Download as pdf or txt
You might also like
- Test Bank For Maternity Nursing 8th Edition, LowdermilkDocument26 pagesTest Bank For Maternity Nursing 8th Edition, LowdermilkILL101100% (3)
- WellsV2Review of Basic Science & Clinical DentistryDocument468 pagesWellsV2Review of Basic Science & Clinical DentistryLangNo ratings yet
- Necropsy - Killer Whale NootkaDocument5 pagesNecropsy - Killer Whale NootkaThe Orca Project Corp100% (2)
- Inguinal Hernia DictationDocument2 pagesInguinal Hernia DictationrainNo ratings yet
- The Male Genital ExaminationDocument4 pagesThe Male Genital ExaminationNiala AlmarioNo ratings yet
- The Chemical Basis of Medical Climatolo (Y: Professor Giorgio PiccardiDocument10 pagesThe Chemical Basis of Medical Climatolo (Y: Professor Giorgio PiccardimarcelNo ratings yet
- Transpalbebral Exenteration in CattleDocument4 pagesTranspalbebral Exenteration in Cattleಮನೋಜ್ ಭಾರದ್ವಾಜ್No ratings yet
- Knee Pain and The Infrapatellar Branch of The Saphenous: NerveDocument3 pagesKnee Pain and The Infrapatellar Branch of The Saphenous: NervefostizzNo ratings yet
- DrożdżeDocument16 pagesDrożdżeMateusz 'Dareth' HoppeNo ratings yet
- The Use of Computed Tomography in AvianDocument7 pagesThe Use of Computed Tomography in AvianDaniel BernalNo ratings yet
- Feingold 1977Document9 pagesFeingold 1977Lucas SantiagoNo ratings yet
- Wilkins, R. H. (1965) - Neurosurgical Classic-XXVIII.Document8 pagesWilkins, R. H. (1965) - Neurosurgical Classic-XXVIII.MARIA MONTSERRAT SOMOZA MONCADANo ratings yet
- Microsystem AcupunctureDocument3 pagesMicrosystem AcupunctureZulfa MayiruliNo ratings yet
- Hugo NecropsyDocument2 pagesHugo NecropsyilafatutooNo ratings yet
- Necropsy - Killer Whale HugoDocument5 pagesNecropsy - Killer Whale HugoThe Orca Project Corp100% (4)
- Biologic Beha of Canine Ammary Eopla Ms Ba Onahi A IficationDocument18 pagesBiologic Beha of Canine Ammary Eopla Ms Ba Onahi A IficationBryan AswNo ratings yet
- Placing A Lumbar Epidural CatheterDocument4 pagesPlacing A Lumbar Epidural CatheterGus LionsNo ratings yet
- Endodontic Emergencies and Its ManagementDocument40 pagesEndodontic Emergencies and Its Managementsonalbatra100% (1)
- Necropsy - Killer Whale CanuckDocument6 pagesNecropsy - Killer Whale CanuckThe Orca Project CorpNo ratings yet
- Articol ORLDocument6 pagesArticol ORLSabina BădilăNo ratings yet
- Nirrrsr Nlmri The During Anterior: Nr:a (Nir SiteDocument8 pagesNirrrsr Nlmri The During Anterior: Nr:a (Nir Siteณรงค์ชัย สอนดาNo ratings yet
- Piis0002713809601151 PDFDocument6 pagesPiis0002713809601151 PDFLuwinda SariNo ratings yet
- Invertebrate Tissue Culture: Applications in Medicine, Biology, and AgricultureFrom EverandInvertebrate Tissue Culture: Applications in Medicine, Biology, and AgricultureNo ratings yet
- 19650017047Document15 pages19650017047zinoyobNo ratings yet
- Music Therapy Coding Scheme (Raglio Et Al., 2006 - PR)Document6 pagesMusic Therapy Coding Scheme (Raglio Et Al., 2006 - PR)Nic Loc OnteNo ratings yet
- 1 s2.0 S000281778242021X MainDocument4 pages1 s2.0 S000281778242021X Main刘雨樵No ratings yet
- Nutrition Course Work One ExportDocument7 pagesNutrition Course Work One ExportYIKI ISAACNo ratings yet
- Grasshopper Dissection ManualDocument27 pagesGrasshopper Dissection ManualIryna ZapekaNo ratings yet
