
CVS - Physio
CVS - Physio
You might also like
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
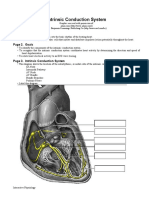
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- Mizuho Vascular (Transcranial) DopplerDocument4 pagesMizuho Vascular (Transcranial) DopplersigmakarsaNo ratings yet
- Detailed Lesson PlanDocument48 pagesDetailed Lesson PlanNaisy Magalona100% (2)
- AP 2 PCW #3 - Cardiovascular - Module 3.7-3.10Document6 pagesAP 2 PCW #3 - Cardiovascular - Module 3.7-3.10eemma.pokemonNo ratings yet
- Permanent PacemakerDocument24 pagesPermanent PacemakerAwais PanhwarNo ratings yet
- Cardiac Muscle PhysiologyDocument4 pagesCardiac Muscle PhysiologyRenatoCosmeGalvanJuniorNo ratings yet
- UPDATED Lesson Guide Dysrhythmias .Docx 118ADocument21 pagesUPDATED Lesson Guide Dysrhythmias .Docx 118ARiri MiguelNo ratings yet
- Sistem KV - PPT (Document121 pagesSistem KV - PPT (Bio Rizki MaulanaNo ratings yet
- Diaphragm + Abdominal Aorta + IVC + LiverDocument2 pagesDiaphragm + Abdominal Aorta + IVC + LiverannaNo ratings yet
- Properties of Heart MusclesDocument11 pagesProperties of Heart MusclesSyedzulqurnainhussainshah ZulqurnainNo ratings yet
- NURS220 - Lect 1-Heart and CirculationDocument36 pagesNURS220 - Lect 1-Heart and Circulation6133858No ratings yet
- CH 11 Heart NotesDocument2 pagesCH 11 Heart Notesummnicole0% (1)
- AP 2 PCW #2 - Cardiovascular - Module 3.3-3.6Document4 pagesAP 2 PCW #2 - Cardiovascular - Module 3.3-3.6eemma.pokemonNo ratings yet
- PHYS150 Tutorial 2 - Cardiovascular SystemDocument68 pagesPHYS150 Tutorial 2 - Cardiovascular Systemsamreenkaur1196No ratings yet
- Cardiac Conduction System Power Point PresentationDocument30 pagesCardiac Conduction System Power Point PresentationAaya AdelNo ratings yet
- Cardiac Muscle: Dr. Kanimozhi Sadasivam, MD Associate Professor SRM Medical College & RC, ChennaiDocument57 pagesCardiac Muscle: Dr. Kanimozhi Sadasivam, MD Associate Professor SRM Medical College & RC, ChennaiShampa SenNo ratings yet
- IV - Cardiovascular SystemDocument3 pagesIV - Cardiovascular SystemGael QuingNo ratings yet
- Cardiovascular PhysiologyDocument287 pagesCardiovascular Physiologyarshamboss4No ratings yet
- CV ED Sem 2 2020 2021Document43 pagesCV ED Sem 2 2020 2021Sarhan AliNo ratings yet
- ANAT 1053 Unit 1 Cardiovascular System, Part II Lecture Slides Prof September 2021Document59 pagesANAT 1053 Unit 1 Cardiovascular System, Part II Lecture Slides Prof September 2021kaitlin.k.woodwardNo ratings yet
- RBM1528 Session 2 2023Document42 pagesRBM1528 Session 2 2023shlokNo ratings yet
- Sistem Konduksi Jantung (Pembekalan) - DR PUT&DrHARDocument32 pagesSistem Konduksi Jantung (Pembekalan) - DR PUT&DrHARNur FarinahNo ratings yet
- The Heart BasicsDocument13 pagesThe Heart BasicsMegan DNo ratings yet
- Understanding EKG's: Avant Healthcare ProfessionalsDocument20 pagesUnderstanding EKG's: Avant Healthcare ProfessionalsmarshaNo ratings yet
- Dysrythmia Review For Pre TestDocument29 pagesDysrythmia Review For Pre TestGeena sekhonNo ratings yet
