Download as pdf or txt
You might also like
- Operator Manual - Brivo XR285amxDocument139 pagesOperator Manual - Brivo XR285amxMarve Felix100% (1)
- BriefingDocument BPAC Topic1A ConsiderationsForIronManagementDocument19 pagesBriefingDocument BPAC Topic1A ConsiderationsForIronManagementGilbertmichyNo ratings yet
- Frequent Blood Donations Alter Susceptibility of Red Blood Cells To Storage and Stress Induced HemolysisDocument12 pagesFrequent Blood Donations Alter Susceptibility of Red Blood Cells To Storage and Stress Induced HemolysisYuendri IrawantoNo ratings yet
- Iron Deficiency Anemia and Associated Risk Factors Among Teenagers in Najran Saudi ArabiaDocument9 pagesIron Deficiency Anemia and Associated Risk Factors Among Teenagers in Najran Saudi ArabiaZkdlin kaiNo ratings yet
- Iron Deficiency Anemia in Chronic Kidney Disease: ReviewDocument7 pagesIron Deficiency Anemia in Chronic Kidney Disease: ReviewSundas Ejaz100% (1)
- Choosing Wisely Avoid Using Hemoglobin To Evaluate Patients For Iron Deficiency in Susceptible Populations. Instead, Use FerritDocument1 pageChoosing Wisely Avoid Using Hemoglobin To Evaluate Patients For Iron Deficiency in Susceptible Populations. Instead, Use FerritbanrwshdhNo ratings yet
- Serum FerratinDocument4 pagesSerum FerratinSOUMYA A DR, DEPT.OF DENTAL SCIENCES,SRIHERNo ratings yet
- Validation Biochemistry MeasurementDocument35 pagesValidation Biochemistry Measurementhudan aziziNo ratings yet
- Assessment of Iron Deficiency Anemia Among Patients Attending Kigali University Teaching HospitalDocument5 pagesAssessment of Iron Deficiency Anemia Among Patients Attending Kigali University Teaching HospitalAzzam SaqrNo ratings yet
- 16identificación Del Estado de Hierro de Los Donantes de Sangre Mediante El Uso de Baja Densidad de Hemoglobina y Factor de Anemia MicrocíticaDocument11 pages16identificación Del Estado de Hierro de Los Donantes de Sangre Mediante El Uso de Baja Densidad de Hemoglobina y Factor de Anemia MicrocíticaFernandoVignoloNo ratings yet
- Reticulocyte Hemoglobin Equivalent As A Potential Marker PDFDocument10 pagesReticulocyte Hemoglobin Equivalent As A Potential Marker PDFFrancoNo ratings yet
- Nihms 1651021Document15 pagesNihms 1651021Anonymous 6dMqKOvNo ratings yet
- HemaDocument10 pagesHemadrkhengkiNo ratings yet
- (Pneumonia) Peerj 03 1374Document5 pages(Pneumonia) Peerj 03 1374Just For funNo ratings yet
- Iron Deficiency and Blood Donation.Document12 pagesIron Deficiency and Blood Donation.HECTOR ESTRELLA TOPETENo ratings yet
- Special Report Diagnosis and Management of Iron Deficiency in CKD: A Summary of The NICE Guideline Recommendations and Their RationaleDocument11 pagesSpecial Report Diagnosis and Management of Iron Deficiency in CKD: A Summary of The NICE Guideline Recommendations and Their RationaledrnattoNo ratings yet
- Jurnal InternasionalDocument6 pagesJurnal Internasionalbela melizaNo ratings yet
- Page 2010Document8 pagesPage 2010Anonymous 6dMqKOvNo ratings yet
- 21 - Prevalencia AnemiaDocument10 pages21 - Prevalencia AnemiaFernandoVignoloNo ratings yet
