Download as pdf or txt
You might also like
- Naplex ReviewDocument63 pagesNaplex Reviewdivinevalley100% (7)
- Antiarrhythmic Drugs 1Document32 pagesAntiarrhythmic Drugs 1AliImadAlKhasakiNo ratings yet
- Antiarrhythmic Drugs: AmiodaroneDocument32 pagesAntiarrhythmic Drugs: Amiodaroneabd hamzaNo ratings yet
- Antiarrhythmic Drugs: Dr. Sachana KC 1 Year Resident Department of AnesthesiaDocument67 pagesAntiarrhythmic Drugs: Dr. Sachana KC 1 Year Resident Department of AnesthesiaKshitizma GiriNo ratings yet
- AntiarrhythmicsDocument10 pagesAntiarrhythmicslandita683No ratings yet
- Diskusi Topik Anestesi GamaDocument65 pagesDiskusi Topik Anestesi Gamakusumagama28No ratings yet
- Antiarrhythmic DrugsDocument20 pagesAntiarrhythmic DrugsMd FcpsNo ratings yet
- Antiarrhythmic DrugsDocument21 pagesAntiarrhythmic DrugsShoeb Nawaz Khan100% (1)
- Lecture 5 AntiarrhythmicsDocument51 pagesLecture 5 AntiarrhythmicsjawadNo ratings yet
- 448 - 194246 - Drug For Arrythmia - HandoutDocument4 pages448 - 194246 - Drug For Arrythmia - HandoutAnaliza Kitongan LantayanNo ratings yet
- نسخة ANTI-ARRHYTHMICDocument49 pagesنسخة ANTI-ARRHYTHMICManWol JangNo ratings yet
- Anti Arrhythmic DrugsDocument91 pagesAnti Arrhythmic DrugsAlex beharuNo ratings yet
- Antiarrhythmic Drugs Classification (Vaughan Williams)Document8 pagesAntiarrhythmic Drugs Classification (Vaughan Williams)ana100% (1)
- Wesam R KadhumDocument31 pagesWesam R Kadhumwisam_1by1No ratings yet
- Drugs Acting On Potassium Channel: Submitted By: Md. Ashikur Rahman ID: 171-021-032Document12 pagesDrugs Acting On Potassium Channel: Submitted By: Md. Ashikur Rahman ID: 171-021-032broken reedNo ratings yet
- Cardiac ArrhythmiaDocument101 pagesCardiac ArrhythmiaYuvraj ChauhanNo ratings yet
- Drugs Used in The Treatment of ArrhythmiasDocument37 pagesDrugs Used in The Treatment of ArrhythmiasChipego ChiyaamaNo ratings yet
- 3rd Year PharmacologyDocument43 pages3rd Year PharmacologyShayeeshan SivapalarajahNo ratings yet
- Cardio AssignmentDocument5 pagesCardio Assignmentthemega1111No ratings yet
- Agents Used in Cardiac ArrhythmiasDocument4 pagesAgents Used in Cardiac ArrhythmiasKaye PatriaNo ratings yet
- AntiarrhythmicsDocument7 pagesAntiarrhythmicszanderNo ratings yet
- AntiarrythmiaDocument11 pagesAntiarrythmiafdamissieNo ratings yet
- CV DrugsDocument6 pagesCV DrugssaharamichaelNo ratings yet
- Anti - ArrhythmicsDocument5 pagesAnti - ArrhythmicsAnabeth F. PungtilanNo ratings yet
- Pharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Document23 pagesPharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Nandraj123100% (1)
- Obat AntiaritmiaDocument18 pagesObat AntiaritmiaWahyu JuliandaNo ratings yet
- Calcium Channel Blockers and Vasodilators DizayeDocument3 pagesCalcium Channel Blockers and Vasodilators DizayeLegendary 099No ratings yet
- Antihypertensives 2Document6 pagesAntihypertensives 2Manyal Kutin KoakNo ratings yet
- Anti AnginaDocument5 pagesAnti Anginalandita683No ratings yet
- AmiodaroneDocument9 pagesAmiodaroneJonathan Ian ArinsolNo ratings yet
- MC Ii Unit IiiDocument38 pagesMC Ii Unit IiinallamillipavithraNo ratings yet
- FI-Medicinal Chemistry 3Document40 pagesFI-Medicinal Chemistry 3Meri Apri YaniNo ratings yet
- Antiarrhythmic DrugsDocument17 pagesAntiarrhythmic DrugsTarek G MustafaNo ratings yet