- Colour Atlas of The Anatomy and Pathology of The EpitympanumDocument110 pagesColour Atlas of The Anatomy and Pathology of The Epitympanumapi-26081450No ratings yet
- Topography of The Inferior Rectal Artery:: A Possible Cause of Chronic, Primary Anal FissureDocument10 pagesTopography of The Inferior Rectal Artery:: A Possible Cause of Chronic, Primary Anal FissureNadyaAlizaMulyadiNo ratings yet
- King John Necropsy Book 10mar16Document259 pagesKing John Necropsy Book 10mar16Wahid Danang PranathaNo ratings yet
- BF01705040Document4 pagesBF01705040fgomezvNo ratings yet
- Journals J-Neurosurg 22 5 Article-p465-PreviewDocument2 pagesJournals J-Neurosurg 22 5 Article-p465-PreviewNiswaNo ratings yet
- Mateen 2006Document5 pagesMateen 2006Gabriella Kezia LiongNo ratings yet
- Cerebral Blood Flow and Cerebral Death 1969Document15 pagesCerebral Blood Flow and Cerebral Death 1969horiionutNo ratings yet
- Archives of Pharmacology: Renal Handling of Oxalate A Micropuncture Study in The RatDocument5 pagesArchives of Pharmacology: Renal Handling of Oxalate A Micropuncture Study in The RatCLPHtheoryNo ratings yet
- Central Neck Dissection For or Recurrent Thyroglossal Duct CystsDocument4 pagesCentral Neck Dissection For or Recurrent Thyroglossal Duct CystsGunduz AgaNo ratings yet
- (10920684 - Neurosurgical Focus) Surgical Management of Trigeminal Schwannomas - Defining The Role For Endoscopic Endonasal ApproachesDocument9 pages(10920684 - Neurosurgical Focus) Surgical Management of Trigeminal Schwannomas - Defining The Role For Endoscopic Endonasal ApproachesasiyazaidiaNo ratings yet
- Variations in Course of Sciatic Nerve in Adult Human CadaversDocument5 pagesVariations in Course of Sciatic Nerve in Adult Human CadaversIJAR JOURNALNo ratings yet
- 2152014141658clinicalmethods 1 PDFDocument10 pages2152014141658clinicalmethods 1 PDFKay BristolNo ratings yet
- Group 4 PolygraphDocument23 pagesGroup 4 PolygraphirenecenagarciaNo ratings yet
- Necropsy Techniques: General Pathology (VPM 152) Jan 2008Document5 pagesNecropsy Techniques: General Pathology (VPM 152) Jan 2008Naresh RaviNo ratings yet
- Cancer - October 1976 - Fishkin - Cervical Lymph Node Metastasis As The First Manifestation of Localized ExtramedullaryDocument4 pagesCancer - October 1976 - Fishkin - Cervical Lymph Node Metastasis As The First Manifestation of Localized ExtramedullarymacklynmanuelNo ratings yet
- X ANATOMY HEAD AND NECKDocument16 pagesX ANATOMY HEAD AND NECKArijeet77No ratings yet
- Final 333Document119 pagesFinal 333nikhilrajput629No ratings yet
- Role of Tympanometry in Otosclerosis With A Proposal of New Classification For Type 'As' CurveDocument3 pagesRole of Tympanometry in Otosclerosis With A Proposal of New Classification For Type 'As' CurveHarshit AmbeshNo ratings yet
- Guidilene Linfoma PDFDocument52 pagesGuidilene Linfoma PDFPaloma SantanaNo ratings yet
- Department of Forensic Medicine, University of Dundee Lecture NotesDocument4 pagesDepartment of Forensic Medicine, University of Dundee Lecture NotesSusan Ram ShresthaNo ratings yet
- Transsphenoidal Hypophysectomy:: Postsurgical CT FindingsDocument6 pagesTranssphenoidal Hypophysectomy:: Postsurgical CT FindingsnurNo ratings yet
- Focusing of Charged Particles V2From EverandFocusing of Charged Particles V2Albert SeptierNo ratings yet