- Study of Iron Defficiency Anaemias, Clinical Presentations and Its Correaltion With Haematological and Biochemical ParametresDocument18 pagesStudy of Iron Defficiency Anaemias, Clinical Presentations and Its Correaltion With Haematological and Biochemical ParametresMayank KaushikNo ratings yet
- Preserving The National Blood Supply: Gary M. Brittenham, Harvey G. Klein, James P. Kushner, and Richard S. AjiokaDocument11 pagesPreserving The National Blood Supply: Gary M. Brittenham, Harvey G. Klein, James P. Kushner, and Richard S. Ajiokasarahloba100No ratings yet
- ArticlesDocument6 pagesArticlesbedahfkumiNo ratings yet
- 3 AnemiainPregnancyDocument6 pages3 AnemiainPregnancyGabriela RablNo ratings yet
- Camaschella 2017Document9 pagesCamaschella 2017Walter Jhon Delgadillo Arone0% (1)
- Using The Hemoglobin Content of Reticulocytes (RET-He) To Evaluate Anemia in Patients With CancerDocument7 pagesUsing The Hemoglobin Content of Reticulocytes (RET-He) To Evaluate Anemia in Patients With CancerMekar PalupiNo ratings yet
- BM and Iron ProfileDocument5 pagesBM and Iron ProfileShila SahaNo ratings yet
- FERRITINANDSERUMIRONDocument4 pagesFERRITINANDSERUMIRONAustin HoodNo ratings yet
- Am J Clin Nutr 2005 Schneider 1269 75Document7 pagesAm J Clin Nutr 2005 Schneider 1269 75Jony KechapNo ratings yet
- Iron Overload in Beta Thalassemia PDFDocument5 pagesIron Overload in Beta Thalassemia PDFyesikaNo ratings yet
- Main Article - BM PancytopeniaDocument10 pagesMain Article - BM PancytopeniaAbdur Rachman Ba'abdullahNo ratings yet
- Andi InaDocument5 pagesAndi InaFiLiOeiNo ratings yet
- Blood Donation - StatPearls - NCBI BookshelfDocument9 pagesBlood Donation - StatPearls - NCBI BookshelfAdamu TokalNo ratings yet
- J Nutr - 2017-Killilea-Jn 116 247171Document8 pagesJ Nutr - 2017-Killilea-Jn 116 247171Adil LagmarNo ratings yet
- Transfusion Transmissible Infections Among Voluntary Blood Donors in Port-Harcourt Metropolis, Rivers State, NigeriaDocument5 pagesTransfusion Transmissible Infections Among Voluntary Blood Donors in Port-Harcourt Metropolis, Rivers State, NigeriaIJEAB JournalNo ratings yet
- Iron Overload in Beta Thalassemia Major Patients: January 2017Document9 pagesIron Overload in Beta Thalassemia Major Patients: January 2017Khawlah AbdulameerNo ratings yet
- 1 s2.0 S0022316622028917 MainDocument8 pages1 s2.0 S0022316622028917 MainRafi DaniswaraNo ratings yet
- RDW 4 PDFDocument5 pagesRDW 4 PDFairusmayantiNo ratings yet
- Journal of Microscopy and Ultrastructure: Nora Nasir Al HassanDocument4 pagesJournal of Microscopy and Ultrastructure: Nora Nasir Al HassanAnis RanisNo ratings yet
- 271 592 1 SMDocument7 pages271 592 1 SMShandi Iriana SitorusNo ratings yet
- Artikel B InggrisDocument15 pagesArtikel B Inggrisramadan agustianNo ratings yet
- Low Iron Stores in Preconception Nulliparous Women A Two Center - 2020 - NutriDocument5 pagesLow Iron Stores in Preconception Nulliparous Women A Two Center - 2020 - NutriRinaNo ratings yet
- Diagnosis of Iron Deficiency and Iron Overload Nov 06Document8 pagesDiagnosis of Iron Deficiency and Iron Overload Nov 06Danielcc LeeNo ratings yet
- Meta Analisis StudiDocument13 pagesMeta Analisis StudiShafira Maulani putriNo ratings yet
- Hepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyDocument17 pagesHepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyAgungBudiPamungkasNo ratings yet
