
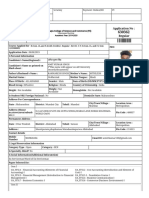
IPA Student Membership Form
IPA Student Membership Form
You might also like
- Api Membership FormDocument2 pagesApi Membership FormBiradar VijayNo ratings yet
- Application Form For Life Membership Andhra Pradesh Chapter of Association of Physicians of IndiaDocument1 pageApplication Form For Life Membership Andhra Pradesh Chapter of Association of Physicians of IndiakrishnaNo ratings yet
- IPC Registration FormDocument1 pageIPC Registration FormprashgiriNo ratings yet
- Indian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Document2 pagesIndian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22AmitNo ratings yet
- BMESI - Individual Membership Form - 2020Document1 pageBMESI - Individual Membership Form - 2020Manikandan NNo ratings yet
- Dhfws-Application Dh177r7p52a3540Document1 pageDhfws-Application Dh177r7p52a3540Avijit BasakNo ratings yet
- MembershipDocument1 pageMembershipAkhilesh Kumar SinghNo ratings yet
- Application No: Regular: Plot A-7/1, N.S. Road No. 10, J.V.P.D. Scheme - AndheriDocument2 pagesApplication No: Regular: Plot A-7/1, N.S. Road No. 10, J.V.P.D. Scheme - Andheriajay gupteNo ratings yet
- 6446 - IMA Membership Application Form 2022Document1 page6446 - IMA Membership Application Form 2022themuthekaNo ratings yet
- TKN 33081Document3 pagesTKN 33081Suku KoshyNo ratings yet
- MEAI Life Membership Application FormDocument3 pagesMEAI Life Membership Application Formmech.gdmnNo ratings yet
- Proforma For College - Information Regarding Fee, Bond - Conditions EtcDocument2 pagesProforma For College - Information Regarding Fee, Bond - Conditions EtcThe Indian DentistNo ratings yet
- FORM G - Renewal of RegistrationDocument2 pagesFORM G - Renewal of RegistrationShowry Reddy BandlaNo ratings yet
- Membership Form / Application For MembershipDocument2 pagesMembership Form / Application For MembershipIron XculptNo ratings yet
- Indian Institute of Banking & Finance "The Arcade", World Trade Centre, Cuffe Parade, Mumbai 400 005Document3 pagesIndian Institute of Banking & Finance "The Arcade", World Trade Centre, Cuffe Parade, Mumbai 400 005mpalanikumarNo ratings yet
- Application For Scholarship: OfficeDocument3 pagesApplication For Scholarship: OfficeJagannath MohapatraNo ratings yet
- Registration Form For Presenting Authors: PhotoDocument1 pageRegistration Form For Presenting Authors: PhotonaturalshadmaNo ratings yet
- Fresh: Backward Classes Development Department 2019-20Document3 pagesFresh: Backward Classes Development Department 2019-20abhilashNo ratings yet
- Membershipv 2Document2 pagesMembershipv 2Shailendra PatelNo ratings yet
- Medical/Nursing No Registrar: Academic Degree (S) (With Dates of Completion /universityDocument4 pagesMedical/Nursing No Registrar: Academic Degree (S) (With Dates of Completion /universityFazil MohammedNo ratings yet
- 8WCC Registration Form 2024Document1 page8WCC Registration Form 2024caaaNo ratings yet
- GAIL (India) Limited: (A Government of India Undertaking) (A Maharatna Company)Document4 pagesGAIL (India) Limited: (A Government of India Undertaking) (A Maharatna Company)KingNo ratings yet
- Iap Application FormDocument2 pagesIap Application FormSuresh100% (1)
- MEAI - Life Membership Application FormDocument3 pagesMEAI - Life Membership Application FormVedansh Thakur VedanshNo ratings yet
