
Chile Case Study SP PHC 23april
Chile Case Study SP PHC 23april
You might also like
- Atlas: Mental HealthDocument136 pagesAtlas: Mental HealthAry AzharyNo ratings yet
- Germany HR PracticesDocument14 pagesGermany HR PracticesRamya ShreeNo ratings yet
- OHS Policies and Procedures ManualDocument13 pagesOHS Policies and Procedures Manualismailines100% (2)
- Qatar Healthcare Facilities Master Plan 2013-2033 - Sept 2014 PDFDocument167 pagesQatar Healthcare Facilities Master Plan 2013-2033 - Sept 2014 PDFbiomedmaulik100% (2)
- Kenya Case Study - SP PHC - 23aprilDocument39 pagesKenya Case Study - SP PHC - 23aprilmuratozbek1992No ratings yet
- Tajikistan-Case-Study SP PHC 6mayDocument33 pagesTajikistan-Case-Study SP PHC 6maymuratozbek1992No ratings yet
- Guide For Action: Eye Care in Health SystemsDocument72 pagesGuide For Action: Eye Care in Health SystemsFrederiel TarnateNo ratings yet
- Infection C. Primarios OmsDocument44 pagesInfection C. Primarios OmsMonica FerreiraNo ratings yet
- Guide For Action: Eye Care in Health SystemsDocument72 pagesGuide For Action: Eye Care in Health SystemsEunice DichosoNo ratings yet
- Maternal and Perinatal Death Surveillance and Response:: Materials To Support ImplementationDocument140 pagesMaternal and Perinatal Death Surveillance and Response:: Materials To Support ImplementationBianca Maria PricopNo ratings yet
- Best PracticesDocument40 pagesBest PracticesRachdi NasriNo ratings yet
- WHO Guidelines For Complementary FeedingDocument96 pagesWHO Guidelines For Complementary FeedingSiva KumarNo ratings yet
- 21 02 26-CSCS Assessment Summary-Written-ReportDocument27 pages21 02 26-CSCS Assessment Summary-Written-ReportTesfayeNo ratings yet
- B09035 EngDocument32 pagesB09035 Engmuratozbek1992No ratings yet
- CPG Management of Neonatal Jaundice (Second Edition)Document62 pagesCPG Management of Neonatal Jaundice (Second Edition)umiraihana1100% (1)
- Web Annexes A To K: Guidelines On The Management of Chronic Pain in ChildrenDocument42 pagesWeb Annexes A To K: Guidelines On The Management of Chronic Pain in ChildrenAshok KumarNo ratings yet
- COVID LCPG Quick Guide - 03april2023Document83 pagesCOVID LCPG Quick Guide - 03april2023glenn.astarlaboratoriesNo ratings yet
- WHO EURO 2023 7565 47332 69449 EngDocument43 pagesWHO EURO 2023 7565 47332 69449 EngWaheed Ul HaqueNo ratings yet
- Plan Oms Stop Obesity PresentationDocument44 pagesPlan Oms Stop Obesity PresentationPascale BrugNo ratings yet
- Towards A Grand Convergence For Child Survival and HealthDocument78 pagesTowards A Grand Convergence For Child Survival and HealthNicholasNo ratings yet
- WHO Consultancy ReportDocument36 pagesWHO Consultancy Reportmaxed.tendaiNo ratings yet
- Toolkit Multisectoral Action Plan For Noncommunicable DiseasesDocument23 pagesToolkit Multisectoral Action Plan For Noncommunicable DiseasesabarmasNo ratings yet
- Toolkit Multisectoral Action Plan For Noncommunicable DiseasesDocument31 pagesToolkit Multisectoral Action Plan For Noncommunicable DiseasesFifi Retiaty YasinNo ratings yet
- WHO HIS SDS 2017.7 EngDocument28 pagesWHO HIS SDS 2017.7 EngAlemania FebriyantaHutasuhutNo ratings yet
- Provider (6.3) ManualDocument44 pagesProvider (6.3) ManualFIAZ MAQBOOL FAZILINo ratings yet
- Action Plan 2022 2023Document74 pagesAction Plan 2022 2023Xam KhanNo ratings yet
- Marketin de Los Sustitutos de La Leche Materna - Texto en InglésDocument88 pagesMarketin de Los Sustitutos de La Leche Materna - Texto en InglésMaría José Agreguecolorfavorito ContrerasNo ratings yet
