SE ALC6250A 131219Document2 pagesMedical Certificate XL Insurance Company SE ALC6250A 131219FelipeNo ratings yet
- JIT 2363 Authorization To Release Med RecordsDocument2 pagesJIT 2363 Authorization To Release Med Recordsalan benedettaNo ratings yet
- HIM 200 Health RecordDocument32 pagesHIM 200 Health RecordMaryamNo ratings yet
- Electronic Medical Record ForensicsDocument14 pagesElectronic Medical Record ForensicskukuhNo ratings yet
- Policy Action Plan Nur 420 1 1Document11 pagesPolicy Action Plan Nur 420 1 1api-480618512No ratings yet
- Release of Info UMDocument1 pageRelease of Info UMsalmapratyushNo ratings yet
- Release From IVF FormsDocument2 pagesRelease From IVF Formsbinish LakNo ratings yet
- The Engines of Hippocrates: From the Dawn of Medicine to Medical and Pharmaceutical InformaticsFrom EverandThe Engines of Hippocrates: From the Dawn of Medicine to Medical and Pharmaceutical InformaticsNo ratings yet
- Cognitive Errors and Diagnostic Mistakes: A Case-Based Guide to Critical Thinking in MedicineFrom EverandCognitive Errors and Diagnostic Mistakes: A Case-Based Guide to Critical Thinking in MedicineNo ratings yet
- Committee On Veterans' Affairs House of Representatives: HearingDocument99 pagesCommittee On Veterans' Affairs House of Representatives: HearingScribd Government DocsNo ratings yet
- MDH Health Status AssessmentDocument1 pageMDH Health Status AssessmentDenise SiguaNo ratings yet
- Vaccination NoticeDocument2 pagesVaccination NoticeJulian Williams©™100% (2)
- Aem Physician Immunity Child Abuse Reporting OrdogDocument3 pagesAem Physician Immunity Child Abuse Reporting OrdogOpeyemiNo ratings yet
- 21 Dangers of The COVID Vaccine EbookDocument37 pages21 Dangers of The COVID Vaccine EbookWilberg SibugNo ratings yet
- Rights: Know YourDocument4 pagesRights: Know YourAli HusseinNo ratings yet
- Urgent Care Emergencies: Avoiding the Pitfalls and Improving the OutcomesFrom EverandUrgent Care Emergencies: Avoiding the Pitfalls and Improving the OutcomesNo ratings yet
- Health and Privacy PDFDocument40 pagesHealth and Privacy PDFMonika NegiNo ratings yet
- GM - FORMATO SINIESTROS - Medical ReportDocument5 pagesGM - FORMATO SINIESTROS - Medical ReportRicardo CadenaNo ratings yet
- Research Reportwiener1998Document12 pagesResearch Reportwiener1998maglangitmarvincNo ratings yet