- Pharmacology of The Cardiovascular SystemsDocument4 pagesPharmacology of The Cardiovascular SystemsMark Russel Sean LealNo ratings yet
- Anti Arrhythmics 2Document1 pageAnti Arrhythmics 2Babu RamakrishnanNo ratings yet
- Antianginal and Antiischemic DrugsDocument18 pagesAntianginal and Antiischemic DrugsNaveen KumarNo ratings yet
- Antiarrhythmic Drugs Part 2Document4 pagesAntiarrhythmic Drugs Part 2AVINASH PvkNo ratings yet
- Prehospital MedicationsDocument123 pagesPrehospital Medicationshilwaalfi100% (1)
- L6 ANTIARRYTHMIC DRUGS - DR - Yagub S SalehDocument5 pagesL6 ANTIARRYTHMIC DRUGS - DR - Yagub S Salehnusaiba.alobaidyNo ratings yet
- Heart Failure and Antidysrhythmic DrugsDocument38 pagesHeart Failure and Antidysrhythmic DrugsYza Belle RamoNo ratings yet
- Antidysrhythmics UpdDocument3 pagesAntidysrhythmics UpdRyanMatiraNo ratings yet
- Cardioactive DrugsDocument20 pagesCardioactive DrugsPamela MendozaNo ratings yet
- M. Gabriel Khan - Cardiac Drug Therapy, Calcium Channel BlockersDocument21 pagesM. Gabriel Khan - Cardiac Drug Therapy, Calcium Channel BlockersluongcongthucNo ratings yet
- Issued A Strong WarningDocument4 pagesIssued A Strong WarningRiss CalmaNo ratings yet
- Treatment and Prophylaxis of HypertensionDocument4 pagesTreatment and Prophylaxis of HypertensionNCPP 2K18No ratings yet
- Lectures Combined CardiologieDocument143 pagesLectures Combined CardiologiedocsNo ratings yet
- Antiarrhythmic Drugs FinalDocument31 pagesAntiarrhythmic Drugs FinalAmanuel Maru50% (2)
- Antiarrhythmic DrugsDocument46 pagesAntiarrhythmic DrugsHUZAIFA YAMAANNo ratings yet
- Anti AritmiaDocument27 pagesAnti AritmiadoraemonmayaNo ratings yet
- Pharmacological Therapy of Arrhythmias (09.11.16)Document46 pagesPharmacological Therapy of Arrhythmias (09.11.16)Mariana CabralNo ratings yet
- Cardiovascular PharmacologyDocument80 pagesCardiovascular PharmacologyThái Hoà PhạmNo ratings yet
- Anti Arrythmia: IGMG. Surya Chandra T, Pharmacology Dept., School of Medicine, Udayana UnivDocument36 pagesAnti Arrythmia: IGMG. Surya Chandra T, Pharmacology Dept., School of Medicine, Udayana UnivSheryl ElitaNo ratings yet
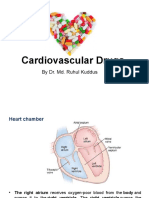
- Cardiovascular Drugs: by Dr. Md. Ruhul KuddusDocument56 pagesCardiovascular Drugs: by Dr. Md. Ruhul Kuddus53-Deepankar SutradharNo ratings yet
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 pagesAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdNo ratings yet
- Congestive Cardiac FailureDocument21 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Drugs For Systemic Hypertension and Angina: What's New?Document6 pagesDrugs For Systemic Hypertension and Angina: What's New?Diana GarcíaNo ratings yet
- 69.-AntiarrythmiticsDocument16 pages69.-AntiarrythmiticsireneNo ratings yet
- Treatment of TachyaarrhythmiaDocument1 pageTreatment of TachyaarrhythmiaFalaq2No ratings yet
- AntiarrhythmiaDocument29 pagesAntiarrhythmiaDRx Raju ChandranNo ratings yet
- Class III Drugs: Potassium Channel BlockadeDocument3 pagesClass III Drugs: Potassium Channel BlockadeMohammadDheniArdhiNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Antiarrhythmic PharmacologyDocument3 pagesAntiarrhythmic PharmacologyPatrick Tan100% (1)
