Download as docx, pdf, or txt
You might also like
- Medical Certificate TemplateDocument2 pagesMedical Certificate TemplateAngelo Villafranca50% (4)
- CPS Dependent Information FormDocument2 pagesCPS Dependent Information Formtristero312No ratings yet
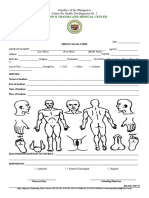
- Medico Legal Form 2017-WENGDocument1 pageMedico Legal Form 2017-WENGherbertNo ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 Palaroronaldodigma100% (1)
- Medical Certificate: Khyber Pakhtunkhwa Medical Form No. 4Document1 pageMedical Certificate: Khyber Pakhtunkhwa Medical Form No. 4Taimur Abdullah100% (1)
- Medical Health Assessment FormDocument1 pageMedical Health Assessment Formrufino delacruzNo ratings yet
- Medical CertificateDocument1 pageMedical Certificatemachristel salvadorNo ratings yet
- Medical Certificate W.IDocument1 pageMedical Certificate W.Itjhunter077No ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 Palarogtunida100% (1)
- Renap Membership Form 3Document1 pageRenap Membership Form 3california18dreamgirlNo ratings yet
- Medical Certificate: Division of SamarDocument1 pageMedical Certificate: Division of SamarWen Gab Dac100% (1)
- Contract 3Document1 pageContract 3aprrove ninjaNo ratings yet
- MED CERT District Final 01Document2 pagesMED CERT District Final 01Krizza Mae De LeonNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateChod DandoyNo ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 PalaroAllen EndayaNo ratings yet
- Medical-Certificate-1Document1 pageMedical-Certificate-1Jamil GutierrezNo ratings yet
- Sample Transmittal FileDocument1 pageSample Transmittal FileNonoemsAbanNo ratings yet
- Sample Medico Legal (Practice Court)Document1 pageSample Medico Legal (Practice Court)TeacherEliNo ratings yet
- Parent'S Permit: Tacloban City Title of Form: Parent's Permit Control No. EVSU-SASO-F-026 Revision No. 0 DateDocument1 pageParent'S Permit: Tacloban City Title of Form: Parent's Permit Control No. EVSU-SASO-F-026 Revision No. 0 DateMee Lai Calinao100% (1)
- Medical Certificate 2016 PalaroDocument6 pagesMedical Certificate 2016 PalaroJosefina LlamadoNo ratings yet
- Application Form For Edsp For RegionsDocument4 pagesApplication Form For Edsp For RegionsPagodNo ratings yet
- Medical Certificate: Department of EducationDocument2 pagesMedical Certificate: Department of EducationVanessa R. FloresNo ratings yet
- Dental Record Form CSPCDocument2 pagesDental Record Form CSPCJEREMY FOLLERO100% (1)
- Referral FormsDocument4 pagesReferral FormssittiejeanabedinNo ratings yet
- Ramain Medical CertificateDocument1 pageRamain Medical CertificateAlibasher MacalnasNo ratings yet
- Medical CertificateDocument1 pageMedical Certificatejohn ryan dela cruz0% (1)
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 Palaroanton082117No ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 PalaroTuvieron JoeyNo ratings yet
- Child's InformationDocument12 pagesChild's InformationymcawncNo ratings yet
- EDSP Application FormDocument4 pagesEDSP Application FormDave MillaresNo ratings yet
- Referral FormDocument2 pagesReferral FormRANDY BAOGBOG100% (1)
- Daily Health ChecklistDocument2 pagesDaily Health ChecklistMa. Charlene SisonNo ratings yet
- Authorization For Receipt of Medical RecordDocument1 pageAuthorization For Receipt of Medical Recordmayreddy.anushaNo ratings yet
- CerificateDocument1 pageCerificatecresencia bulataoNo ratings yet
- ApplicationDocument2 pagesApplicationMark McCoyNo ratings yet
- Refusal FormDocument1 pageRefusal FormViral Chann3LNo ratings yet
- Student'S Profile: 304444@deped - Gov.phDocument1 pageStudent'S Profile: 304444@deped - Gov.phAlessa Jeehan QuiñonesNo ratings yet