- PHYSIO Cardiac Muscle and Heart As A PumpDocument5 pagesPHYSIO Cardiac Muscle and Heart As A PumpAyumi StarNo ratings yet
- Electrical Activity of Heart CellsDocument37 pagesElectrical Activity of Heart Cellsspdharanimaran001No ratings yet
- Initiation and Propagation of Cardiac ImpulseDocument110 pagesInitiation and Propagation of Cardiac Impulsedavid mullingsNo ratings yet
- HPP Lec Cvs2Document4 pagesHPP Lec Cvs2carlo baculiNo ratings yet
- BLG111 Week2 Blood Heart 2Document74 pagesBLG111 Week2 Blood Heart 2phuongphuonganhanh171203No ratings yet
- Ilovepdf MergedDocument61 pagesIlovepdf MergedChidrup MannaNo ratings yet
- FA 2019 CardiovascularDocument44 pagesFA 2019 CardiovascularLexNo ratings yet
- 9 ThyroidDocument3 pages9 Thyroidfekid37444No ratings yet
- HEART SimplifiedDocument94 pagesHEART Simplifiedcloud kumoishNo ratings yet
- Cardiology Ebook Notes PDFDocument26 pagesCardiology Ebook Notes PDFsugisweNo ratings yet
- Electrocardiogram A5Document18 pagesElectrocardiogram A5FrancheskaNo ratings yet
- Transes - Heart and Neck VesselsDocument5 pagesTranses - Heart and Neck VesselscamatoviancaNo ratings yet
- Guyton Hall PHYSIOLOGY Chapter 9 PDFDocument8 pagesGuyton Hall PHYSIOLOGY Chapter 9 PDFOsman NazirNo ratings yet
- Lifs1902 11 5Document36 pagesLifs1902 11 5Gary TsangNo ratings yet
- N5 SampleDocument12 pagesN5 Sampleshaikhbakhtiyar3669No ratings yet
- SB0024 Transport in Animals and Plant (DFN)Document80 pagesSB0024 Transport in Animals and Plant (DFN)jmyphjmrdnNo ratings yet
- CH13 BLOOD-VESSELS ByissaDocument8 pagesCH13 BLOOD-VESSELS ByissaRoeisa SalinasNo ratings yet
- Dharani DharanDocument29 pagesDharani Dharanspdharanimaran001No ratings yet
- Introduction To ECGs DoctorialsDocument36 pagesIntroduction To ECGs DoctorialsJaimie Charlotte Marie LangilleNo ratings yet
- Cardio PhysioDocument11 pagesCardio Physioanonymousperson4696No ratings yet
- The Heart Functions As A Pump. How Is The Pump Action Controlled by Regulated Waves of Cell-Cell Depolarization Within The Pump? 2/4Document12 pagesThe Heart Functions As A Pump. How Is The Pump Action Controlled by Regulated Waves of Cell-Cell Depolarization Within The Pump? 2/4tohungthuyNo ratings yet
- Cardiac NursingDocument26 pagesCardiac Nursingjgcriste95% (20)
- Faculty of Medicine: Course Code: BMS 201 Lab 12Document26 pagesFaculty of Medicine: Course Code: BMS 201 Lab 12Rowaa SamehNo ratings yet
- ElectrocardiogramDocument2 pagesElectrocardiogramonijinoNo ratings yet
- Congestive Cardiac Failure PDFDocument28 pagesCongestive Cardiac Failure PDFNANDHINI S100% (1)
- Or Cardiac Physiology, Pathophysiology, and Some PharmacologyDocument58 pagesOr Cardiac Physiology, Pathophysiology, and Some PharmacologyJacob StoneNo ratings yet
- Vsp-Ug-4 (CVS)Document96 pagesVsp-Ug-4 (CVS)6qhx62pr42No ratings yet
- Physiology Worksheet Chapter Five: Cardiovascular SystemDocument2 pagesPhysiology Worksheet Chapter Five: Cardiovascular SystemTalya DannawiNo ratings yet
