Download as pdf or txt
You might also like
- Non Deliverable ForwardDocument17 pagesNon Deliverable ForwardManish GuptaNo ratings yet
- Original A Nation Wide SurveyDocument7 pagesOriginal A Nation Wide SurveyThe Heavenly ShadesNo ratings yet
- 1 s2.0 S0002817721006589 MainDocument11 pages1 s2.0 S0002817721006589 MainkhamilatusyNo ratings yet
- P.covid B.ingDocument9 pagesP.covid B.ingbudiNo ratings yet
- Corona Dentist Awareness PerceptionDocument7 pagesCorona Dentist Awareness PerceptionFirda IzzatiNo ratings yet
- 11 PDFDocument7 pages11 PDFfirdaizzatiNo ratings yet
- Covid-19. Are We Prepared For Future Outbreaks? An Online Survey To Assess Knowledge, Attitude and Awareness of Dental ProfessionalsDocument13 pagesCovid-19. Are We Prepared For Future Outbreaks? An Online Survey To Assess Knowledge, Attitude and Awareness of Dental ProfessionalsIJAR JOURNALNo ratings yet
- Impact of COVID-19 On Oral Emergency Services: Scientific Research ReportDocument55 pagesImpact of COVID-19 On Oral Emergency Services: Scientific Research ReportgeometrydashyioNo ratings yet
- JIndianAcadOralMedRadiol323203-5276647 143926Document2 pagesJIndianAcadOralMedRadiol323203-5276647 143926Nabila RizkikaNo ratings yet
- Change in Ophthalmology Practice During COVID-19 Pandemic: Egyptian PerspectiveDocument7 pagesChange in Ophthalmology Practice During COVID-19 Pandemic: Egyptian Perspectiveشهر رمزحنNo ratings yet
- Endodontic Treatment During COVID-19 Pandemic - Economic Perception of Dental ProfessionalsDocument8 pagesEndodontic Treatment During COVID-19 Pandemic - Economic Perception of Dental Professionalsbobs_fisioNo ratings yet
- Covid-19 Outbreak - Immediate and Long-Term Impacts On The Dental ProfessionDocument4 pagesCovid-19 Outbreak - Immediate and Long-Term Impacts On The Dental ProfessionYasir IsrarNo ratings yet
- Covid Dental AuxillariesDocument9 pagesCovid Dental AuxillariesfirdaizzatiNo ratings yet
- The Impact of Covid 19 Pandemic On Training and Mental Health of Residents A Cross Sectional StudyDocument11 pagesThe Impact of Covid 19 Pandemic On Training and Mental Health of Residents A Cross Sectional StudyramaNo ratings yet
- Fear and Practice Modifications Among Dentists To Combat Novel Coronavirus Disease (COVID-19) OutbreakDocument11 pagesFear and Practice Modifications Among Dentists To Combat Novel Coronavirus Disease (COVID-19) Outbreakharshita parasharNo ratings yet
- .Clinical Experience, Knowledge, Attitudes and Practice of Turkish Pediatric Dentists During The COVID-19 PandemicDocument23 pages.Clinical Experience, Knowledge, Attitudes and Practice of Turkish Pediatric Dentists During The COVID-19 PandemicMichael PomaNo ratings yet
- Assessment of Pediatric Dental Guidelines in The post-COVID 19 PeriodDocument14 pagesAssessment of Pediatric Dental Guidelines in The post-COVID 19 PeriodCha AlegriaNo ratings yet
- Impact of The COVID-19 Pandemic On The TimingDocument8 pagesImpact of The COVID-19 Pandemic On The TimingMichael PomaNo ratings yet
- Editing of ProposalDocument9 pagesEditing of ProposalMustafaNo ratings yet
- Assessment of Paediatric Dental Guidelines and CarDocument15 pagesAssessment of Paediatric Dental Guidelines and CarRisana RahoofNo ratings yet
- Alharbi Guideline Covid-19Document6 pagesAlharbi Guideline Covid-19desy purnama sariNo ratings yet
- IntJOralHealthDent 6 2 122 125Document5 pagesIntJOralHealthDent 6 2 122 125Laura Putri TraviraNo ratings yet
