Download as pdf or txt
You might also like
- Dexmed Mag SufDocument5 pagesDexmed Mag SufAshiyan IrfanNo ratings yet
- A Comparative Study of Clonidine and Lignocaine For Attenuating Pressor Responses To Laryngoscopy and Endotracheal Intubation in Neurosurgical CasesDocument5 pagesA Comparative Study of Clonidine and Lignocaine For Attenuating Pressor Responses To Laryngoscopy and Endotracheal Intubation in Neurosurgical Casesnethra nitinNo ratings yet
- A Comparative Study Between The Effect of Intravenous Versus Intranasal Dripping of Dexmedetomidine On Intraoperative Blood Loss During Functional EndDocument9 pagesA Comparative Study Between The Effect of Intravenous Versus Intranasal Dripping of Dexmedetomidine On Intraoperative Blood Loss During Functional Endabdelrhman alshawadfyNo ratings yet
- Dex Review 2007Document11 pagesDex Review 2007Jackelyne VilelaNo ratings yet
- 5 Ijca - 3 (2) - 316-323Document8 pages5 Ijca - 3 (2) - 316-323Mythology KingdomNo ratings yet
- AnesthEssaysRes11172-7351168 202511Document6 pagesAnesthEssaysRes11172-7351168 202511Tiêgo PiresNo ratings yet
- Dexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007Document11 pagesDexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007eriza amalia zainNo ratings yet
- Dexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007Document11 pagesDexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007eriza amalia zainNo ratings yet
- Dexmedetomidine Versus Magnesium Sulfate As Adjunct To General Anesthesia in Patients Undergoing Video-Assisted ThoracosDocument10 pagesDexmedetomidine Versus Magnesium Sulfate As Adjunct To General Anesthesia in Patients Undergoing Video-Assisted ThoracosprabaNo ratings yet
- JAMP - Mohamed Ali Edit.Document6 pagesJAMP - Mohamed Ali Edit.Iniya RajendranNo ratings yet
- Anaesth. Pain Intensive CareDocument11 pagesAnaesth. Pain Intensive CareRizki FitriaNo ratings yet
- Anesth Analg 2019 129 6 1504-11Document8 pagesAnesth Analg 2019 129 6 1504-11Fernando SousaNo ratings yet
- AnthropometryDocument6 pagesAnthropometryMinaz PatelNo ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Surve Rohini 2016Document7 pagesSurve Rohini 2016Amro MahmoudNo ratings yet
- Clinical Pharmacokinetics and Pharmacodynamics of DexmedetomidineDocument21 pagesClinical Pharmacokinetics and Pharmacodynamics of DexmedetomidineDavid González VegaNo ratings yet
- 2 Article JCDR FinalDocument4 pages2 Article JCDR FinalMythology KingdomNo ratings yet
- Use of Dexmedetomidine As A Sedative and Analgesic Agent in Critically Ill Adult Patients: A Meta-AnalysisDocument14 pagesUse of Dexmedetomidine As A Sedative and Analgesic Agent in Critically Ill Adult Patients: A Meta-AnalysisPatty Alarcón ParraNo ratings yet
- 1 s2.0 S0104001421002037 MainDocument7 pages1 s2.0 S0104001421002037 MainFarhana MardilaNo ratings yet
- Kelompok 4Document8 pagesKelompok 4TaraaNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument10 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Using Dexmedetomidine For Tourniquet Blood PressureDocument8 pagesUsing Dexmedetomidine For Tourniquet Blood PressureAlexNo ratings yet
- High Dose Versus Low Dose Intravenous Nitroglycerine For Sympathetic Crashing Acute Pulmonary EdemaDocument36 pagesHigh Dose Versus Low Dose Intravenous Nitroglycerine For Sympathetic Crashing Acute Pulmonary EdemaNaiara PfbNo ratings yet