- 5 - The Cardiovascular System 1Document48 pages5 - The Cardiovascular System 1ManarNo ratings yet
- Estimulação Transcutânea Não InvasivaDocument10 pagesEstimulação Transcutânea Não InvasivaMarcos AcioliNo ratings yet
- Summary of Chris Case, Dr. John Mandrola & Lennard Zinn's The Haywire HeartFrom EverandSummary of Chris Case, Dr. John Mandrola & Lennard Zinn's The Haywire HeartNo ratings yet
- IELTS Academic Training Reading Practice Test #7. An Example Exam for You to Practise in Your Spare TimeFrom EverandIELTS Academic Training Reading Practice Test #7. An Example Exam for You to Practise in Your Spare TimeRating: 2 out of 5 stars2/5 (1)
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Animal TissuesDocument55 pagesAnimal TissuesFarah AljayyousiNo ratings yet
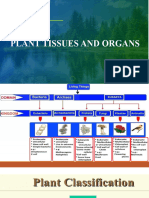
- Plant Tissues and OrgansDocument47 pagesPlant Tissues and OrgansFarah AljayyousiNo ratings yet
- Mitosis and MeiosisDocument31 pagesMitosis and MeiosisFarah AljayyousiNo ratings yet
- MCQ On Endocrine System 5eea6a0c39140f30f369e04bDocument23 pagesMCQ On Endocrine System 5eea6a0c39140f30f369e04bFarah AljayyousiNo ratings yet
- 2 - Chapter02 - Basic Elements of C++Document74 pages2 - Chapter02 - Basic Elements of C++Farah AljayyousiNo ratings yet
- L3Q Physio MergedDocument4 pagesL3Q Physio MergedFarah AljayyousiNo ratings yet
- Mid Eng - Nisrin Fall 2022 by MomaniDocument1 pageMid Eng - Nisrin Fall 2022 by MomaniFarah AljayyousiNo ratings yet
- Mid Physioanatomy Lab - 2020Document35 pagesMid Physioanatomy Lab - 2020Farah AljayyousiNo ratings yet
- Anthropometry (Part1)Document11 pagesAnthropometry (Part1)Farah AljayyousiNo ratings yet
- 2 - AtherosclerosisDocument16 pages2 - AtherosclerosisUnnati PatelNo ratings yet
- Adjustment To Extra Uterine LifeDocument51 pagesAdjustment To Extra Uterine LifeJagadeeswari JayaseelanNo ratings yet
- Transfer Factor CardioDocument2 pagesTransfer Factor CardioGB R100% (1)
- Pentoxifylline in The Treatment of Pathological PDFDocument8 pagesPentoxifylline in The Treatment of Pathological PDFAndreas SmfNo ratings yet
- Gesc 107Document12 pagesGesc 107Nippu SharmaNo ratings yet
- Applied Respiratory PhysiologyDocument4 pagesApplied Respiratory PhysiologyMitul JainNo ratings yet
- Lab 9-10 Mesenchymal Tumours. MM TeratomasDocument65 pagesLab 9-10 Mesenchymal Tumours. MM TeratomasZaccaria KhawatmiNo ratings yet
- Blood and Blood Vessels Module 3Document16 pagesBlood and Blood Vessels Module 3Jenevieve Tungcul SimanganNo ratings yet
- Vasoactive Agents For Adult Septic Shock: An Update and ReviewDocument14 pagesVasoactive Agents For Adult Septic Shock: An Update and Reviewjihan muthiNo ratings yet
- Scalar Energy PendantDocument2 pagesScalar Energy PendantNendi PriyatnaNo ratings yet
- Chapter II: When To Use The Milk DietDocument11 pagesChapter II: When To Use The Milk Dietgibrambo5770No ratings yet
- Lesson PlanDocument149 pagesLesson PlanJocelyn GaniaNo ratings yet