- EngDocument17 pagesEngnavenNo ratings yet
- Understanding The Global Measure of Primary Health Care Expenditure - FAQDocument12 pagesUnderstanding The Global Measure of Primary Health Care Expenditure - FAQNatalia LugovayaNo ratings yet
- WHO Report On Vaccine Denial 2020Document18 pagesWHO Report On Vaccine Denial 2020Marian BaghorNo ratings yet
- LCPG Quick GuideDocument86 pagesLCPG Quick Guidelemonysnicket0008No ratings yet
- National Health Insurance Vision, Challenges and Potential SolutionsDocument15 pagesNational Health Insurance Vision, Challenges and Potential Solutionsmariette1heferNo ratings yet
- Team-Based CareDocument36 pagesTeam-Based CarePatrick CommettantNo ratings yet
- Ethiopia Health Extension Program: A World Bank StudyDocument121 pagesEthiopia Health Extension Program: A World Bank StudyTgZGoldNo ratings yet
- 2020 09 H PP EuropaBio Patient-EngagementDocument6 pages2020 09 H PP EuropaBio Patient-Engagementqichen0818No ratings yet
- Infection Control and Waste MGT Plan - Part I and II - From NACO - CleanDocument58 pagesInfection Control and Waste MGT Plan - Part I and II - From NACO - CleanmalleshNo ratings yet
- Mental Health Atlas 2017Document72 pagesMental Health Atlas 2017sofiabloemNo ratings yet
- Mental Health Action Plan: For TheDocument29 pagesMental Health Action Plan: For TheDalene Erika GarbinNo ratings yet
- Building An NCD-ready Workforce: Technical Meeting ReportDocument48 pagesBuilding An NCD-ready Workforce: Technical Meeting ReportnavenNo ratings yet
- The Staff Are Not Motivated Anymore Health Care WoDocument14 pagesThe Staff Are Not Motivated Anymore Health Care WoMael MagnoNo ratings yet
- Background Document 3 From Science To PolicyDocument43 pagesBackground Document 3 From Science To PolicyvijayaveeNo ratings yet
- GHC - TOR IMO COVID VaccinesDocument4 pagesGHC - TOR IMO COVID VaccinesDan JosephNo ratings yet
- Framework: For Collaborative Action On Tuberculosis and ComorbiditiesDocument88 pagesFramework: For Collaborative Action On Tuberculosis and ComorbiditiesRatnaNo ratings yet
- Evidence Based Obstetrics CareDocument49 pagesEvidence Based Obstetrics CareSANANo ratings yet
- Anc UltrasoundDocument43 pagesAnc UltrasoundidahNo ratings yet
- Guidance On Developing National Learning Healthcare Systems To Sustain and Scale Up Delivery of Quality Maternal, Newborn and Child Health Care-EngDocument32 pagesGuidance On Developing National Learning Healthcare Systems To Sustain and Scale Up Delivery of Quality Maternal, Newborn and Child Health Care-EngrikaNo ratings yet
- Zambia Sanitation Policy and Planning Case Study For DiscussionDocument21 pagesZambia Sanitation Policy and Planning Case Study For DiscussionMzee Boydd Mkaka MwabutwaNo ratings yet
- 9789240084810-Eng WhoDocument26 pages9789240084810-Eng Whodewa putra yasaNo ratings yet
- Concept Note of The Primary Health Care QOC ActivityDocument21 pagesConcept Note of The Primary Health Care QOC ActivityTewodros Worku LiyewNo ratings yet
- Guidingprinciples Labelling Promoting HealthydietDocument46 pagesGuidingprinciples Labelling Promoting HealthydietAman Basheer SheikhNo ratings yet
- Equity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiDocument34 pagesEquity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiEjemai EboreimeNo ratings yet
- A Rede PIE Do ChileDocument8 pagesA Rede PIE Do ChileLuciano Teixeira RochaNo ratings yet