- Dex Vs Tramadol Post Spinal ShiveringDocument4 pagesDex Vs Tramadol Post Spinal ShiveringSana AbbasNo ratings yet
- Ketamina y Dexmedetomidina en QuemadosDocument6 pagesKetamina y Dexmedetomidina en QuemadosVicky CascorNo ratings yet
- Comparison Efectiveness of Dexmedetomidine Versus Dexmedetomidine With Ketamine For Tympanoplasty Surgery Done Under Monitoredanaesthesia CareDocument7 pagesComparison Efectiveness of Dexmedetomidine Versus Dexmedetomidine With Ketamine For Tympanoplasty Surgery Done Under Monitoredanaesthesia CareIJAR JOURNALNo ratings yet
- Dexmedetomidine Combination With Fentanyl On Brain Oxygenation Using Invos in Intubed ICU Patients at Adam Malik Hospital, MedanDocument8 pagesDexmedetomidine Combination With Fentanyl On Brain Oxygenation Using Invos in Intubed ICU Patients at Adam Malik Hospital, MedanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Abstract Dexmed Vs Lignocaine Final Abstract and ArticleDocument25 pagesAbstract Dexmed Vs Lignocaine Final Abstract and ArticleDr.S.Easwaramoorthy IAGES Secretary 2020No ratings yet
- Remdesivir CardiotoxicityDocument5 pagesRemdesivir CardiotoxicitySeptiana Rizki FauziahNo ratings yet
- OJAnes 2019090613584267 PDFDocument12 pagesOJAnes 2019090613584267 PDFArifudin Cipto HusodoNo ratings yet
- JR Neuroanestesi 2Document7 pagesJR Neuroanestesi 2liashuban29No ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Infiltration Anaesthesia For Tympanoplasty: A Comparison of Dexmedetomidine and Clonidine As Adjuvants To Lignocaine and AdrenalineDocument7 pagesInfiltration Anaesthesia For Tympanoplasty: A Comparison of Dexmedetomidine and Clonidine As Adjuvants To Lignocaine and AdrenalineIJAR JOURNALNo ratings yet
- Ane-Publish Ahead of Print-10.1213 Ane.0000000000004887Document2 pagesAne-Publish Ahead of Print-10.1213 Ane.0000000000004887zaira ainurNo ratings yet
- Cardioprotective Effects of Curcumin Loaded Magnetic Hydrogel Nanocomposite Nanocurcumin Against Doxorubicin Induced Cardiac Toxicity in RatDocument10 pagesCardioprotective Effects of Curcumin Loaded Magnetic Hydrogel Nanocomposite Nanocurcumin Against Doxorubicin Induced Cardiac Toxicity in RatAisha MurtazaNo ratings yet
- Naaz 2014Document5 pagesNaaz 2014snookumsnjNo ratings yet
- 2021 - Dexmed LOSDocument9 pages2021 - Dexmed LOScringlesoreosNo ratings yet
- Jaicm MS Id 555727Document7 pagesJaicm MS Id 555727Mita KerjapyNo ratings yet
- Eckardt Et Al.Document12 pagesEckardt Et Al.sheharyarNo ratings yet
- Pone.0227664 Metanalise BNM ARDS AdultDocument14 pagesPone.0227664 Metanalise BNM ARDS AdultClaudia Mei Lan JaeNo ratings yet
- Drogas Durante La RCCPDocument9 pagesDrogas Durante La RCCPangelicaNo ratings yet
- 1 s2.0 S105307702300784X MainDocument7 pages1 s2.0 S105307702300784X MainalfintonNo ratings yet
- Books Binding BodyDocument71 pagesBooks Binding BodyToufique KhanNo ratings yet
- Journal of Critical CareDocument7 pagesJournal of Critical CareQonita Prasta AgustiaNo ratings yet
- Medicina 60 00751 v3Document16 pagesMedicina 60 00751 v3Cristina LopezNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Articulo 9 JulioDocument10 pagesArticulo 9 JulioPaloma AroliNo ratings yet