- Implication of Iron Deficiency 1 3Document32 pagesImplication of Iron Deficiency 1 3john EgesNo ratings yet
- Iron-Deficiency Anemia Among Children in Southwest IranDocument7 pagesIron-Deficiency Anemia Among Children in Southwest IrandooocNo ratings yet
- American J Hematol - 2024 - Wen - High Prevalence of Iron Deficiency and Socioeconomic Disparities in Laboratory ScreeningDocument8 pagesAmerican J Hematol - 2024 - Wen - High Prevalence of Iron Deficiency and Socioeconomic Disparities in Laboratory Screeninglakshminivas PingaliNo ratings yet
- Anemia 1Document8 pagesAnemia 1Patrick ValentinoNo ratings yet
- Abibakar Sheikaden Ismail 2019Document5 pagesAbibakar Sheikaden Ismail 2019Shafici CqadirNo ratings yet
- Iron Chelator DesferrioxamineDocument4 pagesIron Chelator DesferrioxamineMeiyanti MeiyantiNo ratings yet
- Research Open Access: Ahmed Ziedan and Sunil BhandariDocument10 pagesResearch Open Access: Ahmed Ziedan and Sunil BhandariAntika CahyatiNo ratings yet
- Credibility of The Measurement of Serum Ferritin and Transferrin Receptor As Indicators of Iron Deficiency Anemia in Hemodialysis PatientsDocument5 pagesCredibility of The Measurement of Serum Ferritin and Transferrin Receptor As Indicators of Iron Deficiency Anemia in Hemodialysis PatientsTanveerNo ratings yet
- A Review of Iron Overload in Beta-Thalassemia Major, and A Discussion On Alternative Potent Iron Chelation TargetsDocument9 pagesA Review of Iron Overload in Beta-Thalassemia Major, and A Discussion On Alternative Potent Iron Chelation TargetsFalisha Belvia KairinNo ratings yet
- Estimating The Prevalence of Iron Deficiency in The First TwoDocument8 pagesEstimating The Prevalence of Iron Deficiency in The First TwoJavier LunaNo ratings yet
- Hepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyDocument10 pagesHepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyjNo ratings yet
- Research Paper On Iron Deficiency AnemiaDocument5 pagesResearch Paper On Iron Deficiency Anemiawrglrkrhf100% (1)
- Assessment of The Utilization Patterns of Blood AT Mazabuka General Hospital, ZambiaDocument11 pagesAssessment of The Utilization Patterns of Blood AT Mazabuka General Hospital, ZambiaMukale Chipego MoongaNo ratings yet
- Iron Deficiency Research PaperDocument6 pagesIron Deficiency Research Papertwdhopwgf100% (1)
- Assessment of The Utilization Patterns of Blood AT Mazabuka General Hospital, ZambiaDocument11 pagesAssessment of The Utilization Patterns of Blood AT Mazabuka General Hospital, ZambiaMukale Chipego MoongaNo ratings yet
- Association Between Blood Groups and Blood Hemoglobin Levels in Rural Population of Kanchipuram District of Tamil NaduDocument4 pagesAssociation Between Blood Groups and Blood Hemoglobin Levels in Rural Population of Kanchipuram District of Tamil NaduEsrael kanbataNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 16: HematologyFrom EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyNo ratings yet
- Okra - Bamija: Natural Cosmet CsDocument2 pagesOkra - Bamija: Natural Cosmet CsVuci Mijalko BatinaNo ratings yet
- Dano Active AD OilDocument5 pagesDano Active AD Oiljrkresearch researchNo ratings yet