- Fourmula 1Document9 pagesFourmula 1Jamil Lorca100% (3)
- Div Class Title A Framework For Action To Improve Patient and Public InvolvementDocument9 pagesDiv Class Title A Framework For Action To Improve Patient and Public Involvementpaola salinasNo ratings yet
- Oig Gfoig10007audituzbekistan Report enDocument112 pagesOig Gfoig10007audituzbekistan Report encismercNo ratings yet
- HEOC Framework 9789241565134 - EngDocument80 pagesHEOC Framework 9789241565134 - Engleabooks16No ratings yet
- Use of Non-Sugar - WHO Guideline - 1Document18 pagesUse of Non-Sugar - WHO Guideline - 1treste trestexNo ratings yet
- Health Technology Assessment in Brazil - An International PerspectiveDocument14 pagesHealth Technology Assessment in Brazil - An International PerspectiveyutefupNo ratings yet
- Differentiated and Simplified Pre-Exposure Prophylaxis For HIV PreventionDocument46 pagesDifferentiated and Simplified Pre-Exposure Prophylaxis For HIV Preventionaugusto silvaNo ratings yet
- WHO PrEP 2022Document48 pagesWHO PrEP 2022OmarNo ratings yet
- Guidance On The Analysis and Use of Routine Health Information Systems WHO IRISDocument60 pagesGuidance On The Analysis and Use of Routine Health Information Systems WHO IRISDr. Abhishek OnkarNo ratings yet
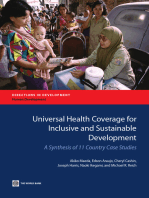
- Universal Health Coverage for Inclusive and Sustainable Development: A Synthesis of 11 Country Case StudiesFrom EverandUniversal Health Coverage for Inclusive and Sustainable Development: A Synthesis of 11 Country Case StudiesNo ratings yet
- Universal Health Coverage for Inclusive and Sustainable DevelopmentFrom EverandUniversal Health Coverage for Inclusive and Sustainable DevelopmentRating: 5 out of 5 stars5/5 (1)
- Ebook American Democracy Now PDF Full Chapter PDFDocument61 pagesEbook American Democracy Now PDF Full Chapter PDFjames.odell240100% (34)
- Acquisitions of Lands in Khyber Pakhtunkhwa (Concept Note)Document2 pagesAcquisitions of Lands in Khyber Pakhtunkhwa (Concept Note)Hayat Ali ShawNo ratings yet
- New York City Health + Hospitals ReportDocument56 pagesNew York City Health + Hospitals ReportcrainsnewyorkNo ratings yet
- Joint Commission International's Essentials of Health Care Quality and Patient SafetyDocument28 pagesJoint Commission International's Essentials of Health Care Quality and Patient Safetyedi100% (2)
- Health Insurance CardDocument3 pagesHealth Insurance Cardrajubhuyan1893No ratings yet
- AD EHSMS RF - Form E - Entity Quaterly Performance Report - V2.1Document3 pagesAD EHSMS RF - Form E - Entity Quaterly Performance Report - V2.1Suraj NairNo ratings yet
- Who Speaks For The Animals?Document4 pagesWho Speaks For The Animals?andersonanimallawNo ratings yet
- CHAPTER 8 (AutoRecovered)Document58 pagesCHAPTER 8 (AutoRecovered)Isabel MalicdanNo ratings yet
- Governemt Responsibilitlties ChartDocument2 pagesGovernemt Responsibilitlties Chartapi-331350096No ratings yet
- Mental Health Resources For The Asian American CommunityDocument4 pagesMental Health Resources For The Asian American CommunitydisgrasianNo ratings yet
- KentexDocument18 pagesKentexChristian Joseph ClavelNo ratings yet
- MDRDocument1 pageMDRRyuu WakuiNo ratings yet
- 01.chinese Government ScholarshipDocument4 pages01.chinese Government ScholarshipCvitković JosipNo ratings yet
- Applicationform Draft Print For AllDocument3 pagesApplicationform Draft Print For AllAnushka SinghNo ratings yet