- AIOS Membership FormDocument2 pagesAIOS Membership FormiAdrivNo ratings yet
- Status of Bpharmacy Registration: Academic Information.Document4 pagesStatus of Bpharmacy Registration: Academic Information.AnjithNo ratings yet
- Declaration - 22207875 - 3 - 22 - 2022 12 - 53 - 39 AMDocument1 pageDeclaration - 22207875 - 3 - 22 - 2022 12 - 53 - 39 AMDuchess AnsariNo ratings yet
- MADURAI KAMARAJ UNIVERSITY PH - D ApplicationDocument8 pagesMADURAI KAMARAJ UNIVERSITY PH - D ApplicationvikisgNo ratings yet
- Application For Student MembershipDocument2 pagesApplication For Student Membershipapi-26153714No ratings yet
- API Membership FormDocument2 pagesAPI Membership FormMukesh Kumar100% (1)
- 21001434application 08 04 2024Document2 pages21001434application 08 04 2024atulraj2316No ratings yet
- Indian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Document2 pagesIndian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Amit Kr GodaraNo ratings yet
- DentalDocument4 pagesDentalKingshukNo ratings yet
- Fogsi Criteria and Application Form Social Security SchemeDocument3 pagesFogsi Criteria and Application Form Social Security SchemeAnanda MauryaNo ratings yet
- Annexure - For - PGDIE NITIEDocument5 pagesAnnexure - For - PGDIE NITIEIshika PadhyNo ratings yet
- Individual Membership: The Indian Institute of MetalsDocument3 pagesIndividual Membership: The Indian Institute of MetalsddgdmrlNo ratings yet
- ASI Membership Form PDF1Document2 pagesASI Membership Form PDF1Aishwarya NaikNo ratings yet
- IDA Membership FormDocument3 pagesIDA Membership FormAbhijit LeleNo ratings yet
- Undertaking:-: Prime Membership Application Form (Fill With All Capital Letters)Document3 pagesUndertaking:-: Prime Membership Application Form (Fill With All Capital Letters)Anuj ManglaNo ratings yet
- PMA Member Registration FormDocument1 pagePMA Member Registration FormMary patrize GonzalesNo ratings yet
- Membesrhip Form, AnatomyDocument1 pageMembesrhip Form, AnatomyVivek KumarNo ratings yet
- GAIL Website Advertisement - EnglishDocument3 pagesGAIL Website Advertisement - EnglishKingNo ratings yet
- SMS Info (MCC)Document2 pagesSMS Info (MCC)siddhantaNo ratings yet
- Curriculum Vitae: Dr. Ayeshik ChakrabortyDocument3 pagesCurriculum Vitae: Dr. Ayeshik ChakrabortyAyeshik ChakrabortyNo ratings yet
- Iaacd Registration FormDocument1 pageIaacd Registration FormkaderNo ratings yet
- Annual Subscription Reminder NoticeDocument1 pageAnnual Subscription Reminder NoticeBalaji KannanNo ratings yet
- Page No.1/2Document2 pagesPage No.1/2Shiva KumarNo ratings yet
- Medical Reimbursement Dipika Vasava 2019-20Document2 pagesMedical Reimbursement Dipika Vasava 2019-20praful2604No ratings yet
- Membership/ Renewal Form: Indian Association of Permanent MakeupDocument2 pagesMembership/ Renewal Form: Indian Association of Permanent MakeupAmit SharmaNo ratings yet
- MembershipApplicationForm Feb2010Document3 pagesMembershipApplicationForm Feb2010Prithvraj GopinathanNo ratings yet
- Application No: Regular: Vidyanagar - Mumbai Academic Year: 2019-2020Document2 pagesApplication No: Regular: Vidyanagar - Mumbai Academic Year: 2019-2020Kx Åmït SïñghNo ratings yet
- Member Application - The Association of SurgeonsDocument1 pageMember Application - The Association of SurgeonsCraj RajNo ratings yet
