
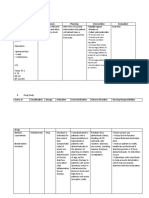
Case-1 On Open Chole
Case-1 On Open Chole
You might also like
- Public Health Law and Ethics: Lecture NoteDocument47 pagesPublic Health Law and Ethics: Lecture Noteabdiqani abdulaahi100% (9)
- Pedia 1Document8 pagesPedia 1Jani MisterioNo ratings yet
- Sample POMRDocument4 pagesSample POMRJeffrey RamosNo ratings yet
- Emailing Ophthalmology - Past Papers SEQS - KMUDocument70 pagesEmailing Ophthalmology - Past Papers SEQS - KMUem khan100% (2)
- Source and Reliability: Informant Is Her Mother With A Reliability of 90%Document3 pagesSource and Reliability: Informant Is Her Mother With A Reliability of 90%Dennis Jr ManguilimotanNo ratings yet
- Week 3 Case - DOBDocument3 pagesWeek 3 Case - DOBKirk Matthew ZhuNo ratings yet
- 病歷教學 20240606Document5 pages病歷教學 20240606u108001951No ratings yet
- IM - Patient Esguera (Final)Document4 pagesIM - Patient Esguera (Final)k.n.e.d.No ratings yet
- IM Gastro FinalDocument10 pagesIM Gastro FinalIzzyMaxinoNo ratings yet
- B6 - Surgery GS II Case IIDocument10 pagesB6 - Surgery GS II Case IIGregNo ratings yet
- Rectal CancerDocument71 pagesRectal CancerGio Balisi100% (2)
- Date and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessDocument3 pagesDate and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessConcepcion R. AquinoNo ratings yet
- FRANCISCO-CMC-with-EBM (Merged)Document12 pagesFRANCISCO-CMC-with-EBM (Merged)Nehemiah FranciscoNo ratings yet
- BPUDDocument26 pagesBPUDIvanNo ratings yet
- Cwu SurgeryDocument16 pagesCwu SurgeryAslah NabilahNo ratings yet
- CaseDocument2 pagesCaseJim Christian EllaserNo ratings yet
- Enterobiasis CaseDocument4 pagesEnterobiasis CaseKimm Delos ReyesNo ratings yet
- Dela Torre Case Presentation South GenDocument44 pagesDela Torre Case Presentation South GenRalph Dale Dela TorreNo ratings yet
- Protocol - IM Cough and DyspneaDocument7 pagesProtocol - IM Cough and DyspneaTrisNo ratings yet
- IM-Generalized Peritonitis HX PEDocument20 pagesIM-Generalized Peritonitis HX PETrisNo ratings yet
- Pediatrics Case PresentationDocument11 pagesPediatrics Case PresentationAishwarya Bharath0% (1)
- Cebu Doctors' University Department of Internal Medicine EndorsementDocument38 pagesCebu Doctors' University Department of Internal Medicine EndorsementRalph de la TorreNo ratings yet
- I. General DataDocument6 pagesI. General Datamadison DeliNo ratings yet
- Case Clerking ApendicDocument15 pagesCase Clerking ApendicMelvin Khung100% (1)
- Case Clerking ApendicDocument15 pagesCase Clerking ApendicChen Cheng0% (1)
- Batmc OrthoDocument5 pagesBatmc OrthoDorish Faith CarilloNo ratings yet
- Pedia 2017 Case ProtocolDocument14 pagesPedia 2017 Case ProtocolArjay Amba0% (1)
- POMRDocument7 pagesPOMRIan RamosNo ratings yet
- Group 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariDocument35 pagesGroup 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariZedd ZorïNo ratings yet
- I. General DataDocument7 pagesI. General Datamadison DeliNo ratings yet
- Bedside OutputDocument5 pagesBedside OutputREGENE KRIS SIMMONE GAMILNo ratings yet
- Clinical Case: Section A - Group 8Document68 pagesClinical Case: Section A - Group 8madison Deli100% (1)
- Thalassemia Report Edited2Document121 pagesThalassemia Report Edited2rjcarlos_05No ratings yet