- Cardiovascular Agents: Florianne E. Adlawan, R.NDocument31 pagesCardiovascular Agents: Florianne E. Adlawan, R.NadlawanflorianneNo ratings yet
- Antiarrhythmic AgentsDocument45 pagesAntiarrhythmic AgentsSoh Kae SiangNo ratings yet
- Antiarrhythmic Drugs-Test-2-QuestionsDocument7 pagesAntiarrhythmic Drugs-Test-2-QuestionsDrishya BioplannetNo ratings yet
- Antiarrhythmic Drugs FinalDocument31 pagesAntiarrhythmic Drugs FinalAmanuel Maru50% (2)
- A. Anti-Arrhythmic B.tech 5th SemDocument49 pagesA. Anti-Arrhythmic B.tech 5th SemNitesh SinghNo ratings yet
- Cardiovascular Drugs: Dare OgunladeDocument18 pagesCardiovascular Drugs: Dare OgunladeNatik Bi IllahNo ratings yet
- Cardiac Arrhythmias Cardiac ArrhythmiasDocument29 pagesCardiac Arrhythmias Cardiac ArrhythmiasgowthamNo ratings yet
- Case StudyDocument34 pagesCase StudyBSNNursing101No ratings yet
- Cardiovascular Pharmacology PDFDocument20 pagesCardiovascular Pharmacology PDFMelanie PrinceNo ratings yet
- ACLS ModuleDocument68 pagesACLS ModuleSalah ElbadawyNo ratings yet
- ATI Flash Cards 06, Medications Affecting The Cardiovascular SystemDocument48 pagesATI Flash Cards 06, Medications Affecting The Cardiovascular SystemWiilka QarnigaNo ratings yet
- Antiarrhythmic Drugs-Test-1-QuestionsDocument7 pagesAntiarrhythmic Drugs-Test-1-QuestionsDrishya Bioplannet100% (2)
- Pages From First Aid For The USMLE Step 1 2015, 25 Edition-2Document7 pagesPages From First Aid For The USMLE Step 1 2015, 25 Edition-2Mahmoud MohsenNo ratings yet
- Cardiovascular System Acronyms and MnemonicsDocument18 pagesCardiovascular System Acronyms and Mnemonicsdecsag06No ratings yet
- NCM 106 Cardiac DrugsDocument111 pagesNCM 106 Cardiac DrugsKatie HolmesNo ratings yet
- Cardiovascular Nursing Bullet Points I PDFDocument4 pagesCardiovascular Nursing Bullet Points I PDFKhalid Epping100% (3)
- Atrial Fibrillation and Flutter After Cardiac Surgery - UpToDateDocument22 pagesAtrial Fibrillation and Flutter After Cardiac Surgery - UpToDateFlavia SaccomaniNo ratings yet
- Anesthesiology and Intensive Care Medicine Answers For ExamDocument94 pagesAnesthesiology and Intensive Care Medicine Answers For Exammichal ben meronNo ratings yet
- Pharmacology of Antiarrhythmic Drugs - RecordedDocument33 pagesPharmacology of Antiarrhythmic Drugs - RecordedSarah SabtiNo ratings yet
- PHARMACOLOGY (Autocoid-Renal-GI-CV-CNS)Document33 pagesPHARMACOLOGY (Autocoid-Renal-GI-CV-CNS)Famela Anne GOmez MadambaNo ratings yet
- Mechanism of Action For Each Class of AntiDocument146 pagesMechanism of Action For Each Class of AntiReynaldo RiveraNo ratings yet
- Medsolutions PharmacologyDocument123 pagesMedsolutions Pharmacologykamran_zarrarNo ratings yet
- C G, A, A: Ardiac Lycosides Ntianginals AND NtidysrhythmicsDocument21 pagesC G, A, A: Ardiac Lycosides Ntianginals AND NtidysrhythmicsPam LalaNo ratings yet
- Classifications of Pharmaceutical Drugs1Document24 pagesClassifications of Pharmaceutical Drugs1RPh Krishna Chandra JagritNo ratings yet
- Pharmacology IIDocument178 pagesPharmacology IIMelanieNo ratings yet
- Tutorial On Electrophysiology of The Heart) Sam Dudley, Brown UniversityDocument50 pagesTutorial On Electrophysiology of The Heart) Sam Dudley, Brown UniversityNavojit Chowdhury100% (1)
- CPTP - Af & Anti CoagulationDocument4 pagesCPTP - Af & Anti CoagulationAinahMahaniNo ratings yet