- Bar Council of Kerala Application For Admission As An Advocate On The Roll of The Bar Council of KeralaDocument3 pagesBar Council of Kerala Application For Admission As An Advocate On The Roll of The Bar Council of KeralaAjinRajNo ratings yet
- DR - Gopinath Saravanan - MIAP - ApplicationDocument2 pagesDR - Gopinath Saravanan - MIAP - ApplicationDr.Gopinath Saravanan67% (3)
- Application Form No. 16Document3 pagesApplication Form No. 16Iskolar TimeNo ratings yet
- Pravara Institute of Medical Sciences: Application Form For PIMS - AICET - 2008 PGDocument3 pagesPravara Institute of Medical Sciences: Application Form For PIMS - AICET - 2008 PGanon-998406No ratings yet
- I S O O I: Ndian Ociety F RAL MplantologistsDocument3 pagesI S O O I: Ndian Ociety F RAL MplantologistsBalwantNo ratings yet
- ASPICON 2019 BrochureDocument3 pagesASPICON 2019 BrochureAjay BansalNo ratings yet
- Drug StudyDocument3 pagesDrug StudyKristine Faith AzcuetaNo ratings yet
- Pharmaceutical Sales & Marketing Legal and Ethical ConsiderationsDocument41 pagesPharmaceutical Sales & Marketing Legal and Ethical ConsiderationsqmnwebNo ratings yet
- Timolol 2Document19 pagesTimolol 2Atthapu ThirupathaiahNo ratings yet
- Cephalosporins in Veterinary MedicineDocument23 pagesCephalosporins in Veterinary MedicineSunil100% (3)
- Occupations Vocabulary Esl Multiple Choice Tests For KidsDocument6 pagesOccupations Vocabulary Esl Multiple Choice Tests For KidsJanna RickNo ratings yet
- Folium Menthae PiperitaeDocument8 pagesFolium Menthae PiperitaeDestiny Vian DianNo ratings yet
- Alpha Spending FunctionDocument10 pagesAlpha Spending FunctionEcaterina AdascaliteiNo ratings yet
- BFMDocument18 pagesBFMGis GeorgeNo ratings yet
- Amines: Group 8Document14 pagesAmines: Group 8Aeriel Mcfernz AbercaNo ratings yet
- FavotriptanDocument12 pagesFavotriptansandyriaaaNo ratings yet
- Daftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDocument17 pagesDaftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiFirda LestariNo ratings yet
- Fentanyl Analouge SynthDocument11 pagesFentanyl Analouge SynthamesffNo ratings yet
- Determination of Isoniazid and Pyridoxine Hydrochloride Levels in Tablets With Ultraviolet Spectrophotometry by Successive Ratio DerivativeDocument7 pagesDetermination of Isoniazid and Pyridoxine Hydrochloride Levels in Tablets With Ultraviolet Spectrophotometry by Successive Ratio Derivativelemustarbatch60No ratings yet
- Principle, Advantages, Disadvantages, Applications of Different Sterilisation Methods and in Process ControlDocument40 pagesPrinciple, Advantages, Disadvantages, Applications of Different Sterilisation Methods and in Process ControlAnonymous GcUIZCKNo ratings yet
- English Task Give DirectionDocument4 pagesEnglish Task Give DirectionSindi LestariNo ratings yet
- BHP CraniotomyDocument8 pagesBHP Craniotomyintan purnama sariNo ratings yet
- Lecture 2 - Pharma HOTC Drug LawsDocument20 pagesLecture 2 - Pharma HOTC Drug LawsyahyaNo ratings yet
- Process Validation Guidelines PDFDocument13 pagesProcess Validation Guidelines PDFran_ooNo ratings yet
- Dyrenium Triamterene Drug CardDocument1 pageDyrenium Triamterene Drug CardSheri490No ratings yet
- Pain ManagementDocument162 pagesPain ManagementFASIKAW GIZAWNo ratings yet
- AESGP Conference - October 2019 - ProgrammeDocument3 pagesAESGP Conference - October 2019 - ProgrammeaesgpNo ratings yet
- The Science Issue - Edibles Magazine Edition 45Document33 pagesThe Science Issue - Edibles Magazine Edition 45Edibles MagazineNo ratings yet
