Download as docx, pdf, or txt
You might also like
- Nursing Care Plan ON: Caesarean DeliveryDocument22 pagesNursing Care Plan ON: Caesarean DeliveryKavi rajput79% (14)
- January 2014: Occupational English TestDocument40 pagesJanuary 2014: Occupational English TestNLNo ratings yet
- General Information:: Sta. Ana Hospital Department of Rehabilitation Medicine Physical Therapy SectionDocument13 pagesGeneral Information:: Sta. Ana Hospital Department of Rehabilitation Medicine Physical Therapy SectionOlenFuerteNo ratings yet
- Neuro Ii SGD 2 PDFDocument8 pagesNeuro Ii SGD 2 PDFRichelle IgnacioNo ratings yet
- Step 2 NotesDocument202 pagesStep 2 NotesNaved Rahman100% (2)
- OB Report Jerrold AguilaDocument42 pagesOB Report Jerrold Aguilaafreenbegum-0502No ratings yet
- Grand Case Presentation Group 1A Pedia PSHDocument70 pagesGrand Case Presentation Group 1A Pedia PSHAla'a Emerald AguamNo ratings yet
- Case Study On Placenta PreviaDocument19 pagesCase Study On Placenta PreviagherlethrNo ratings yet
- Grand Conference: Clinical Clerks Openiano, Oquendo, Pasaporte, PangandianDocument65 pagesGrand Conference: Clinical Clerks Openiano, Oquendo, Pasaporte, PangandianJessa MeaNo ratings yet
- Endorsement BB TDocument27 pagesEndorsement BB TToni Marie Haro ChavezNo ratings yet
- Case Presentation: - Vuppu BhavaniDocument53 pagesCase Presentation: - Vuppu BhavaniLohith Kumar MenchuNo ratings yet
- Pedia Clinics Sample HX PEDocument6 pagesPedia Clinics Sample HX PEJim Christian EllaserNo ratings yet
- Sample Obg Case SheetDocument10 pagesSample Obg Case SheetKamil AlchalisNo ratings yet
- CWU 2 Spinal Fracture PolytraumaDocument19 pagesCWU 2 Spinal Fracture PolytraumaHana FauziNo ratings yet
- Case Presentation Febrile Seizure: Supervisor: Dr. Ulynar Marpaung, Sp.A Created By: Bening Irhamna (1102013057)Document47 pagesCase Presentation Febrile Seizure: Supervisor: Dr. Ulynar Marpaung, Sp.A Created By: Bening Irhamna (1102013057)Bening IrhamnaNo ratings yet
- Care Plan BRAIN TUMORDocument16 pagesCare Plan BRAIN TUMORELISION OFFICIALNo ratings yet
- Case Write Up MedicineDocument16 pagesCase Write Up MedicineKamogelo MabotjaNo ratings yet
- Case Presentation: Yousef Hassan Basman BazarDocument76 pagesCase Presentation: Yousef Hassan Basman BazarYousef Hassan BazarNo ratings yet
- Block 7 Active Phase 1st Stage of LaborDocument29 pagesBlock 7 Active Phase 1st Stage of LaborRoselle Joy D. RosalejosNo ratings yet
- AGN 3B FinalDocument37 pagesAGN 3B FinalKristine Dela CruzNo ratings yet
- Cardio Case Report:: Kawasaki DiseaseDocument53 pagesCardio Case Report:: Kawasaki Diseasemhegan07No ratings yet
- Case Study On Meninomyocele (Repaired) PDocument29 pagesCase Study On Meninomyocele (Repaired) Pcharanjit kaur100% (1)
- Acute (1) 3Document56 pagesAcute (1) 3sivabharathijeyapaulNo ratings yet
- Pediatric AGE EditedDocument4 pagesPediatric AGE EditedMichael VillavertNo ratings yet
- OB GYN CasePre FinalDocument82 pagesOB GYN CasePre FinalMarjorie Lahaylahay AlabataNo ratings yet
- Chapter 3Document40 pagesChapter 3hengkihanggaraNo ratings yet
- Clinical Presentation On AppendicectomyDocument30 pagesClinical Presentation On AppendicectomyValarmathiNo ratings yet
- Pre-Eclampsia Case StudyDocument22 pagesPre-Eclampsia Case StudySusmita SenNo ratings yet
- Lapjag 10 Maret 19Document2 pagesLapjag 10 Maret 19Bernardo Daniel LawrenciusNo ratings yet