- Im Precep - Asthma W - PneumoniaDocument63 pagesIm Precep - Asthma W - PneumoniaAoi ShinNo ratings yet
- Acute AppendicitisDocument14 pagesAcute AppendicitisJane GarciaNo ratings yet
- IM-Hx and PE Cough and Dyspnea (CAP)Document34 pagesIM-Hx and PE Cough and Dyspnea (CAP)TrisNo ratings yet
- Case Presentation: Course: EndocrinologyDocument13 pagesCase Presentation: Course: EndocrinologyCalingalan Hussin CaluangNo ratings yet
- Patient History Amang 2Document7 pagesPatient History Amang 2Christine Evan HoNo ratings yet
- Review of SystemsDocument12 pagesReview of SystemseyakoyNo ratings yet
- UNEVERSITATEA DE STAT DE MEDICINA SI FARMACIE New PneumoDocument15 pagesUNEVERSITATEA DE STAT DE MEDICINA SI FARMACIE New PneumoGalina LozovanuNo ratings yet
- I. General DataDocument16 pagesI. General DataJaymart BieNo ratings yet
- De La Salle University Medical Center Department of Obstetrics and GynecologyDocument3 pagesDe La Salle University Medical Center Department of Obstetrics and GynecologyNehemiah FranciscoNo ratings yet
- B6 - Surgery GS II Case 1Document9 pagesB6 - Surgery GS II Case 1GregNo ratings yet
- Case Report: Division ADocument19 pagesCase Report: Division AAyuub AbdirizakNo ratings yet
- Team C Final Written OutputDocument22 pagesTeam C Final Written OutputCarina SuarezNo ratings yet
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocument15 pagesCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNo ratings yet
- Acute GlomerulonephritisDocument85 pagesAcute GlomerulonephritisPunsalan ChecaNo ratings yet
- Case Report II Internal MedicineDocument11 pagesCase Report II Internal MedicineGidu SaidNo ratings yet
- Case Presentation SleDocument33 pagesCase Presentation SleJxyp MundoNo ratings yet
- HIVCase Report II Internal MedicineDocument12 pagesHIVCase Report II Internal Medicineaxmedfare138No ratings yet
- APPENDICITISDocument69 pagesAPPENDICITISKim Alvarez100% (1)
- LinksDocument24 pagesLinksTrisNo ratings yet
- Admission Conference: Ernesto V. Ignacio JRDocument17 pagesAdmission Conference: Ernesto V. Ignacio JRernignacioNo ratings yet
- Chronic Obstructive PulmonaryDocument28 pagesChronic Obstructive PulmonaryAyu Sulung NariratriNo ratings yet
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDocument10 pagesConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoNo ratings yet
- Clinical Case PresentationDocument44 pagesClinical Case PresentationRUSSELL CILOTNo ratings yet
- History 1Document11 pagesHistory 1KaleabNo ratings yet
- Clinicopathologic Case Conference: Department of Family MedicineDocument39 pagesClinicopathologic Case Conference: Department of Family MedicineRaq KhoNo ratings yet
- Sample POMRDocument4 pagesSample POMRJeffrey RamosNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Skizofrenia (Pak Cecep)Document30 pagesSkizofrenia (Pak Cecep)Nurul SafitriNo ratings yet
- 409-Article Text-1439-1-10-20211018Document12 pages409-Article Text-1439-1-10-20211018Anonymous a2nxIq5No ratings yet
- Chemotherapy Administration in Pediatric: An OverviewDocument76 pagesChemotherapy Administration in Pediatric: An OverviewMiftaa HurrahmiNo ratings yet
- Indwelling CatheterDocument6 pagesIndwelling Cathetereloiza custodioNo ratings yet
- Prospectus New India Asha Kiran PolicyDocument17 pagesProspectus New India Asha Kiran PolicySHYLAJA DNo ratings yet