- Dendrite International: Submitted by Group 8 Kavita Patil Kavya Gupta Narender Tanya Jain Tasya KatiyarDocument6 pagesDendrite International: Submitted by Group 8 Kavita Patil Kavya Gupta Narender Tanya Jain Tasya KatiyarTanya JainNo ratings yet
- Clinical Safety Data Management Periodic Safety UpdateDocument19 pagesClinical Safety Data Management Periodic Safety UpdatedopamNo ratings yet
- Nishtha (FMCG Industry)Document17 pagesNishtha (FMCG Industry)Nishtha BansalNo ratings yet
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- P List Sampharindo 2019Document10 pagesP List Sampharindo 2019pierosca tsaNo ratings yet
- Chapter 13. Heartburn and DyspepsiaDocument22 pagesChapter 13. Heartburn and DyspepsiaMonica CiorneiNo ratings yet
- Cryo Derm ENG 1Document15 pagesCryo Derm ENG 1beaumedicNo ratings yet
























































































Download as pdf or txt
You might also like
- Api Membership FormDocument2 pagesApi Membership FormBiradar VijayNo ratings yet
- Application Form For Life Membership Andhra Pradesh Chapter of Association of Physicians of IndiaDocument1 pageApplication Form For Life Membership Andhra Pradesh Chapter of Association of Physicians of IndiakrishnaNo ratings yet
- IPC Registration FormDocument1 pageIPC Registration FormprashgiriNo ratings yet
- Indian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Document2 pagesIndian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22AmitNo ratings yet
- BMESI - Individual Membership Form - 2020Document1 pageBMESI - Individual Membership Form - 2020Manikandan NNo ratings yet
- Dhfws-Application Dh177r7p52a3540Document1 pageDhfws-Application Dh177r7p52a3540Avijit BasakNo ratings yet
- MembershipDocument1 pageMembershipAkhilesh Kumar SinghNo ratings yet
- Application No: Regular: Plot A-7/1, N.S. Road No. 10, J.V.P.D. Scheme - AndheriDocument2 pagesApplication No: Regular: Plot A-7/1, N.S. Road No. 10, J.V.P.D. Scheme - Andheriajay gupteNo ratings yet
- 6446 - IMA Membership Application Form 2022Document1 page6446 - IMA Membership Application Form 2022themuthekaNo ratings yet
- TKN 33081Document3 pagesTKN 33081Suku KoshyNo ratings yet
- MEAI Life Membership Application FormDocument3 pagesMEAI Life Membership Application Formmech.gdmnNo ratings yet
- Proforma For College - Information Regarding Fee, Bond - Conditions EtcDocument2 pagesProforma For College - Information Regarding Fee, Bond - Conditions EtcThe Indian DentistNo ratings yet
- FORM G - Renewal of RegistrationDocument2 pagesFORM G - Renewal of RegistrationShowry Reddy BandlaNo ratings yet
- Membership Form / Application For MembershipDocument2 pagesMembership Form / Application For MembershipIron XculptNo ratings yet
- Indian Institute of Banking & Finance "The Arcade", World Trade Centre, Cuffe Parade, Mumbai 400 005Document3 pagesIndian Institute of Banking & Finance "The Arcade", World Trade Centre, Cuffe Parade, Mumbai 400 005mpalanikumarNo ratings yet
- Application For Scholarship: OfficeDocument3 pagesApplication For Scholarship: OfficeJagannath MohapatraNo ratings yet
- Registration Form For Presenting Authors: PhotoDocument1 pageRegistration Form For Presenting Authors: PhotonaturalshadmaNo ratings yet
- Fresh: Backward Classes Development Department 2019-20Document3 pagesFresh: Backward Classes Development Department 2019-20abhilashNo ratings yet