- Immersion Medical CertificateDocument1 pageImmersion Medical Certificatejestoni manipolNo ratings yet
- Parent ConsentDocument1 pageParent ConsentDennis FuerteNo ratings yet
- Phil HealthDocument1 pagePhil HealthLorence WarrenNo ratings yet
- Recreation Medical Forms 2018Document1 pageRecreation Medical Forms 2018Charlie BreitroseNo ratings yet
- Request FormDocument1 pageRequest FormMeycauayan DialysisNo ratings yet
- Libmanan North District: The Schools Division Superintendent Division of Camarines SurDocument8 pagesLibmanan North District: The Schools Division Superintendent Division of Camarines SurChard A. CañasNo ratings yet
- Chiropractic Application Form: Section A: Contact InformationDocument6 pagesChiropractic Application Form: Section A: Contact InformationAmanakeNo ratings yet
- OJT Application FormDocument3 pagesOJT Application FormSayong , John Mike J.No ratings yet
- Checklist For IntegrationDocument4 pagesChecklist For IntegrationMONALIE CHERRY RAMASNo ratings yet
- DENR Health Survey Form and Contact Person Form Page 2Document2 pagesDENR Health Survey Form and Contact Person Form Page 2Mary Jane BarrientosNo ratings yet
- Referral LetterDocument1 pageReferral LetterSugar CanibanNo ratings yet
- Final Hra-Hrdta-Form-01Document13 pagesFinal Hra-Hrdta-Form-01Charisse Jean PelominoNo ratings yet
- MGB07-1-Appln-for-FTAA (Application For Financial and Technical Assistance Agreement (FTAA) )Document3 pagesMGB07-1-Appln-for-FTAA (Application For Financial and Technical Assistance Agreement (FTAA) )Vyiel Gerald Ledesma CawalingNo ratings yet
- Palaro 2009 Medical CertificateDocument1 pagePalaro 2009 Medical CertificateHari Ng Sablay100% (1)
- Teen MedicalDocument1 pageTeen MedicalJohn C StarkNo ratings yet
- CHS Case NotebookDocument33 pagesCHS Case NotebookrigasanaorayNo ratings yet
- 2020 MedicalCertificate-ATHLETEDocument2 pages2020 MedicalCertificate-ATHLETEJoise Albertine J. Romblon100% (1)
- School Health Examination CardDocument3 pagesSchool Health Examination Cardjrose fay amatNo ratings yet
- Letter For TranspoDocument4 pagesLetter For TranspoRex S. CompaniaNo ratings yet
- Parent/ Consent Form: Boy Scouts of The Philippines Sultan Kudarat Council Lutayan District II Boy'S Application FormDocument4 pagesParent/ Consent Form: Boy Scouts of The Philippines Sultan Kudarat Council Lutayan District II Boy'S Application FormEdward Jr. PorrasNo ratings yet
- Medical Certificate Macabuhay TungaDocument1 pageMedical Certificate Macabuhay TungachuNo ratings yet
- ITR DentalDocument3 pagesITR Dentalnelmark.pepitoNo ratings yet
- HEATDocument9 pagesHEATnelmark.pepitoNo ratings yet
- C A QUizDocument2 pagesC A QUiznelmark.pepitoNo ratings yet
- Teaching Internship Certificate BSEDDocument1 pageTeaching Internship Certificate BSEDnelmark.pepitoNo ratings yet
- Digital TDocument2 pagesDigital Tnelmark.pepitoNo ratings yet
- Consumer Act of The PhilippinesDocument3 pagesConsumer Act of The Philippinesnelmark.pepitoNo ratings yet
- AttendanceDocument16 pagesAttendancenelmark.pepitoNo ratings yet
- Tooth ExtrationDocument1 pageTooth Extrationnelmark.pepitoNo ratings yet
- Rubric For PPT PresentationDocument1 pageRubric For PPT Presentationnelmark.pepitoNo ratings yet
- Republic of The Philippine1Document2 pagesRepublic of The Philippine1nelmark.pepitoNo ratings yet
- ARTS 7 Second QuarterDocument4 pagesARTS 7 Second Quarternelmark.pepitoNo ratings yet
- Boys DormDocument1 pageBoys Dormnelmark.pepitoNo ratings yet
- Department of Educatio1Document4 pagesDepartment of Educatio1nelmark.pepitoNo ratings yet