Download as pdf or txt
You might also like
- Apixaban For Stroke Prevention in Subclinical AFDocument11 pagesApixaban For Stroke Prevention in Subclinical AFalaahossam591No ratings yet
- Misinterpretation of TasawwufDocument260 pagesMisinterpretation of TasawwufSpirituality Should Be LivedNo ratings yet
- Medicinus Maret 2018 PDFDocument25 pagesMedicinus Maret 2018 PDFIsdiana IsmailNo ratings yet
- Pulmonary Hypertension: A Patient's Survival Guide: Fifth Edition, 2013 RevisionFrom EverandPulmonary Hypertension: A Patient's Survival Guide: Fifth Edition, 2013 RevisionRating: 5 out of 5 stars5/5 (1)
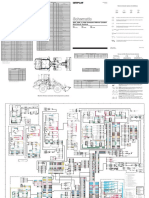
- 902, 906, & 908 Compact Wheel Loader Electrical System: Machine Harness Connector and Component LocationsDocument2 pages902, 906, & 908 Compact Wheel Loader Electrical System: Machine Harness Connector and Component Locationsait mimouneNo ratings yet
- Stat NotesDocument40 pagesStat Notesssckp86No ratings yet
- Biochemistry of Oxidative Stress - Physiopathology and Clinical Aspects (PDFDrive)Document448 pagesBiochemistry of Oxidative Stress - Physiopathology and Clinical Aspects (PDFDrive)Vitoria LimaNo ratings yet
- ASpirin Target KerjaDocument15 pagesASpirin Target KerjaANISA RACHMITA ARIANTI 2020No ratings yet
- Medical Management of Missed Abortion and Anembryonic PregnancyDocument2 pagesMedical Management of Missed Abortion and Anembryonic PregnancyIriamana Liasyarah MarudinNo ratings yet
- Section: of The History of MedicineDocument10 pagesSection: of The History of MedicineaceNo ratings yet
- PIIS0012369216529419Document3 pagesPIIS0012369216529419puskesmassedadap.2023No ratings yet
- Nejmcpc 1909628Document11 pagesNejmcpc 1909628MS R.No ratings yet
- Jurnal OnlineDocument5 pagesJurnal OnlineWireifnitedNo ratings yet
- Drug Information HandbookDocument2 pagesDrug Information HandbookdiahNo ratings yet
- A History of Pulmonary Embolism and Deep Venous ThrombosisDocument17 pagesA History of Pulmonary Embolism and Deep Venous ThrombosisAleksVaReNo ratings yet
- Brmedj03772 0032aDocument1 pageBrmedj03772 0032afpm5948No ratings yet
- ClassicsDocument2 pagesClassicsIndra Budi PermanaNo ratings yet
- Improving Outcomes in Heart Failure: A Personal PerspectiveDocument4 pagesImproving Outcomes in Heart Failure: A Personal PerspectiveyeinisehNo ratings yet
- Receptive SubstancesDocument22 pagesReceptive SubstancesDaniel ChaguenNo ratings yet
- Brjgenprac00016 0058bDocument2 pagesBrjgenprac00016 0058bM EhabNo ratings yet
- Drug Information HandbookDocument2 pagesDrug Information HandbookSarah NurhalizaNo ratings yet
- DR Eric Brestel's Sep 5 2000 Letter To EditorDocument2 pagesDR Eric Brestel's Sep 5 2000 Letter To EditorRobert Davidson, M.D., Ph.D.No ratings yet
- Glutathione Peroxidase 1 Activity and Cardiovascular Events in Patients With Coronary Artery DiseaseDocument9 pagesGlutathione Peroxidase 1 Activity and Cardiovascular Events in Patients With Coronary Artery Diseaseapi-26034055No ratings yet
- Fuller Albright-Primul Articol de HPPDocument2 pagesFuller Albright-Primul Articol de HPPadelinaNo ratings yet
- Coronary Heart Disease and Physical ActivityDocument12 pagesCoronary Heart Disease and Physical ActivityÁngelNo ratings yet
- Ketamine and Intracranial Pressure: No Contraindication Except HydrocephalusDocument3 pagesKetamine and Intracranial Pressure: No Contraindication Except Hydrocephaluslidwina143No ratings yet
- Ashtma Timeline T2Document21 pagesAshtma Timeline T2ISABEL SOFIA CABARCAS COGOLLONo ratings yet
- Trauma Brain Injury 2Document2 pagesTrauma Brain Injury 2lala putriNo ratings yet