- Jamacardiology Cotter 2023 Oi 230063 1706752510.55879Document11 pagesJamacardiology Cotter 2023 Oi 230063 1706752510.55879qbn8zhzhwhNo ratings yet
- The Effect of Intravenously Administered Dexmedetomidine On Haemodynamic Response To Intubation in Patients Undergoing Surgery Under General AnaesthesiaDocument3 pagesThe Effect of Intravenously Administered Dexmedetomidine On Haemodynamic Response To Intubation in Patients Undergoing Surgery Under General AnaesthesiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hemodynamic Effects of Propofol and Dexmedetomidine in Septic Patients Without ShockDocument8 pagesHemodynamic Effects of Propofol and Dexmedetomidine in Septic Patients Without ShockSulindri IntanNo ratings yet
- Chudnofsky 2000Document8 pagesChudnofsky 2000Sanjeewa de AlwisNo ratings yet
- AN4 OA Sidharth-2Document6 pagesAN4 OA Sidharth-2Dede TarunaNo ratings yet
- APM 21 1989 FinalDocument15 pagesAPM 21 1989 FinalRuben HerediaNo ratings yet
- Indian Heart Journal: Research BriefDocument4 pagesIndian Heart Journal: Research BriefGitty RistianaNo ratings yet
- Ethos 2020Document14 pagesEthos 2020Radu CiprianNo ratings yet
- Cardiogenic Shock Dopamine or Norepinephrine .1Document4 pagesCardiogenic Shock Dopamine or Norepinephrine .1Diego RomeroNo ratings yet
- Attenuation of The Pressor Responses To.3Document7 pagesAttenuation of The Pressor Responses To.3prabaNo ratings yet
- Effect of Supplementation of Low Dose Intravenous Dexmedetomidine On Characteristics of Spinal Anaesthesia With Hyperbaric BupivacaineDocument5 pagesEffect of Supplementation of Low Dose Intravenous Dexmedetomidine On Characteristics of Spinal Anaesthesia With Hyperbaric BupivacaineMOHAMMED IQBALNo ratings yet
- Terapia Triple para EPOCDocument14 pagesTerapia Triple para EPOCSebastian Cebrian GuerreroNo ratings yet
- Dexmedetomidine Versus Magnesium Sulfate As Adjunct To General Anesthesia in Patients Undergoing Video-Assisted ThoracosDocument10 pagesDexmedetomidine Versus Magnesium Sulfate As Adjunct To General Anesthesia in Patients Undergoing Video-Assisted ThoracosprabaNo ratings yet
- 1 s2.0 S0308016121000223 Main1Document11 pages1 s2.0 S0308016121000223 Main1prabaNo ratings yet
- Question Bank: £ =X /Y =√1+ (2 ζ r) /√ (1-r) + (2 ζ r)Document6 pagesQuestion Bank: £ =X /Y =√1+ (2 ζ r) /√ (1-r) + (2 ζ r)prabaNo ratings yet
- MPDFDocument1 pageMPDFprabaNo ratings yet
- Unit 5Document7 pagesUnit 5prabaNo ratings yet
- Prabakaran 2017Document14 pagesPrabakaran 2017prabaNo ratings yet
- QC How To Make A Good Method StatementDocument3 pagesQC How To Make A Good Method StatementRsjBugtongNo ratings yet
- (M. Black, H.W. Pritchard) Desiccation and SurvivaDocument26 pages(M. Black, H.W. Pritchard) Desiccation and SurvivaLuis PedreroNo ratings yet
- Explanatory Styles Test ManualDocument47 pagesExplanatory Styles Test ManualKim Anthony T. MacaseroNo ratings yet
- Module Vi - Neleco2Document8 pagesModule Vi - Neleco2claudine padillonNo ratings yet
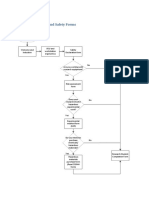
- Flow Chart: Health and Safety FormsDocument2 pagesFlow Chart: Health and Safety FormsBenouna FertNo ratings yet