- Neurovascular Assessment.... MMMMMDocument7 pagesNeurovascular Assessment.... MMMMMArian May MarcosNo ratings yet
- Heart Gcse Qs OnlyDocument6 pagesHeart Gcse Qs OnlygriggansNo ratings yet
- Nur 111 Session 18 Sas 1Document11 pagesNur 111 Session 18 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- I Microcirculatory DisordersDocument37 pagesI Microcirculatory DisordersMarina ModringaNo ratings yet
- Artifacts PPT OKDocument46 pagesArtifacts PPT OKCharles SiregarNo ratings yet
- DENTEP Desertation FINALDocument83 pagesDENTEP Desertation FINALCESAR NDJOKONo ratings yet
- What Happen When U Quit SmokingDocument2 pagesWhat Happen When U Quit Smokinglook at meNo ratings yet
- 15A ArteryDocument72 pages15A Arterypavi7muruganathanNo ratings yet
- Lower Extremity Arterial Protocol 14 1Document2 pagesLower Extremity Arterial Protocol 14 1api-3494022400% (1)
- Medical Terminology Chapter 1 Practice QuestionsDocument30 pagesMedical Terminology Chapter 1 Practice Questionshtb495No ratings yet
- Strokeaha 116 013650Document7 pagesStrokeaha 116 013650priyaNo ratings yet
- Cambridge IGCSE: Biology 0610/12Document16 pagesCambridge IGCSE: Biology 0610/12Teacher AlexNo ratings yet
- Life Process.Document43 pagesLife Process.Anzar100% (1)
- Circulatory Pt. 1Document10 pagesCirculatory Pt. 1Melvin Razon Espinola Jr.No ratings yet
- The Cardiovascular System: Learning ObjectivesDocument42 pagesThe Cardiovascular System: Learning ObjectivesMuba sonNo ratings yet
- 2019 Raynaud's PhenomenonDocument21 pages2019 Raynaud's PhenomenonGerman Gustavo Salgado TapiaNo ratings yet
































































































Download as pdf or txt
You might also like
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- Mizuho Vascular (Transcranial) DopplerDocument4 pagesMizuho Vascular (Transcranial) DopplersigmakarsaNo ratings yet
- Detailed Lesson PlanDocument48 pagesDetailed Lesson PlanNaisy Magalona100% (2)
- AP 2 PCW #3 - Cardiovascular - Module 3.7-3.10Document6 pagesAP 2 PCW #3 - Cardiovascular - Module 3.7-3.10eemma.pokemonNo ratings yet
- Permanent PacemakerDocument24 pagesPermanent PacemakerAwais PanhwarNo ratings yet
- Cardiac Muscle PhysiologyDocument4 pagesCardiac Muscle PhysiologyRenatoCosmeGalvanJuniorNo ratings yet
- UPDATED Lesson Guide Dysrhythmias .Docx 118ADocument21 pagesUPDATED Lesson Guide Dysrhythmias .Docx 118ARiri MiguelNo ratings yet
- Sistem KV - PPT (Document121 pagesSistem KV - PPT (Bio Rizki MaulanaNo ratings yet
- Diaphragm + Abdominal Aorta + IVC + LiverDocument2 pagesDiaphragm + Abdominal Aorta + IVC + LiverannaNo ratings yet
- Properties of Heart MusclesDocument11 pagesProperties of Heart MusclesSyedzulqurnainhussainshah ZulqurnainNo ratings yet
- NURS220 - Lect 1-Heart and CirculationDocument36 pagesNURS220 - Lect 1-Heart and Circulation6133858No ratings yet
- CH 11 Heart NotesDocument2 pagesCH 11 Heart Notesummnicole0% (1)
- AP 2 PCW #2 - Cardiovascular - Module 3.3-3.6Document4 pagesAP 2 PCW #2 - Cardiovascular - Module 3.3-3.6eemma.pokemonNo ratings yet