- Pleural Disease During Treatment With Bromocriptine in Patients Previously Exposed To AsbestosDocument6 pagesPleural Disease During Treatment With Bromocriptine in Patients Previously Exposed To Asbestosgarberer1No ratings yet
- PR 1993752Document4 pagesPR 1993752Verónica UriósteguiNo ratings yet
- Spontaneous Breathing During Mechanical Ventilation: A Two-Edged SwordDocument2 pagesSpontaneous Breathing During Mechanical Ventilation: A Two-Edged SwordKhanh Ha NguyenNo ratings yet
- PG 0063Document1 pagePG 0063Leah TigersNo ratings yet
- Unusual Cause of Neonatal Cyanosis: Journal of The Saudi Heart AssociationDocument3 pagesUnusual Cause of Neonatal Cyanosis: Journal of The Saudi Heart AssociationfikaNo ratings yet
- Treatment of Bronchospasm During Anesthesia .28Document4 pagesTreatment of Bronchospasm During Anesthesia .28Anish H DaveNo ratings yet
- Iron Overload and Hepatic Fibrosis in Response - JMDocument1 pageIron Overload and Hepatic Fibrosis in Response - JMBastomy EkaNo ratings yet
- MC Sparr On 2016Document10 pagesMC Sparr On 2016Matias FlammNo ratings yet
- Drug Information HandbookDocument1 pageDrug Information Handbookwulansari nurjanahNo ratings yet
- Aroxysmal Atrial Tachycardia With Atrioventricular BlockDocument7 pagesAroxysmal Atrial Tachycardia With Atrioventricular BlockDenisseRangelNo ratings yet
- New Classification of Stroke: Preliminary Communication: Mmol/lDocument3 pagesNew Classification of Stroke: Preliminary Communication: Mmol/lBella CoritaNo ratings yet
- Bronchial Asthma Research PaperDocument6 pagesBronchial Asthma Research Paperniisexgkf100% (1)
- Caso Clinico Fiebre GlandularDocument3 pagesCaso Clinico Fiebre GlandularJoana L. BauNo ratings yet
- Aair 2 165Document7 pagesAair 2 165HeheebNo ratings yet
- The Cold Water Cure As Practised by Vincent PriessnitzDocument144 pagesThe Cold Water Cure As Practised by Vincent PriessnitzDaz100% (1)
- Overview of Common Causes of Chronic Cough: ACCP Evidence-Based Clinical Practice GuidelinesDocument4 pagesOverview of Common Causes of Chronic Cough: ACCP Evidence-Based Clinical Practice GuidelineschuckyonfireNo ratings yet
- ACE Inhibitors and Abdominal Aortic AneurysmDocument2 pagesACE Inhibitors and Abdominal Aortic Aneurysmvfd08051996No ratings yet
- Penting PIIS0016508597004976Document5 pagesPenting PIIS0016508597004976afifahridhahumairahhNo ratings yet
- Prosiding Pertemuan IlmiahDocument5 pagesProsiding Pertemuan IlmiahVic CullundNo ratings yet
- Double Blind Evaluation of Verapamil, Propranolol and Isosorbide Dinitrate Against A Placebo in The Treatment of Angina PectorisDocument4 pagesDouble Blind Evaluation of Verapamil, Propranolol and Isosorbide Dinitrate Against A Placebo in The Treatment of Angina PectorisLoverz BeebzNo ratings yet
- Should We Question If Something Works Just Because We Don't Know How It Works?Document2 pagesShould We Question If Something Works Just Because We Don't Know How It Works?Liga Medicina InternaNo ratings yet
- E Resp MedDocument2,401 pagesE Resp MedbtaleraNo ratings yet
- Thorax00020 0093Document11 pagesThorax00020 0093Hario Tri HendrokoNo ratings yet
- Brmedj03163 0034Document4 pagesBrmedj03163 0034stevenburrow06No ratings yet
- Jclinpath00023 0077bDocument2 pagesJclinpath00023 0077bChyntia D. RahadiaNo ratings yet
- 527 FullDocument2 pages527 FullRadina RusevaNo ratings yet
- 1. !!!prac. СPRDocument55 pages1. !!!prac. СPRtop theNo ratings yet
- Bedell (1958)Document12 pagesBedell (1958)perceptive.wiseNo ratings yet
- Respiratory Effects of Amyotrophic Lateral Sclerosis, Problems and SolutionsDocument14 pagesRespiratory Effects of Amyotrophic Lateral Sclerosis, Problems and SolutionsMarcelaNo ratings yet
- Tablet 2 PDFDocument64 pagesTablet 2 PDFmaulida hasanahNo ratings yet