- Atlas of Retinal OCT 2nd EditionDocument480 pagesAtlas of Retinal OCT 2nd EditionSisoesNo ratings yet
- Osteoarthritis and Joint Diseases 2023Document29 pagesOsteoarthritis and Joint Diseases 2023Abdullah MelhimNo ratings yet
- I. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationDocument3 pagesI. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationCherubim Lei DC FloresNo ratings yet
- Preeclampsia Case StudyDocument13 pagesPreeclampsia Case StudyBiway RegalaNo ratings yet
- Louis Kuhne Facial Diagnosis 1897 02 PDFDocument105 pagesLouis Kuhne Facial Diagnosis 1897 02 PDFJosé BitarNo ratings yet
- Stem Cells and Their ApplicationDocument16 pagesStem Cells and Their ApplicationRam Kewal TripathiNo ratings yet
- 22.52 Social Determinants of HealthUK and The Local Government - 05 - 0Document26 pages22.52 Social Determinants of HealthUK and The Local Government - 05 - 0lesleyNo ratings yet
- NCP Outpatient Diagnosis Made EasierDocument19 pagesNCP Outpatient Diagnosis Made EasiertapallajanicaNo ratings yet
- Study PlanDocument4 pagesStudy PlanKeshab RijalNo ratings yet
- The Effect of Music On Auditory Hallucination and Quality of Life in Schizophrenic Patients: A Randomised Controlled TrialDocument9 pagesThe Effect of Music On Auditory Hallucination and Quality of Life in Schizophrenic Patients: A Randomised Controlled Trialyulia22No ratings yet
- Lect # 2 Care of Patients With Gout and Paget's DiseaseDocument21 pagesLect # 2 Care of Patients With Gout and Paget's DiseaseShayan ShayanNo ratings yet
- Managing Ammonia in Poultry Farms: Effects of Ammonia On BirdsDocument8 pagesManaging Ammonia in Poultry Farms: Effects of Ammonia On Birdsamamùra maamarNo ratings yet
- Emergency Psychiatry Primer On Series 1St Edition Tony Thrasher Editor Full ChapterDocument67 pagesEmergency Psychiatry Primer On Series 1St Edition Tony Thrasher Editor Full Chaptergina.larson159100% (12)
- Homeosiniatry - Combination of Acupuncture and HomeopathyDocument4 pagesHomeosiniatry - Combination of Acupuncture and HomeopathyGold SunriseNo ratings yet
- PNB Claim FormsDocument2 pagesPNB Claim Formssaika tabbasumNo ratings yet
- G.R. No. 193500 Government Service Insurance System, Petitioners SIMEON TAÑEDO, JR., RespondentDocument4 pagesG.R. No. 193500 Government Service Insurance System, Petitioners SIMEON TAÑEDO, JR., RespondentLara DelleNo ratings yet
- Stool Specimen CollectionDocument8 pagesStool Specimen CollectionPraveen KumarNo ratings yet
- RAD RLE Guide - Written Requirements: Patients DataDocument16 pagesRAD RLE Guide - Written Requirements: Patients DataHanniel MontecalboNo ratings yet
- Drug Study (Haloperidol)Document3 pagesDrug Study (Haloperidol)Mae Ann Bueno CastillonNo ratings yet
- Orthopaedic Trauma Lecture Notes MBCHBDocument73 pagesOrthopaedic Trauma Lecture Notes MBCHBjhqmpzg7sjNo ratings yet
- Authorization Approved: Applicant InformationDocument1 pageAuthorization Approved: Applicant Informationnicolle hansenNo ratings yet
- 11-Paroxysmal Nocturnal HaemoglobinuriaDocument6 pages11-Paroxysmal Nocturnal HaemoglobinuriaHamid IqbalNo ratings yet
- Challenging Cases in Neonatology 2018Document388 pagesChallenging Cases in Neonatology 2018Sabera Kapasi100% (1)
























































