- PHYS150 Tutorial 2 - Cardiovascular SystemDocument68 pagesPHYS150 Tutorial 2 - Cardiovascular Systemsamreenkaur1196No ratings yet
- Cardiac Conduction System Power Point PresentationDocument30 pagesCardiac Conduction System Power Point PresentationAaya AdelNo ratings yet
- Cardiac Muscle: Dr. Kanimozhi Sadasivam, MD Associate Professor SRM Medical College & RC, ChennaiDocument57 pagesCardiac Muscle: Dr. Kanimozhi Sadasivam, MD Associate Professor SRM Medical College & RC, ChennaiShampa SenNo ratings yet
- IV - Cardiovascular SystemDocument3 pagesIV - Cardiovascular SystemGael QuingNo ratings yet
- Cardiovascular PhysiologyDocument287 pagesCardiovascular Physiologyarshamboss4No ratings yet
- CV ED Sem 2 2020 2021Document43 pagesCV ED Sem 2 2020 2021Sarhan AliNo ratings yet
- ANAT 1053 Unit 1 Cardiovascular System, Part II Lecture Slides Prof September 2021Document59 pagesANAT 1053 Unit 1 Cardiovascular System, Part II Lecture Slides Prof September 2021kaitlin.k.woodwardNo ratings yet
- RBM1528 Session 2 2023Document42 pagesRBM1528 Session 2 2023shlokNo ratings yet
- Sistem Konduksi Jantung (Pembekalan) - DR PUT&DrHARDocument32 pagesSistem Konduksi Jantung (Pembekalan) - DR PUT&DrHARNur FarinahNo ratings yet
- The Heart BasicsDocument13 pagesThe Heart BasicsMegan DNo ratings yet
- Understanding EKG's: Avant Healthcare ProfessionalsDocument20 pagesUnderstanding EKG's: Avant Healthcare ProfessionalsmarshaNo ratings yet
- Dysrythmia Review For Pre TestDocument29 pagesDysrythmia Review For Pre TestGeena sekhonNo ratings yet
- PHYSIO Cardiac Muscle and Heart As A PumpDocument5 pagesPHYSIO Cardiac Muscle and Heart As A PumpAyumi StarNo ratings yet
- Electrical Activity of Heart CellsDocument37 pagesElectrical Activity of Heart Cellsspdharanimaran001No ratings yet
- Initiation and Propagation of Cardiac ImpulseDocument110 pagesInitiation and Propagation of Cardiac Impulsedavid mullingsNo ratings yet
- HPP Lec Cvs2Document4 pagesHPP Lec Cvs2carlo baculiNo ratings yet
- BLG111 Week2 Blood Heart 2Document74 pagesBLG111 Week2 Blood Heart 2phuongphuonganhanh171203No ratings yet
- Ilovepdf MergedDocument61 pagesIlovepdf MergedChidrup MannaNo ratings yet
- FA 2019 CardiovascularDocument44 pagesFA 2019 CardiovascularLexNo ratings yet
- 9 ThyroidDocument3 pages9 Thyroidfekid37444No ratings yet
- HEART SimplifiedDocument94 pagesHEART Simplifiedcloud kumoishNo ratings yet
- Cardiology Ebook Notes PDFDocument26 pagesCardiology Ebook Notes PDFsugisweNo ratings yet
- Electrocardiogram A5Document18 pagesElectrocardiogram A5FrancheskaNo ratings yet
- Transes - Heart and Neck VesselsDocument5 pagesTranses - Heart and Neck VesselscamatoviancaNo ratings yet
- Guyton Hall PHYSIOLOGY Chapter 9 PDFDocument8 pagesGuyton Hall PHYSIOLOGY Chapter 9 PDFOsman NazirNo ratings yet
- Lifs1902 11 5Document36 pagesLifs1902 11 5Gary TsangNo ratings yet
- N5 SampleDocument12 pagesN5 Sampleshaikhbakhtiyar3669No ratings yet