- DH 2011 1406 Part A DCHB Imphal WestDocument144 pagesDH 2011 1406 Part A DCHB Imphal Westpriyveer chauhanNo ratings yet
- Section Iv 510 (K) Summary of Safety and Effectiveness InformationDocument5 pagesSection Iv 510 (K) Summary of Safety and Effectiveness InformationLarissa GolucciNo ratings yet
- Superstar Catalogue 2024.4.6Document19 pagesSuperstar Catalogue 2024.4.6molisho13No ratings yet
- Risk Assessment Short FilmDocument1 pageRisk Assessment Short FilmMohammed MiahNo ratings yet
- Hse Program BMSDocument13 pagesHse Program BMSYogi HusniNo ratings yet
- Interkolaborasi ProfesionalDocument38 pagesInterkolaborasi Profesionalmuhamad hanapirohmanNo ratings yet
- Pt. Rania Jaya Farmarindo Daftar Harga Jual PersediaanDocument22 pagesPt. Rania Jaya Farmarindo Daftar Harga Jual PersediaanLalu EyiqNo ratings yet
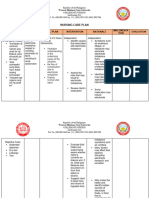
- Nursing Care Plan Risk For Electrolyte ImbalanceDocument4 pagesNursing Care Plan Risk For Electrolyte ImbalanceEzra Miguel DarundayNo ratings yet
- UntitledDocument43 pagesUntitledPbkkel 15No ratings yet
- Chemistry ProjecttttttttDocument51 pagesChemistry Projecttttttttrudra samadhiyaNo ratings yet
- Darc CasevacDocument4 pagesDarc CasevacLeoNo ratings yet
- General Surgery: Saturday, March 20th 2021Document17 pagesGeneral Surgery: Saturday, March 20th 2021ida ayu tungga dewiNo ratings yet
- Auriculotherapy Manual: Chinese and Western Systems of Ear AcupunctureDocument2 pagesAuriculotherapy Manual: Chinese and Western Systems of Ear AcupunctureYh KooNo ratings yet
- Panel Doctors List-India-14 Feb 12Document2 pagesPanel Doctors List-India-14 Feb 12Santosh Chaluvadi75% (4)
- Ampi+Salbactum Amo+ Clavulanate Piper+Tazobactam: ST ST ND ND ND ND TH ST ND TH TH TH RD RD RD TH THDocument1 pageAmpi+Salbactum Amo+ Clavulanate Piper+Tazobactam: ST ST ND ND ND ND TH ST ND TH TH TH RD RD RD TH THAnnieNo ratings yet
- Daftar Obat Lemari IcuDocument2 pagesDaftar Obat Lemari IcuHelin DriyanaNo ratings yet
- Skims Medical College & HospitalDocument5 pagesSkims Medical College & HospitalAaQib BhatNo ratings yet
- DAFTAR Harga Obat 2JULIDocument30 pagesDAFTAR Harga Obat 2JULIZaenuriNo ratings yet
- NABHDocument31 pagesNABHManjunath NNo ratings yet
- Biochemical Report: Id No: D393760Document2 pagesBiochemical Report: Id No: D393760Sultan AhmedNo ratings yet
- Lecture 2Document18 pagesLecture 2zainab ElsayedNo ratings yet
- Clinical Practice Guidelines For Acute Otitis Media in Children: A Systematic Review and Appraisal of European National GuidelinesDocument3 pagesClinical Practice Guidelines For Acute Otitis Media in Children: A Systematic Review and Appraisal of European National GuidelinesusmfdocNo ratings yet
- Exam Mot 5Document38 pagesExam Mot 5Mostafa Elsayed100% (1)
- Amanda Haynes Revised ResumeDocument2 pagesAmanda Haynes Revised Resumeapi-300845540No ratings yet
- 1-17-叶伟玉 Acupuncture and Tuina Report 1. (With Table)Document17 pages1-17-叶伟玉 Acupuncture and Tuina Report 1. (With Table)Virda Izzah PermatasariNo ratings yet
- Tramadol For Pain 2Document2 pagesTramadol For Pain 2William ImpNo ratings yet
- Pamoja Afya Brochure 2Document4 pagesPamoja Afya Brochure 2Chazzy f ChazzyNo ratings yet