- Cardiovascular Eponymic Signs: Diagnostic Skills Applied During the Physical ExaminationFrom EverandCardiovascular Eponymic Signs: Diagnostic Skills Applied During the Physical ExaminationNo ratings yet
- The Pituitary Gland, Volume 1: Anterior PituitaryFrom EverandThe Pituitary Gland, Volume 1: Anterior PituitaryG. W. HarrisNo ratings yet
- Physick to Physiology: Tales from an Oxford Life in MedicineFrom EverandPhysick to Physiology: Tales from an Oxford Life in MedicineNo ratings yet
- BS 03900 0 2010Document26 pagesBS 03900 0 2010selvaNo ratings yet
- 3b Domestic Water Meter Installation in Meter Room GuidelinesDocument10 pages3b Domestic Water Meter Installation in Meter Room GuidelinesVinish HARIDAS NAIRNo ratings yet
- Calibration Curve Between Pressure Drop and Mass Flow RateDocument2 pagesCalibration Curve Between Pressure Drop and Mass Flow RateMikail IsmailNo ratings yet
- Pia Calabarzon 7 Prs (April 12,15, 2013), Dispatch For April 15, 2013 (Monday)Document34 pagesPia Calabarzon 7 Prs (April 12,15, 2013), Dispatch For April 15, 2013 (Monday)Pia QuezonNo ratings yet
- Polynomial FunctionDocument36 pagesPolynomial FunctionfaithreignNo ratings yet
- To Study Well Design Aspects in HPHT EnvironmentDocument40 pagesTo Study Well Design Aspects in HPHT Environmentnikhil_barshettiwat100% (1)
- User S Manual Bedienungsanleitung: Version 1.0 October 1998Document32 pagesUser S Manual Bedienungsanleitung: Version 1.0 October 1998Ojit QuizonNo ratings yet
- Homework 2 SolutionDocument5 pagesHomework 2 SolutiongretabunciNo ratings yet
- Tutorial L298N Driver MotorDocument5 pagesTutorial L298N Driver MotorHairul Anam SNo ratings yet
- Australian Standard: Roof TilesDocument10 pagesAustralian Standard: Roof TilesVeetoau Joseph100% (1)
- Maun StreamDocument22 pagesMaun StreamPrasanth ReddyNo ratings yet
- Life On MarsDocument3 pagesLife On MarsSahar SmNo ratings yet
- Substation Construction and CommissioningDocument83 pagesSubstation Construction and CommissioningShung Tak ChanNo ratings yet
- Mathematics ECAT (Sir Nasim Zulfiqar) - 1Document134 pagesMathematics ECAT (Sir Nasim Zulfiqar) - 1AYESH qureshiNo ratings yet
- Lesson 6 Solving Rational Equations and InequalitiesDocument80 pagesLesson 6 Solving Rational Equations and InequalitiesCarbon Copy0% (1)
- Hydrodynamic Characteristics of The Kort-Nozzle Propeller by Different Turbulence ModelsDocument4 pagesHydrodynamic Characteristics of The Kort-Nozzle Propeller by Different Turbulence ModelstafocanNo ratings yet
- GO Price - escalation.GO - Ms.124.2007Document3 pagesGO Price - escalation.GO - Ms.124.2007hussainNo ratings yet
- Ielts Writing Tu NoiDocument7 pagesIelts Writing Tu NoiQuang Anh TốngNo ratings yet
- Drugs For Chemical EngineeringDocument34 pagesDrugs For Chemical Engineeringshivakumar hrNo ratings yet
- Techniques For Collection, Isolation and Preservation of MicroorganismsDocument42 pagesTechniques For Collection, Isolation and Preservation of Microorganismsaziskf100% (2)
- Lung Sounds Auscultation - 1Document3 pagesLung Sounds Auscultation - 1George BarajazNo ratings yet
- 2010 PriusDocument5 pages2010 PriusNext Day Design -Glassco Global LLCNo ratings yet
- FMEDA E3 ModulevelDocument21 pagesFMEDA E3 ModulevelRonny AjaNo ratings yet
- Indra Motion MLC - Trainning Manual PDFDocument36 pagesIndra Motion MLC - Trainning Manual PDFjorfleitasNo ratings yet
- Singer 291U1, U3Document46 pagesSinger 291U1, U3Datum VivelacriqueNo ratings yet
- Aquaculture Aeration ModulesDocument7 pagesAquaculture Aeration ModulesecosafeNo ratings yet
- 33 1rv18cv119 Umar BashirDocument10 pages33 1rv18cv119 Umar BashirUMARNo ratings yet
- Forensic Syllabus@Document6 pagesForensic Syllabus@YocobSamandrewsNo ratings yet