- Knowledge, Attitude and Practice Regarding COVID-19 and Its Impact On Dentistry: A Cross-Sectional Survey Among Nepalese DentistsDocument7 pagesKnowledge, Attitude and Practice Regarding COVID-19 and Its Impact On Dentistry: A Cross-Sectional Survey Among Nepalese DentistsSalon LamichhaneNo ratings yet
- Dental Patients' Perspective On COVID-19: A Systematic ReviewDocument18 pagesDental Patients' Perspective On COVID-19: A Systematic ReviewJohnny CHNo ratings yet
- COVID-19's Impact On Private Practice and Academic Dentistry in North AmericaDocument4 pagesCOVID-19's Impact On Private Practice and Academic Dentistry in North AmericaJoDaNo ratings yet
- Guidelines For Dental Care Provision During The COVID-19 PandemicDocument7 pagesGuidelines For Dental Care Provision During The COVID-19 PandemicFirda IzzatiNo ratings yet
- Impact of Pandemic Period of Covid - 19 in Dental MedicineDocument11 pagesImpact of Pandemic Period of Covid - 19 in Dental MedicineAndreea Andrei AndreeaNo ratings yet
- Dental Care and Personal Protective Measures For Dentists and Non-Dental Health Care WorkersDocument5 pagesDental Care and Personal Protective Measures For Dentists and Non-Dental Health Care WorkersKalpanaNo ratings yet
- COVID-19 PublicationDocument8 pagesCOVID-19 PublicationMariam TariqNo ratings yet
- Coronavirus Disease 2019 (COVID-19) : Emerging and Future Challenges For Dental and Oral MedicineDocument7 pagesCoronavirus Disease 2019 (COVID-19) : Emerging and Future Challenges For Dental and Oral MedicineDaniela Valencia FigueroaNo ratings yet
- Dentistry in Post COVIDDocument3 pagesDentistry in Post COVIDsagrika groverNo ratings yet
- Knowledge of Legal Aspects in Teledentistry AmongDocument6 pagesKnowledge of Legal Aspects in Teledentistry AmongGian ErnestoNo ratings yet
- The Impact of The COVID-19 Epidemic On The Utilization of Emergency Dental ServicesDocument4 pagesThe Impact of The COVID-19 Epidemic On The Utilization of Emergency Dental ServicesMishellKarelisMorochoSegarraNo ratings yet
- Pandemic Preparedness of Dentists Against Coronavirus Disease: A Saudi Arabian ExperienceDocument13 pagesPandemic Preparedness of Dentists Against Coronavirus Disease: A Saudi Arabian ExperiencenoviNo ratings yet
- A Scoping Review of Respirator Literature and A Survey Among Dental ProfessionalsDocument12 pagesA Scoping Review of Respirator Literature and A Survey Among Dental ProfessionalsHNiondiv EdvmpoeirmNo ratings yet
- Compliance With Health ProtocolsDocument7 pagesCompliance With Health Protocolskadoxe1682No ratings yet
- Maternal Practices Towards Dental Treatment of Primary School Children After The Emergence of Covid 19Document6 pagesMaternal Practices Towards Dental Treatment of Primary School Children After The Emergence of Covid 19International Journal of Innovative Science and Research TechnologyNo ratings yet
- JFMPC 2020 TDDocument2 pagesJFMPC 2020 TDTulika WakhlooNo ratings yet
- Pancasila Gigi JurnalDocument12 pagesPancasila Gigi Jurnalandini fitriNo ratings yet
- Challenges and Impact of COVID-19 Lockdown On Indian Optometry Practice: A Survey-Based StudyDocument9 pagesChallenges and Impact of COVID-19 Lockdown On Indian Optometry Practice: A Survey-Based StudyLaura Alvarado BrophyNo ratings yet
- Outpatient Otolaryngology in The Era of COVID-19: A Data-Driven Analysis of Practice PatternsDocument7 pagesOutpatient Otolaryngology in The Era of COVID-19: A Data-Driven Analysis of Practice PatternsMada Dwi HariNo ratings yet