- Passmedicine Statistics Note 2021: Prepared by DR - Abohaneen Mrcpase Telegram GroupDocument25 pagesPassmedicine Statistics Note 2021: Prepared by DR - Abohaneen Mrcpase Telegram Groupshenouda abdelshahidNo ratings yet
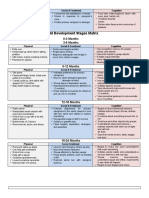
- Child Development Stages Matrix: 0-3 Months 3-6 MonthsDocument6 pagesChild Development Stages Matrix: 0-3 Months 3-6 MonthsJoenard Sadorra CabaelNo ratings yet
- Legal Responsibilities of The NurseDocument8 pagesLegal Responsibilities of The NurseWisley GadinganNo ratings yet
- Pula 2015Document15 pagesPula 2015Gabriela AviñaNo ratings yet
- Different Abilities Associated With Intelligence Test: Cristine Lae C. ErasgaDocument10 pagesDifferent Abilities Associated With Intelligence Test: Cristine Lae C. ErasgaDaisyNo ratings yet
- The Outer Limits - 7x02 - Patient Zero - en PDFDocument51 pagesThe Outer Limits - 7x02 - Patient Zero - en PDFoic-ad-agNo ratings yet
- Medical Tourism - ProposalDocument3 pagesMedical Tourism - ProposalANIL PSNo ratings yet
- APEGS Test: Competency Report: Name Discipline of Application JurisdictionDocument29 pagesAPEGS Test: Competency Report: Name Discipline of Application JurisdictionmycdrhelpNo ratings yet
- Anti-Cancer Drugs: Generic Name Strength SR. NO. Formulation TypeDocument4 pagesAnti-Cancer Drugs: Generic Name Strength SR. NO. Formulation TypeqaseemNo ratings yet
- Cofton Prospectus 2020-21 FINALDocument19 pagesCofton Prospectus 2020-21 FINALtheehengNo ratings yet
- Heat-Stress-Management-Training-Program-Samir 11 R4Document28 pagesHeat-Stress-Management-Training-Program-Samir 11 R4Sheri DiĺlNo ratings yet
- Contaminación en MéxicoDocument1 pageContaminación en MéxicoAngélica MayNo ratings yet
- Department of Biochemistry - Biochemistry Department - UMDCDocument17 pagesDepartment of Biochemistry - Biochemistry Department - UMDCTuf backlinkingNo ratings yet
- 0502 AcneDocument29 pages0502 AcneSam ShahbazNo ratings yet
- Sterile Abscess Due To Hyaluronic Acid A New Diagnosis and A Proposal For Treatment-A Series of Eight CasesDocument7 pagesSterile Abscess Due To Hyaluronic Acid A New Diagnosis and A Proposal For Treatment-A Series of Eight CasesGiovanna MazzettiNo ratings yet
- HeroDocument1 pageHeroEdward CullenNo ratings yet
- Linagliptin Drug MonographDocument7 pagesLinagliptin Drug MonographNearMelowNo ratings yet
- Standards For Competence For Registered MidwivesDocument14 pagesStandards For Competence For Registered MidwivescarNo ratings yet
- Supplementary Online Content: © 2020 American Medical Association. All Rights ReservedDocument19 pagesSupplementary Online Content: © 2020 American Medical Association. All Rights ReservedMai GonzalezNo ratings yet
- Fundamentals of Psychology 202110 - Lecture 1Document36 pagesFundamentals of Psychology 202110 - Lecture 1KITTIVONGSAK VONGSUTHEP KEITHNo ratings yet
- Otik A Liter o PisteDocument4 pagesOtik A Liter o PisteKonstantinos PapadopoulosNo ratings yet
- GPG PS003 Cold Formed BendsDocument80 pagesGPG PS003 Cold Formed BendsNirvana RamkissoonNo ratings yet
- Risk Management SyllabusDocument11 pagesRisk Management SyllabusKarl Villarubia100% (6)
- NSTPDocument10 pagesNSTPHilda DagyoNo ratings yet
- Lesson 5.1 Introduction To Health Information System HIS 1Document36 pagesLesson 5.1 Introduction To Health Information System HIS 1mariel santosNo ratings yet