- Health Insurance: Passed By: Rhea May PoriloDocument12 pagesHealth Insurance: Passed By: Rhea May PoriloRhea May PoriloNo ratings yet
- Gandhi - Collected Works Vol 84Document478 pagesGandhi - Collected Works Vol 84Nrusimha ( नृसिंह )No ratings yet
- Insurance Project - Risk Management For BMRCL The Bengaluru Metro Rail Corporation LTDDocument10 pagesInsurance Project - Risk Management For BMRCL The Bengaluru Metro Rail Corporation LTDJaswanth Singh RajpurohitNo ratings yet
- Car Insurance IrelandDocument4 pagesCar Insurance IrelandDavidNo ratings yet
- MEDISEP Hospital ListDocument1 pageMEDISEP Hospital Listഓല പീപ്പിNo ratings yet
- Form For Letter of NeedDocument2 pagesForm For Letter of NeedTejas ShahNo ratings yet
- The Employees State Insurance Act 1948Document21 pagesThe Employees State Insurance Act 1948Veena ManoharanNo ratings yet
- NGO Activities in Rural DevelopmentDocument7 pagesNGO Activities in Rural Developmentapi-378825575% (4)
- In The Matter of Charging Party Simone Teagle, Et Al. v. Respondent The City of New YorkDocument31 pagesIn The Matter of Charging Party Simone Teagle, Et Al. v. Respondent The City of New YorkEric SandersNo ratings yet
- Statistics On Poisoning Cases Region IX 2018Document3 pagesStatistics On Poisoning Cases Region IX 2018Rudy LangeNo ratings yet
- ACLU Lawsuit Over Homeless in SarasotaDocument418 pagesACLU Lawsuit Over Homeless in Sarasota10News WTSPNo ratings yet
- The Education of The Handicapped Amendments of 1986: Public Law 99-457Document16 pagesThe Education of The Handicapped Amendments of 1986: Public Law 99-457Jennie AnnNo ratings yet
- Perez v. Madrona DigestDocument2 pagesPerez v. Madrona DigestErla Elauria100% (1)
























































































Download as pdf or txt
You might also like
- Atlas: Mental HealthDocument136 pagesAtlas: Mental HealthAry AzharyNo ratings yet
- Germany HR PracticesDocument14 pagesGermany HR PracticesRamya ShreeNo ratings yet
- OHS Policies and Procedures ManualDocument13 pagesOHS Policies and Procedures Manualismailines100% (2)
- Qatar Healthcare Facilities Master Plan 2013-2033 - Sept 2014 PDFDocument167 pagesQatar Healthcare Facilities Master Plan 2013-2033 - Sept 2014 PDFbiomedmaulik100% (2)
- Kenya Case Study - SP PHC - 23aprilDocument39 pagesKenya Case Study - SP PHC - 23aprilmuratozbek1992No ratings yet
- Tajikistan-Case-Study SP PHC 6mayDocument33 pagesTajikistan-Case-Study SP PHC 6maymuratozbek1992No ratings yet
- Guide For Action: Eye Care in Health SystemsDocument72 pagesGuide For Action: Eye Care in Health SystemsFrederiel TarnateNo ratings yet
- Infection C. Primarios OmsDocument44 pagesInfection C. Primarios OmsMonica FerreiraNo ratings yet
- Guide For Action: Eye Care in Health SystemsDocument72 pagesGuide For Action: Eye Care in Health SystemsEunice DichosoNo ratings yet
- Maternal and Perinatal Death Surveillance and Response:: Materials To Support ImplementationDocument140 pagesMaternal and Perinatal Death Surveillance and Response:: Materials To Support ImplementationBianca Maria PricopNo ratings yet
- Best PracticesDocument40 pagesBest PracticesRachdi NasriNo ratings yet
- WHO Guidelines For Complementary FeedingDocument96 pagesWHO Guidelines For Complementary FeedingSiva KumarNo ratings yet
- 21 02 26-CSCS Assessment Summary-Written-ReportDocument27 pages21 02 26-CSCS Assessment Summary-Written-ReportTesfayeNo ratings yet