- Clinicopathologic Conference: Governor Celestino Gallares Memorial Hospital Department of Obstetrics and GynecologyDocument57 pagesClinicopathologic Conference: Governor Celestino Gallares Memorial Hospital Department of Obstetrics and GynecologyramwshNo ratings yet
- An RH IncompactibilityDocument34 pagesAn RH IncompactibilityValarmathi100% (2)
- ASKEP BBLR HannaningrumDocument12 pagesASKEP BBLR HannaningrumAnnisNo ratings yet
- Pregnant Woman Emergency Clinical CaseDocument38 pagesPregnant Woman Emergency Clinical CaseBianca Gallardo AriasNo ratings yet
- Lapjag 19 Maret 19Document6 pagesLapjag 19 Maret 19Bernardo Daniel LawrenciusNo ratings yet
- Case Presentati On: Sevilla, Loreanne Novem Silim, Miriam Grace DDocument18 pagesCase Presentati On: Sevilla, Loreanne Novem Silim, Miriam Grace DKen StarNo ratings yet
- Neonatal CareplanDocument12 pagesNeonatal Careplanjinsi georgeNo ratings yet
- Case Report DHF FadhilDocument49 pagesCase Report DHF FadhilPashëm IndonesiaNo ratings yet
- Lower Limb WeaknessDocument15 pagesLower Limb WeaknessA MNo ratings yet
- Ob Case 3 ChartDocument6 pagesOb Case 3 ChartSteffiNo ratings yet
- Clinical Case: Csu Junior InternsDocument82 pagesClinical Case: Csu Junior InternsAlexious Marie CalluengNo ratings yet
- Cwu O&g 1 PPROMDocument13 pagesCwu O&g 1 PPROMFaris Mohd Nasir100% (1)
- Acute Appendicitis 3Document8 pagesAcute Appendicitis 3Aiman ArifinNo ratings yet
- CMC Abruptio PlacentaDocument76 pagesCMC Abruptio PlacentaNorman Vryne CaduaNo ratings yet
- Case Presentation Acute GlomerulonephritisDocument10 pagesCase Presentation Acute Glomerulonephritisminangsung minangnengNo ratings yet
- Breakthrough SeizuresDocument13 pagesBreakthrough SeizuresAiman ArifinNo ratings yet
- APPENDICITISDocument69 pagesAPPENDICITISKim Alvarez100% (1)
- Cholelithiasis AnpDocument32 pagesCholelithiasis AnpSuchitaNo ratings yet
- NCP On Low Birth WeightDocument22 pagesNCP On Low Birth Weightbasithere6No ratings yet
- ANC CASE (Revised)Document32 pagesANC CASE (Revised)Mike RossNo ratings yet
- Dengue Fever (A90) + Nosocomial Condition (Y95) : Case ReportDocument22 pagesDengue Fever (A90) + Nosocomial Condition (Y95) : Case ReportMafisahNo ratings yet
- EN - Vita Pramatasari (Rev Miss Aini)Document20 pagesEN - Vita Pramatasari (Rev Miss Aini)Hendra WardhanaNo ratings yet
- Neurology Case ConferenceDocument64 pagesNeurology Case ConferenceAnonymous HH3c17osNo ratings yet
- 6 POSTNATAL Case - Book Rupi - OBS p367-534Document168 pages6 POSTNATAL Case - Book Rupi - OBS p367-534piyush0751100% (1)
- Successful Pregnancy in A Woman With Chronic Kidney Disease Due Toautosomal Polycystic Disease A Case Report 2161 0932 1000338Document5 pagesSuccessful Pregnancy in A Woman With Chronic Kidney Disease Due Toautosomal Polycystic Disease A Case Report 2161 0932 1000338HD RSRNo ratings yet
- All Cases: - Name/Age/Sex/Address Outcome Diagnosis - X/2 yo/F/Bantul Estela 1A Aplastic AnemiaDocument20 pagesAll Cases: - Name/Age/Sex/Address Outcome Diagnosis - X/2 yo/F/Bantul Estela 1A Aplastic AnemiaSeptinaAyuSamsiatiNo ratings yet
- Case Study For OligohydramniosDocument8 pagesCase Study For OligohydramniosKinjal Vasava100% (1)
- Case DonyDocument17 pagesCase Donymuhamad donyNo ratings yet
- II. AssessmentDocument13 pagesII. AssessmentIan Mizzel A. DulfinaNo ratings yet
- Long Case - Susilowati (En Lokal)Document17 pagesLong Case - Susilowati (En Lokal)Hendra WardhanaNo ratings yet
- Small Group Discussion NSDDocument96 pagesSmall Group Discussion NSDKittidej KaewruangNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- EAPP Finals Thesis StatementDocument19 pagesEAPP Finals Thesis StatementUriel MapatacNo ratings yet