- Ijerph 18 05889Document18 pagesIjerph 18 05889Febri YolandaNo ratings yet
- Knowledge Dental Anxiety and Patient ExpectationsDocument9 pagesKnowledge Dental Anxiety and Patient ExpectationsbenjoscoliNo ratings yet
- 1 s2.0 S1473309920302267 MainDocument2 pages1 s2.0 S1473309920302267 MainMarlo Jules LagunaNo ratings yet
- The Impact of COVID-19 Pandemic On The Academic Performance of Veterinary Medical StudentsDocument8 pagesThe Impact of COVID-19 Pandemic On The Academic Performance of Veterinary Medical StudentsRitam chaturvediNo ratings yet
- A Review of COVID-19 and The Implications For Orthodontic Provision in EnglandDocument8 pagesA Review of COVID-19 and The Implications For Orthodontic Provision in Englanddruzair007No ratings yet
- Ophthalmic Complaints in Face Mask Wearing Prevalence Treatment and Prevention With A Potential Protective Effect Against SARS CoV 2Document14 pagesOphthalmic Complaints in Face Mask Wearing Prevalence Treatment and Prevention With A Potential Protective Effect Against SARS CoV 2Feli FelNo ratings yet
- .Management of The Oral Health of Children During The COVID-19Document6 pages.Management of The Oral Health of Children During The COVID-19Michael PomaNo ratings yet
- Cross Infection 4444Document12 pagesCross Infection 4444khamilatusyNo ratings yet
- Dental Considerations After The Outbreak of 2019 Novel Coronavirus Disease: A Review of LiteratureDocument7 pagesDental Considerations After The Outbreak of 2019 Novel Coronavirus Disease: A Review of Literatureharshita parasharNo ratings yet
- Clinical Endodontic Management During The COVID-19 Pandemic: A Literature Review and Clinical RecommendationsDocument11 pagesClinical Endodontic Management During The COVID-19 Pandemic: A Literature Review and Clinical Recommendationsangel gudiyaNo ratings yet
- Covid 19 Article Dental ImpactDocument10 pagesCovid 19 Article Dental Impactwedad jumaNo ratings yet
- 1 s2.0 S1350946220300720 MainDocument32 pages1 s2.0 S1350946220300720 MainSaba ChavchavadzeNo ratings yet
- How COVID-19 Has Affected DentistryDocument13 pagesHow COVID-19 Has Affected DentistryDeborah AnneNo ratings yet
- Covid 19 ItaliaDocument9 pagesCovid 19 ItaliaSergio Losada AmayaNo ratings yet
- COVID-19-Orthodontic Care During and After The Pandemic: A Narrative ReviewDocument15 pagesCOVID-19-Orthodontic Care During and After The Pandemic: A Narrative ReviewAndreea Andrei AndreeaNo ratings yet
- Incidence of COVID-19 Virus Transmission in Three Dental Offices: A 6-Month Retrospective StudyDocument7 pagesIncidence of COVID-19 Virus Transmission in Three Dental Offices: A 6-Month Retrospective StudyAlexNo ratings yet
- Abbas 2020Document7 pagesAbbas 2020desy purnama sariNo ratings yet
- GJESM Volume 8 Issue 3 Pages 327-338Document12 pagesGJESM Volume 8 Issue 3 Pages 327-338GJESMNo ratings yet
- Index - PHPP Revista&tipo Pdf-Simple&pii S1578219021000603 3Document2 pagesIndex - PHPP Revista&tipo Pdf-Simple&pii S1578219021000603 3Iago GonçalvesNo ratings yet
- HEALTHCARE SERVICE QUALITY AND PATIENT SATISFACTION IN OMANI PUBLIC HOSPITALS THROUGHOUT COVID-19 ERA: AN EMPIRICAL INVESTIGATIONFrom EverandHEALTHCARE SERVICE QUALITY AND PATIENT SATISFACTION IN OMANI PUBLIC HOSPITALS THROUGHOUT COVID-19 ERA: AN EMPIRICAL INVESTIGATIONNo ratings yet