- Nasolacrimal Duct MuleDocument7 pagesNasolacrimal Duct MulealsadicNo ratings yet
- Clinical Psychology 1Document22 pagesClinical Psychology 1Salima HabeebNo ratings yet
- Auricular Prostheses and Osseointegrated Implants: Experience UclaDocument6 pagesAuricular Prostheses and Osseointegrated Implants: Experience UclanoranNo ratings yet
- Duktus ThyroglosusDocument13 pagesDuktus ThyroglosusOscar BrooksNo ratings yet
- 800 - Important - Fact Agrilearner App PDFDocument45 pages800 - Important - Fact Agrilearner App PDFShankar TanpureNo ratings yet
- Corpus Alienum PneumothoraxDocument3 pagesCorpus Alienum PneumothoraxPratita Jati PermatasariNo ratings yet
- KieiDocument18 pagesKieiIndrashis MandalNo ratings yet
- Fluid-Fluid Level Within The Ependymoma of The Posterior Fossa (#272117) - 252848Document3 pagesFluid-Fluid Level Within The Ependymoma of The Posterior Fossa (#272117) - 252848Thiru KannanNo ratings yet
- Parotidectomia - UpToDate 2022Document2 pagesParotidectomia - UpToDate 2022juanrangoneNo ratings yet
- Glandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.Document2 pagesGlandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.juanrangoneNo ratings yet
- Intraoperative Parathyroid Hormone Assays - Uptodate 2022Document18 pagesIntraoperative Parathyroid Hormone Assays - Uptodate 2022juanrangoneNo ratings yet
- 23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomaDocument19 pages23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomajuanrangoneNo ratings yet
- Parathyroidectomy in End-Stage Kidney Disease - Uptodate 2022Document27 pagesParathyroidectomy in End-Stage Kidney Disease - Uptodate 2022juanrangoneNo ratings yet
- Parathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022Document42 pagesParathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Surgical Anatomy of The Parathyroid Glands - Uptodate 2022Document8 pagesSurgical Anatomy of The Parathyroid Glands - Uptodate 2022juanrangoneNo ratings yet
- Preoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022Document22 pagesPreoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Parathyroid Surgery For Inherited Syndromes - Uptodate 2022Document25 pagesParathyroid Surgery For Inherited Syndromes - Uptodate 2022juanrangoneNo ratings yet
- Vandeventer 2016Document10 pagesVandeventer 2016juanrangoneNo ratings yet
- The Attachments of The Breast To The Chest Wall: A Dissection StudyDocument12 pagesThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneNo ratings yet
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDocument11 pages5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangoneNo ratings yet
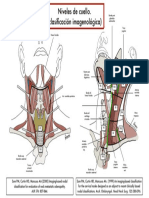
- Clasif Imagenológica Niveles de CuelloDocument1 pageClasif Imagenológica Niveles de CuellojuanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document5 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
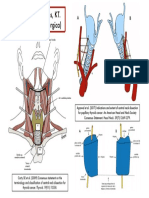
- Niveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesDocument1 pageNiveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesjuanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Repeat Case Breech 1Document73 pagesRepeat Case Breech 1Francis MendozaNo ratings yet
- The Gram-Negative Bacilli of Medical ImportanceDocument54 pagesThe Gram-Negative Bacilli of Medical ImportanceAna-Maria Nicolae100% (1)