- B09035 EngDocument32 pagesB09035 Engmuratozbek1992No ratings yet
- CPG Management of Neonatal Jaundice (Second Edition)Document62 pagesCPG Management of Neonatal Jaundice (Second Edition)umiraihana1100% (1)
- Web Annexes A To K: Guidelines On The Management of Chronic Pain in ChildrenDocument42 pagesWeb Annexes A To K: Guidelines On The Management of Chronic Pain in ChildrenAshok KumarNo ratings yet
- COVID LCPG Quick Guide - 03april2023Document83 pagesCOVID LCPG Quick Guide - 03april2023glenn.astarlaboratoriesNo ratings yet
- WHO EURO 2023 7565 47332 69449 EngDocument43 pagesWHO EURO 2023 7565 47332 69449 EngWaheed Ul HaqueNo ratings yet
- Plan Oms Stop Obesity PresentationDocument44 pagesPlan Oms Stop Obesity PresentationPascale BrugNo ratings yet
- Towards A Grand Convergence For Child Survival and HealthDocument78 pagesTowards A Grand Convergence For Child Survival and HealthNicholasNo ratings yet
- WHO Consultancy ReportDocument36 pagesWHO Consultancy Reportmaxed.tendaiNo ratings yet
- Toolkit Multisectoral Action Plan For Noncommunicable DiseasesDocument23 pagesToolkit Multisectoral Action Plan For Noncommunicable DiseasesabarmasNo ratings yet
- Toolkit Multisectoral Action Plan For Noncommunicable DiseasesDocument31 pagesToolkit Multisectoral Action Plan For Noncommunicable DiseasesFifi Retiaty YasinNo ratings yet
- WHO HIS SDS 2017.7 EngDocument28 pagesWHO HIS SDS 2017.7 EngAlemania FebriyantaHutasuhutNo ratings yet
- Provider (6.3) ManualDocument44 pagesProvider (6.3) ManualFIAZ MAQBOOL FAZILINo ratings yet
- Action Plan 2022 2023Document74 pagesAction Plan 2022 2023Xam KhanNo ratings yet
- Marketin de Los Sustitutos de La Leche Materna - Texto en InglésDocument88 pagesMarketin de Los Sustitutos de La Leche Materna - Texto en InglésMaría José Agreguecolorfavorito ContrerasNo ratings yet
- EngDocument17 pagesEngnavenNo ratings yet
- Understanding The Global Measure of Primary Health Care Expenditure - FAQDocument12 pagesUnderstanding The Global Measure of Primary Health Care Expenditure - FAQNatalia LugovayaNo ratings yet
- WHO Report On Vaccine Denial 2020Document18 pagesWHO Report On Vaccine Denial 2020Marian BaghorNo ratings yet
- LCPG Quick GuideDocument86 pagesLCPG Quick Guidelemonysnicket0008No ratings yet
- National Health Insurance Vision, Challenges and Potential SolutionsDocument15 pagesNational Health Insurance Vision, Challenges and Potential Solutionsmariette1heferNo ratings yet
- Team-Based CareDocument36 pagesTeam-Based CarePatrick CommettantNo ratings yet
- Ethiopia Health Extension Program: A World Bank StudyDocument121 pagesEthiopia Health Extension Program: A World Bank StudyTgZGoldNo ratings yet
- 2020 09 H PP EuropaBio Patient-EngagementDocument6 pages2020 09 H PP EuropaBio Patient-Engagementqichen0818No ratings yet
- Infection Control and Waste MGT Plan - Part I and II - From NACO - CleanDocument58 pagesInfection Control and Waste MGT Plan - Part I and II - From NACO - CleanmalleshNo ratings yet
- Mental Health Atlas 2017Document72 pagesMental Health Atlas 2017sofiabloemNo ratings yet
- Mental Health Action Plan: For TheDocument29 pagesMental Health Action Plan: For TheDalene Erika GarbinNo ratings yet
- Building An NCD-ready Workforce: Technical Meeting ReportDocument48 pagesBuilding An NCD-ready Workforce: Technical Meeting ReportnavenNo ratings yet
- The Staff Are Not Motivated Anymore Health Care WoDocument14 pagesThe Staff Are Not Motivated Anymore Health Care WoMael MagnoNo ratings yet