- SB0024 Transport in Animals and Plant (DFN)Document80 pagesSB0024 Transport in Animals and Plant (DFN)jmyphjmrdnNo ratings yet
- CH13 BLOOD-VESSELS ByissaDocument8 pagesCH13 BLOOD-VESSELS ByissaRoeisa SalinasNo ratings yet
- Dharani DharanDocument29 pagesDharani Dharanspdharanimaran001No ratings yet
- Introduction To ECGs DoctorialsDocument36 pagesIntroduction To ECGs DoctorialsJaimie Charlotte Marie LangilleNo ratings yet
- Cardio PhysioDocument11 pagesCardio Physioanonymousperson4696No ratings yet
- The Heart Functions As A Pump. How Is The Pump Action Controlled by Regulated Waves of Cell-Cell Depolarization Within The Pump? 2/4Document12 pagesThe Heart Functions As A Pump. How Is The Pump Action Controlled by Regulated Waves of Cell-Cell Depolarization Within The Pump? 2/4tohungthuyNo ratings yet
- Cardiac NursingDocument26 pagesCardiac Nursingjgcriste95% (20)
- Faculty of Medicine: Course Code: BMS 201 Lab 12Document26 pagesFaculty of Medicine: Course Code: BMS 201 Lab 12Rowaa SamehNo ratings yet
- ElectrocardiogramDocument2 pagesElectrocardiogramonijinoNo ratings yet
- Congestive Cardiac Failure PDFDocument28 pagesCongestive Cardiac Failure PDFNANDHINI S100% (1)
- Or Cardiac Physiology, Pathophysiology, and Some PharmacologyDocument58 pagesOr Cardiac Physiology, Pathophysiology, and Some PharmacologyJacob StoneNo ratings yet
- Vsp-Ug-4 (CVS)Document96 pagesVsp-Ug-4 (CVS)6qhx62pr42No ratings yet
- Physiology Worksheet Chapter Five: Cardiovascular SystemDocument2 pagesPhysiology Worksheet Chapter Five: Cardiovascular SystemTalya DannawiNo ratings yet
- 5 - The Cardiovascular System 1Document48 pages5 - The Cardiovascular System 1ManarNo ratings yet
- Estimulação Transcutânea Não InvasivaDocument10 pagesEstimulação Transcutânea Não InvasivaMarcos AcioliNo ratings yet
- Summary of Chris Case, Dr. John Mandrola & Lennard Zinn's The Haywire HeartFrom EverandSummary of Chris Case, Dr. John Mandrola & Lennard Zinn's The Haywire HeartNo ratings yet
- IELTS Academic Training Reading Practice Test #7. An Example Exam for You to Practise in Your Spare TimeFrom EverandIELTS Academic Training Reading Practice Test #7. An Example Exam for You to Practise in Your Spare TimeRating: 2 out of 5 stars2/5 (1)
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Animal TissuesDocument55 pagesAnimal TissuesFarah AljayyousiNo ratings yet
- Plant Tissues and OrgansDocument47 pagesPlant Tissues and OrgansFarah AljayyousiNo ratings yet
- Mitosis and MeiosisDocument31 pagesMitosis and MeiosisFarah AljayyousiNo ratings yet
- MCQ On Endocrine System 5eea6a0c39140f30f369e04bDocument23 pagesMCQ On Endocrine System 5eea6a0c39140f30f369e04bFarah AljayyousiNo ratings yet
- 2 - Chapter02 - Basic Elements of C++Document74 pages2 - Chapter02 - Basic Elements of C++Farah AljayyousiNo ratings yet
- L3Q Physio MergedDocument4 pagesL3Q Physio MergedFarah AljayyousiNo ratings yet
- Mid Eng - Nisrin Fall 2022 by MomaniDocument1 pageMid Eng - Nisrin Fall 2022 by MomaniFarah AljayyousiNo ratings yet
- Mid Physioanatomy Lab - 2020Document35 pagesMid Physioanatomy Lab - 2020Farah AljayyousiNo ratings yet