- Weekly Outbreak COVID 19 ReportDocument44 pagesWeekly Outbreak COVID 19 ReportSinclair Broadcast Group - EugeneNo ratings yet
- This Guide Will Help You Find Your Way Around The Denver Health Medical Center Main CampusDocument2 pagesThis Guide Will Help You Find Your Way Around The Denver Health Medical Center Main Campus007003sNo ratings yet
- Positioning Improves The Oral and Pharyngeal Swallowing Function in Children With Cerebral PalsyDocument4 pagesPositioning Improves The Oral and Pharyngeal Swallowing Function in Children With Cerebral PalsySwathi GeethaNo ratings yet
- Amon409 415Document7 pagesAmon409 415MogleNo ratings yet
- Pain AssessmntDocument2 pagesPain Assessmntmohs2007100% (1)
- Ethylene Oxide C2h4o Safety Data Sheet Sds p4798Document10 pagesEthylene Oxide C2h4o Safety Data Sheet Sds p4798Yuna VerdyNo ratings yet
- Employees Compensation and State Insurance Fund HandoutDocument19 pagesEmployees Compensation and State Insurance Fund HandoutDanice Go GanNo ratings yet
- Khalifeh 2016Document16 pagesKhalifeh 2016Felipe LazoNo ratings yet
- Gandhi - Collected Works Vol 12Document487 pagesGandhi - Collected Works Vol 12Nrusimha ( नृसिंह )No ratings yet
- 1-30 November 2009 - Love Peace and Harmony JournalDocument291 pages1-30 November 2009 - Love Peace and Harmony JournalDavid Doğan BeyoNo ratings yet
- The Active Cycle of Breathing TechniqueDocument13 pagesThe Active Cycle of Breathing Techniquedan iacobNo ratings yet
- TrichDocument30 pagesTrichwadige4668No ratings yet
- Bassett and Turner 2007Document17 pagesBassett and Turner 2007Ludovic FanstenNo ratings yet
- Nutritional AssessmentDocument61 pagesNutritional Assessmentshahid9212No ratings yet
- Research Topics of Current ResearchDocument31 pagesResearch Topics of Current Researchmisgana etichaNo ratings yet
- Pediatrics JuniorDocument7 pagesPediatrics JuniorWise AmroNo ratings yet
- Acceptability and Development of PINEAPPLE POLVORON Hitosis Et - AlDocument57 pagesAcceptability and Development of PINEAPPLE POLVORON Hitosis Et - AlNebNo ratings yet
- GIT PathologyDocument27 pagesGIT PathologyIshali NuwanjiniNo ratings yet
- Multiple Gestation: Dr. Hotma Partogi Pasaribu Spog Sub Division of Fetomaternal Medical Faculty - Usu Rsham - RSPM MedanDocument47 pagesMultiple Gestation: Dr. Hotma Partogi Pasaribu Spog Sub Division of Fetomaternal Medical Faculty - Usu Rsham - RSPM MedanSyarifah KhamsiawanNo ratings yet
- The Breast - Comprehensive Management of Benign and Malignant Diseases 5e WWW Bookbaz IrDocument1,435 pagesThe Breast - Comprehensive Management of Benign and Malignant Diseases 5e WWW Bookbaz Irzahra m100% (1)
- Perinatal Manual of Southwestern OntarioDocument6 pagesPerinatal Manual of Southwestern OntarioƦя de GuzмѧN100% (1)
- Consequences of Sleep DeprivationDocument20 pagesConsequences of Sleep DeprivationAnonymous IXCgBcmXNo ratings yet
- WRITING CAE - Summary With VocabularyDocument18 pagesWRITING CAE - Summary With VocabularySerenajly100% (1)
- BrucellosisDocument65 pagesBrucellosisKotha Chaitanya AbhiramNo ratings yet
- Freaks and Marvels of Plant Life Or, Curiosities of VegetationDocument488 pagesFreaks and Marvels of Plant Life Or, Curiosities of VegetationTee SorensizzleNo ratings yet
- 2.4 SURG1 OncoDocument8 pages2.4 SURG1 OncoGeriz Daniella VigoNo ratings yet