Download as pdf or txt
You might also like
- Public Health Law and Ethics: Lecture NoteDocument47 pagesPublic Health Law and Ethics: Lecture Noteabdiqani abdulaahi100% (9)
- Pedia 1Document8 pagesPedia 1Jani MisterioNo ratings yet
- Sample POMRDocument4 pagesSample POMRJeffrey RamosNo ratings yet
- Emailing Ophthalmology - Past Papers SEQS - KMUDocument70 pagesEmailing Ophthalmology - Past Papers SEQS - KMUem khan100% (2)
- Source and Reliability: Informant Is Her Mother With A Reliability of 90%Document3 pagesSource and Reliability: Informant Is Her Mother With A Reliability of 90%Dennis Jr ManguilimotanNo ratings yet
- Week 3 Case - DOBDocument3 pagesWeek 3 Case - DOBKirk Matthew ZhuNo ratings yet
- 病歷教學 20240606Document5 pages病歷教學 20240606u108001951No ratings yet
- IM - Patient Esguera (Final)Document4 pagesIM - Patient Esguera (Final)k.n.e.d.No ratings yet
- IM Gastro FinalDocument10 pagesIM Gastro FinalIzzyMaxinoNo ratings yet
- B6 - Surgery GS II Case IIDocument10 pagesB6 - Surgery GS II Case IIGregNo ratings yet
- Rectal CancerDocument71 pagesRectal CancerGio Balisi100% (2)
- Date and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessDocument3 pagesDate and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessConcepcion R. AquinoNo ratings yet
- FRANCISCO-CMC-with-EBM (Merged)Document12 pagesFRANCISCO-CMC-with-EBM (Merged)Nehemiah FranciscoNo ratings yet
- BPUDDocument26 pagesBPUDIvanNo ratings yet
- Cwu SurgeryDocument16 pagesCwu SurgeryAslah NabilahNo ratings yet
- CaseDocument2 pagesCaseJim Christian EllaserNo ratings yet
- Enterobiasis CaseDocument4 pagesEnterobiasis CaseKimm Delos ReyesNo ratings yet
- Dela Torre Case Presentation South GenDocument44 pagesDela Torre Case Presentation South GenRalph Dale Dela TorreNo ratings yet
- Protocol - IM Cough and DyspneaDocument7 pagesProtocol - IM Cough and DyspneaTrisNo ratings yet
- IM-Generalized Peritonitis HX PEDocument20 pagesIM-Generalized Peritonitis HX PETrisNo ratings yet
- Pediatrics Case PresentationDocument11 pagesPediatrics Case PresentationAishwarya Bharath0% (1)
- Cebu Doctors' University Department of Internal Medicine EndorsementDocument38 pagesCebu Doctors' University Department of Internal Medicine EndorsementRalph de la TorreNo ratings yet
- I. General DataDocument6 pagesI. General Datamadison DeliNo ratings yet
- Case Clerking ApendicDocument15 pagesCase Clerking ApendicMelvin Khung100% (1)
- Case Clerking ApendicDocument15 pagesCase Clerking ApendicChen Cheng0% (1)
- Batmc OrthoDocument5 pagesBatmc OrthoDorish Faith CarilloNo ratings yet
- Pedia 2017 Case ProtocolDocument14 pagesPedia 2017 Case ProtocolArjay Amba0% (1)
- POMRDocument7 pagesPOMRIan RamosNo ratings yet
- Group 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariDocument35 pagesGroup 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariZedd ZorïNo ratings yet
- I. General DataDocument7 pagesI. General Datamadison DeliNo ratings yet
- Bedside OutputDocument5 pagesBedside OutputREGENE KRIS SIMMONE GAMILNo ratings yet
- Clinical Case: Section A - Group 8Document68 pagesClinical Case: Section A - Group 8madison Deli100% (1)
- Thalassemia Report Edited2Document121 pagesThalassemia Report Edited2rjcarlos_05No ratings yet