- Where To Find Large Datasets Open To The PublicDocument41 pagesWhere To Find Large Datasets Open To The PublicgeronimlNo ratings yet
- CCNA1 Mod 6Document28 pagesCCNA1 Mod 6KlokanNo ratings yet
- Phantom Turbo 6000Document22 pagesPhantom Turbo 6000Manos LoukianosNo ratings yet
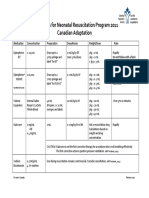
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- General Definition of Sag and Tension in Electrical Transmission LinesDocument11 pagesGeneral Definition of Sag and Tension in Electrical Transmission Linesdskymaximus67% (3)
- People Vs OandasanDocument2 pagesPeople Vs OandasanAdoha Lei T Blanco100% (1)
- Nihongo Lesson FL 1Document21 pagesNihongo Lesson FL 1Lee MendozaNo ratings yet
- Managed Pressure Drilling Modeling & Simulation (A Case Study)Document8 pagesManaged Pressure Drilling Modeling & Simulation (A Case Study)Mejbahul SarkerNo ratings yet
- Class XII Applied Mathematics 2023-24 (K R Mangalam School)Document7 pagesClass XII Applied Mathematics 2023-24 (K R Mangalam School)GouriJayanNo ratings yet
- जनावरहरूमा फेनबेन्डाजोलको प्रयोग (Use of Fenbendazole in animals)Document17 pagesजनावरहरूमा फेनबेन्डाजोलको प्रयोग (Use of Fenbendazole in animals)Jibachha SahNo ratings yet
- Model QuestionsDocument27 pagesModel Questionskalyan555No ratings yet
- General Information: Location A Location BDocument2 pagesGeneral Information: Location A Location BNikNo ratings yet
- Lubricattng Oil For Marine EnginesDocument5 pagesLubricattng Oil For Marine Enginesemmsh71No ratings yet
- Laporan Kasus (Stroke NHS)Document4 pagesLaporan Kasus (Stroke NHS)keluargacendanaNo ratings yet
- Studying The Performance of Pongamia Biodiesel by Using Nano Partical Fuel AdditivesDocument6 pagesStudying The Performance of Pongamia Biodiesel by Using Nano Partical Fuel Additivessemi1919No ratings yet
- Dynamic Modeling of PMSMDocument10 pagesDynamic Modeling of PMSMHisham Magdi El DeebNo ratings yet
- Case Study CCTV BuildingDocument11 pagesCase Study CCTV BuildingChendra Ling LingNo ratings yet
- RIP Riverbed LabDocument13 pagesRIP Riverbed LabnekaNo ratings yet
- Section A - QuestionsDocument27 pagesSection A - Questionsnek_akhtar87250% (1)
- Multimedia Chapter 1 and 2Document22 pagesMultimedia Chapter 1 and 2tsegab bekeleNo ratings yet
- Game Master's Kit: An Accessory For The Dragon Age RPGDocument32 pagesGame Master's Kit: An Accessory For The Dragon Age RPGLuiz Fernando Rodrigues CarrijoNo ratings yet
- PMEC Flash CardsDocument17 pagesPMEC Flash CardsHariyantoNo ratings yet
- CSA Standard W178.2-01: Certification of Welding InspectorsDocument2 pagesCSA Standard W178.2-01: Certification of Welding InspectorsramalingamNo ratings yet
- DLL WK 10 LC 171819Document14 pagesDLL WK 10 LC 171819Regiel Guiang ArnibalNo ratings yet
- Japan TechnologyDocument4 pagesJapan TechnologyMa Leonora SorianoNo ratings yet
- Actuator DX PDFDocument6 pagesActuator DX PDFFelix Enrique MoratayaNo ratings yet
- CascadeTEK Vacuum Oven ManualDocument49 pagesCascadeTEK Vacuum Oven ManualCascade TEKNo ratings yet
- 72.61.00.045 26-MAR-2020 08-DEC-2021 Closed A319-100N, A320-200N, A321-200N, A321-200NX, A321-200NY 72-61 Iae LLC Pratt & Whitney TFU UpdateDocument9 pages72.61.00.045 26-MAR-2020 08-DEC-2021 Closed A319-100N, A320-200N, A321-200N, A321-200NX, A321-200NY 72-61 Iae LLC Pratt & Whitney TFU UpdatejivomirNo ratings yet
- BSN1-2 Lab Activity 2.2 Proteins DenaturationDocument3 pagesBSN1-2 Lab Activity 2.2 Proteins DenaturationCristine EchaveNo ratings yet