- Background Document 3 From Science To PolicyDocument43 pagesBackground Document 3 From Science To PolicyvijayaveeNo ratings yet
- GHC - TOR IMO COVID VaccinesDocument4 pagesGHC - TOR IMO COVID VaccinesDan JosephNo ratings yet
- Framework: For Collaborative Action On Tuberculosis and ComorbiditiesDocument88 pagesFramework: For Collaborative Action On Tuberculosis and ComorbiditiesRatnaNo ratings yet
- Evidence Based Obstetrics CareDocument49 pagesEvidence Based Obstetrics CareSANANo ratings yet
- Anc UltrasoundDocument43 pagesAnc UltrasoundidahNo ratings yet
- Guidance On Developing National Learning Healthcare Systems To Sustain and Scale Up Delivery of Quality Maternal, Newborn and Child Health Care-EngDocument32 pagesGuidance On Developing National Learning Healthcare Systems To Sustain and Scale Up Delivery of Quality Maternal, Newborn and Child Health Care-EngrikaNo ratings yet
- Zambia Sanitation Policy and Planning Case Study For DiscussionDocument21 pagesZambia Sanitation Policy and Planning Case Study For DiscussionMzee Boydd Mkaka MwabutwaNo ratings yet
- 9789240084810-Eng WhoDocument26 pages9789240084810-Eng Whodewa putra yasaNo ratings yet
- Concept Note of The Primary Health Care QOC ActivityDocument21 pagesConcept Note of The Primary Health Care QOC ActivityTewodros Worku LiyewNo ratings yet
- Guidingprinciples Labelling Promoting HealthydietDocument46 pagesGuidingprinciples Labelling Promoting HealthydietAman Basheer SheikhNo ratings yet
- Equity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiDocument34 pagesEquity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiEjemai EboreimeNo ratings yet
- A Rede PIE Do ChileDocument8 pagesA Rede PIE Do ChileLuciano Teixeira RochaNo ratings yet
- Fourmula 1Document9 pagesFourmula 1Jamil Lorca100% (3)
- Div Class Title A Framework For Action To Improve Patient and Public InvolvementDocument9 pagesDiv Class Title A Framework For Action To Improve Patient and Public Involvementpaola salinasNo ratings yet
- Oig Gfoig10007audituzbekistan Report enDocument112 pagesOig Gfoig10007audituzbekistan Report encismercNo ratings yet
- HEOC Framework 9789241565134 - EngDocument80 pagesHEOC Framework 9789241565134 - Engleabooks16No ratings yet
- Use of Non-Sugar - WHO Guideline - 1Document18 pagesUse of Non-Sugar - WHO Guideline - 1treste trestexNo ratings yet
- Health Technology Assessment in Brazil - An International PerspectiveDocument14 pagesHealth Technology Assessment in Brazil - An International PerspectiveyutefupNo ratings yet
- Differentiated and Simplified Pre-Exposure Prophylaxis For HIV PreventionDocument46 pagesDifferentiated and Simplified Pre-Exposure Prophylaxis For HIV Preventionaugusto silvaNo ratings yet
- WHO PrEP 2022Document48 pagesWHO PrEP 2022OmarNo ratings yet
- Guidance On The Analysis and Use of Routine Health Information Systems WHO IRISDocument60 pagesGuidance On The Analysis and Use of Routine Health Information Systems WHO IRISDr. Abhishek OnkarNo ratings yet
- Universal Health Coverage for Inclusive and Sustainable Development: A Synthesis of 11 Country Case StudiesFrom EverandUniversal Health Coverage for Inclusive and Sustainable Development: A Synthesis of 11 Country Case StudiesNo ratings yet
- Universal Health Coverage for Inclusive and Sustainable DevelopmentFrom EverandUniversal Health Coverage for Inclusive and Sustainable DevelopmentRating: 5 out of 5 stars5/5 (1)