- Im Precep - Asthma W - PneumoniaDocument63 pagesIm Precep - Asthma W - PneumoniaAoi ShinNo ratings yet
- Acute AppendicitisDocument14 pagesAcute AppendicitisJane GarciaNo ratings yet
- IM-Hx and PE Cough and Dyspnea (CAP)Document34 pagesIM-Hx and PE Cough and Dyspnea (CAP)TrisNo ratings yet
- Case Presentation: Course: EndocrinologyDocument13 pagesCase Presentation: Course: EndocrinologyCalingalan Hussin CaluangNo ratings yet
- Patient History Amang 2Document7 pagesPatient History Amang 2Christine Evan HoNo ratings yet
- Review of SystemsDocument12 pagesReview of SystemseyakoyNo ratings yet
- UNEVERSITATEA DE STAT DE MEDICINA SI FARMACIE New PneumoDocument15 pagesUNEVERSITATEA DE STAT DE MEDICINA SI FARMACIE New PneumoGalina LozovanuNo ratings yet
- I. General DataDocument16 pagesI. General DataJaymart BieNo ratings yet
- De La Salle University Medical Center Department of Obstetrics and GynecologyDocument3 pagesDe La Salle University Medical Center Department of Obstetrics and GynecologyNehemiah FranciscoNo ratings yet
- B6 - Surgery GS II Case 1Document9 pagesB6 - Surgery GS II Case 1GregNo ratings yet
- Case Report: Division ADocument19 pagesCase Report: Division AAyuub AbdirizakNo ratings yet
- Team C Final Written OutputDocument22 pagesTeam C Final Written OutputCarina SuarezNo ratings yet
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocument15 pagesCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNo ratings yet
- Acute GlomerulonephritisDocument85 pagesAcute GlomerulonephritisPunsalan ChecaNo ratings yet
- Case Report II Internal MedicineDocument11 pagesCase Report II Internal MedicineGidu SaidNo ratings yet
- Case Presentation SleDocument33 pagesCase Presentation SleJxyp MundoNo ratings yet
- HIVCase Report II Internal MedicineDocument12 pagesHIVCase Report II Internal Medicineaxmedfare138No ratings yet
- APPENDICITISDocument69 pagesAPPENDICITISKim Alvarez100% (1)
- LinksDocument24 pagesLinksTrisNo ratings yet
- Admission Conference: Ernesto V. Ignacio JRDocument17 pagesAdmission Conference: Ernesto V. Ignacio JRernignacioNo ratings yet
- Chronic Obstructive PulmonaryDocument28 pagesChronic Obstructive PulmonaryAyu Sulung NariratriNo ratings yet
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDocument10 pagesConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoNo ratings yet
- Clinical Case PresentationDocument44 pagesClinical Case PresentationRUSSELL CILOTNo ratings yet
- History 1Document11 pagesHistory 1KaleabNo ratings yet
- Clinicopathologic Case Conference: Department of Family MedicineDocument39 pagesClinicopathologic Case Conference: Department of Family MedicineRaq KhoNo ratings yet
- Sample POMRDocument4 pagesSample POMRJeffrey RamosNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Skizofrenia (Pak Cecep)Document30 pagesSkizofrenia (Pak Cecep)Nurul SafitriNo ratings yet
- 409-Article Text-1439-1-10-20211018Document12 pages409-Article Text-1439-1-10-20211018Anonymous a2nxIq5No ratings yet
- Chemotherapy Administration in Pediatric: An OverviewDocument76 pagesChemotherapy Administration in Pediatric: An OverviewMiftaa HurrahmiNo ratings yet
- Indwelling CatheterDocument6 pagesIndwelling Cathetereloiza custodioNo ratings yet