- Anthropometry (Part1)Document11 pagesAnthropometry (Part1)Farah AljayyousiNo ratings yet
- 2 - AtherosclerosisDocument16 pages2 - AtherosclerosisUnnati PatelNo ratings yet
- Adjustment To Extra Uterine LifeDocument51 pagesAdjustment To Extra Uterine LifeJagadeeswari JayaseelanNo ratings yet
- Transfer Factor CardioDocument2 pagesTransfer Factor CardioGB R100% (1)
- Pentoxifylline in The Treatment of Pathological PDFDocument8 pagesPentoxifylline in The Treatment of Pathological PDFAndreas SmfNo ratings yet
- Gesc 107Document12 pagesGesc 107Nippu SharmaNo ratings yet
- Applied Respiratory PhysiologyDocument4 pagesApplied Respiratory PhysiologyMitul JainNo ratings yet
- Lab 9-10 Mesenchymal Tumours. MM TeratomasDocument65 pagesLab 9-10 Mesenchymal Tumours. MM TeratomasZaccaria KhawatmiNo ratings yet
- Blood and Blood Vessels Module 3Document16 pagesBlood and Blood Vessels Module 3Jenevieve Tungcul SimanganNo ratings yet
- Vasoactive Agents For Adult Septic Shock: An Update and ReviewDocument14 pagesVasoactive Agents For Adult Septic Shock: An Update and Reviewjihan muthiNo ratings yet
- Scalar Energy PendantDocument2 pagesScalar Energy PendantNendi PriyatnaNo ratings yet
- Chapter II: When To Use The Milk DietDocument11 pagesChapter II: When To Use The Milk Dietgibrambo5770No ratings yet
- Lesson PlanDocument149 pagesLesson PlanJocelyn GaniaNo ratings yet
- Neurovascular Assessment.... MMMMMDocument7 pagesNeurovascular Assessment.... MMMMMArian May MarcosNo ratings yet
- Heart Gcse Qs OnlyDocument6 pagesHeart Gcse Qs OnlygriggansNo ratings yet
- Nur 111 Session 18 Sas 1Document11 pagesNur 111 Session 18 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- I Microcirculatory DisordersDocument37 pagesI Microcirculatory DisordersMarina ModringaNo ratings yet
- Artifacts PPT OKDocument46 pagesArtifacts PPT OKCharles SiregarNo ratings yet
- DENTEP Desertation FINALDocument83 pagesDENTEP Desertation FINALCESAR NDJOKONo ratings yet
- What Happen When U Quit SmokingDocument2 pagesWhat Happen When U Quit Smokinglook at meNo ratings yet
- 15A ArteryDocument72 pages15A Arterypavi7muruganathanNo ratings yet
- Lower Extremity Arterial Protocol 14 1Document2 pagesLower Extremity Arterial Protocol 14 1api-3494022400% (1)
- Medical Terminology Chapter 1 Practice QuestionsDocument30 pagesMedical Terminology Chapter 1 Practice Questionshtb495No ratings yet
- Strokeaha 116 013650Document7 pagesStrokeaha 116 013650priyaNo ratings yet
- Cambridge IGCSE: Biology 0610/12Document16 pagesCambridge IGCSE: Biology 0610/12Teacher AlexNo ratings yet
- Life Process.Document43 pagesLife Process.Anzar100% (1)
- Circulatory Pt. 1Document10 pagesCirculatory Pt. 1Melvin Razon Espinola Jr.No ratings yet
- The Cardiovascular System: Learning ObjectivesDocument42 pagesThe Cardiovascular System: Learning ObjectivesMuba sonNo ratings yet
- 2019 Raynaud's PhenomenonDocument21 pages2019 Raynaud's PhenomenonGerman Gustavo Salgado TapiaNo ratings yet