- Ebook American Democracy Now PDF Full Chapter PDFDocument61 pagesEbook American Democracy Now PDF Full Chapter PDFjames.odell240100% (34)
- Acquisitions of Lands in Khyber Pakhtunkhwa (Concept Note)Document2 pagesAcquisitions of Lands in Khyber Pakhtunkhwa (Concept Note)Hayat Ali ShawNo ratings yet
- New York City Health + Hospitals ReportDocument56 pagesNew York City Health + Hospitals ReportcrainsnewyorkNo ratings yet
- Joint Commission International's Essentials of Health Care Quality and Patient SafetyDocument28 pagesJoint Commission International's Essentials of Health Care Quality and Patient Safetyedi100% (2)
- Health Insurance CardDocument3 pagesHealth Insurance Cardrajubhuyan1893No ratings yet
- AD EHSMS RF - Form E - Entity Quaterly Performance Report - V2.1Document3 pagesAD EHSMS RF - Form E - Entity Quaterly Performance Report - V2.1Suraj NairNo ratings yet
- Who Speaks For The Animals?Document4 pagesWho Speaks For The Animals?andersonanimallawNo ratings yet
- CHAPTER 8 (AutoRecovered)Document58 pagesCHAPTER 8 (AutoRecovered)Isabel MalicdanNo ratings yet
- Governemt Responsibilitlties ChartDocument2 pagesGovernemt Responsibilitlties Chartapi-331350096No ratings yet
- Mental Health Resources For The Asian American CommunityDocument4 pagesMental Health Resources For The Asian American CommunitydisgrasianNo ratings yet
- KentexDocument18 pagesKentexChristian Joseph ClavelNo ratings yet
- MDRDocument1 pageMDRRyuu WakuiNo ratings yet
- 01.chinese Government ScholarshipDocument4 pages01.chinese Government ScholarshipCvitković JosipNo ratings yet
- Applicationform Draft Print For AllDocument3 pagesApplicationform Draft Print For AllAnushka SinghNo ratings yet
- Health Insurance: Passed By: Rhea May PoriloDocument12 pagesHealth Insurance: Passed By: Rhea May PoriloRhea May PoriloNo ratings yet
- Gandhi - Collected Works Vol 84Document478 pagesGandhi - Collected Works Vol 84Nrusimha ( नृसिंह )No ratings yet
- Insurance Project - Risk Management For BMRCL The Bengaluru Metro Rail Corporation LTDDocument10 pagesInsurance Project - Risk Management For BMRCL The Bengaluru Metro Rail Corporation LTDJaswanth Singh RajpurohitNo ratings yet
- Car Insurance IrelandDocument4 pagesCar Insurance IrelandDavidNo ratings yet
- MEDISEP Hospital ListDocument1 pageMEDISEP Hospital Listഓല പീപ്പിNo ratings yet
- Form For Letter of NeedDocument2 pagesForm For Letter of NeedTejas ShahNo ratings yet
- The Employees State Insurance Act 1948Document21 pagesThe Employees State Insurance Act 1948Veena ManoharanNo ratings yet
- NGO Activities in Rural DevelopmentDocument7 pagesNGO Activities in Rural Developmentapi-378825575% (4)
- In The Matter of Charging Party Simone Teagle, Et Al. v. Respondent The City of New YorkDocument31 pagesIn The Matter of Charging Party Simone Teagle, Et Al. v. Respondent The City of New YorkEric SandersNo ratings yet
- Statistics On Poisoning Cases Region IX 2018Document3 pagesStatistics On Poisoning Cases Region IX 2018Rudy LangeNo ratings yet
- ACLU Lawsuit Over Homeless in SarasotaDocument418 pagesACLU Lawsuit Over Homeless in Sarasota10News WTSPNo ratings yet
- The Education of The Handicapped Amendments of 1986: Public Law 99-457Document16 pagesThe Education of The Handicapped Amendments of 1986: Public Law 99-457Jennie AnnNo ratings yet
- Perez v. Madrona DigestDocument2 pagesPerez v. Madrona DigestErla Elauria100% (1)