- Prospectus New India Asha Kiran PolicyDocument17 pagesProspectus New India Asha Kiran PolicySHYLAJA DNo ratings yet
- Atlas of Retinal OCT 2nd EditionDocument480 pagesAtlas of Retinal OCT 2nd EditionSisoesNo ratings yet
- Osteoarthritis and Joint Diseases 2023Document29 pagesOsteoarthritis and Joint Diseases 2023Abdullah MelhimNo ratings yet
- I. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationDocument3 pagesI. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationCherubim Lei DC FloresNo ratings yet
- Preeclampsia Case StudyDocument13 pagesPreeclampsia Case StudyBiway RegalaNo ratings yet
- Louis Kuhne Facial Diagnosis 1897 02 PDFDocument105 pagesLouis Kuhne Facial Diagnosis 1897 02 PDFJosé BitarNo ratings yet
- Stem Cells and Their ApplicationDocument16 pagesStem Cells and Their ApplicationRam Kewal TripathiNo ratings yet
- 22.52 Social Determinants of HealthUK and The Local Government - 05 - 0Document26 pages22.52 Social Determinants of HealthUK and The Local Government - 05 - 0lesleyNo ratings yet
- NCP Outpatient Diagnosis Made EasierDocument19 pagesNCP Outpatient Diagnosis Made EasiertapallajanicaNo ratings yet
- Study PlanDocument4 pagesStudy PlanKeshab RijalNo ratings yet
- The Effect of Music On Auditory Hallucination and Quality of Life in Schizophrenic Patients: A Randomised Controlled TrialDocument9 pagesThe Effect of Music On Auditory Hallucination and Quality of Life in Schizophrenic Patients: A Randomised Controlled Trialyulia22No ratings yet
- Lect # 2 Care of Patients With Gout and Paget's DiseaseDocument21 pagesLect # 2 Care of Patients With Gout and Paget's DiseaseShayan ShayanNo ratings yet
- Managing Ammonia in Poultry Farms: Effects of Ammonia On BirdsDocument8 pagesManaging Ammonia in Poultry Farms: Effects of Ammonia On Birdsamamùra maamarNo ratings yet
- Emergency Psychiatry Primer On Series 1St Edition Tony Thrasher Editor Full ChapterDocument67 pagesEmergency Psychiatry Primer On Series 1St Edition Tony Thrasher Editor Full Chaptergina.larson159100% (12)
- Homeosiniatry - Combination of Acupuncture and HomeopathyDocument4 pagesHomeosiniatry - Combination of Acupuncture and HomeopathyGold SunriseNo ratings yet
- PNB Claim FormsDocument2 pagesPNB Claim Formssaika tabbasumNo ratings yet
- G.R. No. 193500 Government Service Insurance System, Petitioners SIMEON TAÑEDO, JR., RespondentDocument4 pagesG.R. No. 193500 Government Service Insurance System, Petitioners SIMEON TAÑEDO, JR., RespondentLara DelleNo ratings yet
- Stool Specimen CollectionDocument8 pagesStool Specimen CollectionPraveen KumarNo ratings yet
- RAD RLE Guide - Written Requirements: Patients DataDocument16 pagesRAD RLE Guide - Written Requirements: Patients DataHanniel MontecalboNo ratings yet
- Drug Study (Haloperidol)Document3 pagesDrug Study (Haloperidol)Mae Ann Bueno CastillonNo ratings yet
- Orthopaedic Trauma Lecture Notes MBCHBDocument73 pagesOrthopaedic Trauma Lecture Notes MBCHBjhqmpzg7sjNo ratings yet
- Authorization Approved: Applicant InformationDocument1 pageAuthorization Approved: Applicant Informationnicolle hansenNo ratings yet
- 11-Paroxysmal Nocturnal HaemoglobinuriaDocument6 pages11-Paroxysmal Nocturnal HaemoglobinuriaHamid IqbalNo ratings yet
- Challenging Cases in Neonatology 2018Document388 pagesChallenging Cases in Neonatology 2018Sabera Kapasi100% (1)