- Paediatric TracheostomyDocument13 pagesPaediatric TracheostomyYwagar YwagarNo ratings yet
- Marijuana Facts For TeensDocument23 pagesMarijuana Facts For Teensneeraj_prajapati_16No ratings yet
- Arrhythmogenic CardiomyopathyDocument218 pagesArrhythmogenic CardiomyopathyAntonella SabatiniNo ratings yet
- Treatment of SepsisDocument52 pagesTreatment of SepsisUmmulAklaNo ratings yet
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDocument10 pagesConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoNo ratings yet
- A Chance in Hell Part 3 - Blood and GritDocument5 pagesA Chance in Hell Part 3 - Blood and GritkenthepaNo ratings yet
- Haematology Physical AssessmentDocument26 pagesHaematology Physical AssessmentMarium Mohamed Ali100% (1)
- Sans 1921-6-2004Document11 pagesSans 1921-6-2004lenouteutuNo ratings yet
- Introduction To Electro TherapyDocument55 pagesIntroduction To Electro TherapyHema Malani Murthi82% (11)
- Lyceum-Northwestern UniversityDocument9 pagesLyceum-Northwestern UniversityGwyneth PastorNo ratings yet
- Substance Use Disorders in Children and AdolescentsDocument21 pagesSubstance Use Disorders in Children and AdolescentsagelvezonNo ratings yet
- Second AnnouncementDocument27 pagesSecond AnnouncementSheila FebrianaNo ratings yet
- Fever With Rash Atlas PDFDocument14 pagesFever With Rash Atlas PDFK C Goutham ReddyNo ratings yet
- Oet Writing Nurse 4Document2 pagesOet Writing Nurse 4Janine Joson SalvaniaNo ratings yet
- Johnson Samantha HLTH 3420 Teaching Plan Template 1Document7 pagesJohnson Samantha HLTH 3420 Teaching Plan Template 1api-329945753No ratings yet
- A Study To Assess The Effectiveness of Fenugreek Water To Reduce Blood Glucose Levels Among Clients With Diabetes MellitusDocument5 pagesA Study To Assess The Effectiveness of Fenugreek Water To Reduce Blood Glucose Levels Among Clients With Diabetes MellitusEditor IJTSRDNo ratings yet
- Artigo Bad SplitDocument6 pagesArtigo Bad SplitCarolinaNo ratings yet
- Abscess of THE PeriodontiumDocument57 pagesAbscess of THE PeriodontiumSandeep SunilNo ratings yet
- What Is Acute BronchitisDocument11 pagesWhat Is Acute BronchitisKerri-DojhnHallNo ratings yet
- Death by Heroin Intoxication in A Body Pusher WithDocument7 pagesDeath by Heroin Intoxication in A Body Pusher WithRuben_Monroy_ClaudioNo ratings yet
- الاسهال البكتيري الحادDocument11 pagesالاسهال البكتيري الحادsultan mansoubNo ratings yet
- Alvarez Post Tib Dysfunction Managed With OrthosisDocument7 pagesAlvarez Post Tib Dysfunction Managed With OrthosisChar LeeNo ratings yet
- 3 Year: Punjab Nurses Registration Council SAS Nagar, Mohali Dated: 17.01.2023Document2 pages3 Year: Punjab Nurses Registration Council SAS Nagar, Mohali Dated: 17.01.2023innocent girlNo ratings yet
- BLS ExamDocument4 pagesBLS ExammanalgalmutairiNo ratings yet
- Coleus Blumei (Mayana) Is One of The Traditionally Used Folkloric Medicine and Is Primarily Used For Pain, SoreDocument2 pagesColeus Blumei (Mayana) Is One of The Traditionally Used Folkloric Medicine and Is Primarily Used For Pain, SoreMia Pearl Tabios ValenzuelaNo ratings yet
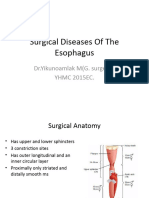
- Surgical Diseases of The EsophagusDocument35 pagesSurgical Diseases of The Esophagusmogesie1995No ratings yet
- Concise DermatologyDocument279 pagesConcise DermatologyVivtor Silva100% (2)
- Types of Drug Information Resources - EditedDocument122 pagesTypes of Drug Information Resources - EditedGammachuu Leejjiisa Mul'ataa SabbooqaaNo ratings yet