- Membershipv 2Document2 pagesMembershipv 2Shailendra PatelNo ratings yet
- Medical/Nursing No Registrar: Academic Degree (S) (With Dates of Completion /universityDocument4 pagesMedical/Nursing No Registrar: Academic Degree (S) (With Dates of Completion /universityFazil MohammedNo ratings yet
- 8WCC Registration Form 2024Document1 page8WCC Registration Form 2024caaaNo ratings yet
- GAIL (India) Limited: (A Government of India Undertaking) (A Maharatna Company)Document4 pagesGAIL (India) Limited: (A Government of India Undertaking) (A Maharatna Company)KingNo ratings yet
- Iap Application FormDocument2 pagesIap Application FormSuresh100% (1)
- MEAI - Life Membership Application FormDocument3 pagesMEAI - Life Membership Application FormVedansh Thakur VedanshNo ratings yet
- AIOS Membership FormDocument2 pagesAIOS Membership FormiAdrivNo ratings yet
- Status of Bpharmacy Registration: Academic Information.Document4 pagesStatus of Bpharmacy Registration: Academic Information.AnjithNo ratings yet
- Declaration - 22207875 - 3 - 22 - 2022 12 - 53 - 39 AMDocument1 pageDeclaration - 22207875 - 3 - 22 - 2022 12 - 53 - 39 AMDuchess AnsariNo ratings yet
- MADURAI KAMARAJ UNIVERSITY PH - D ApplicationDocument8 pagesMADURAI KAMARAJ UNIVERSITY PH - D ApplicationvikisgNo ratings yet
- Application For Student MembershipDocument2 pagesApplication For Student Membershipapi-26153714No ratings yet
- API Membership FormDocument2 pagesAPI Membership FormMukesh Kumar100% (1)
- 21001434application 08 04 2024Document2 pages21001434application 08 04 2024atulraj2316No ratings yet
- Indian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Document2 pagesIndian Dairy Association: IDA House, Sector IV, R.K. Puram, N. Delhi-22Amit Kr GodaraNo ratings yet
- DentalDocument4 pagesDentalKingshukNo ratings yet
- Fogsi Criteria and Application Form Social Security SchemeDocument3 pagesFogsi Criteria and Application Form Social Security SchemeAnanda MauryaNo ratings yet
- Annexure - For - PGDIE NITIEDocument5 pagesAnnexure - For - PGDIE NITIEIshika PadhyNo ratings yet
- Individual Membership: The Indian Institute of MetalsDocument3 pagesIndividual Membership: The Indian Institute of MetalsddgdmrlNo ratings yet
- ASI Membership Form PDF1Document2 pagesASI Membership Form PDF1Aishwarya NaikNo ratings yet
- IDA Membership FormDocument3 pagesIDA Membership FormAbhijit LeleNo ratings yet
- Undertaking:-: Prime Membership Application Form (Fill With All Capital Letters)Document3 pagesUndertaking:-: Prime Membership Application Form (Fill With All Capital Letters)Anuj ManglaNo ratings yet
- PMA Member Registration FormDocument1 pagePMA Member Registration FormMary patrize GonzalesNo ratings yet
- Membesrhip Form, AnatomyDocument1 pageMembesrhip Form, AnatomyVivek KumarNo ratings yet
- GAIL Website Advertisement - EnglishDocument3 pagesGAIL Website Advertisement - EnglishKingNo ratings yet
- SMS Info (MCC)Document2 pagesSMS Info (MCC)siddhantaNo ratings yet
- Curriculum Vitae: Dr. Ayeshik ChakrabortyDocument3 pagesCurriculum Vitae: Dr. Ayeshik ChakrabortyAyeshik ChakrabortyNo ratings yet
- Iaacd Registration FormDocument1 pageIaacd Registration FormkaderNo ratings yet
- Annual Subscription Reminder NoticeDocument1 pageAnnual Subscription Reminder NoticeBalaji KannanNo ratings yet
- Page No.1/2Document2 pagesPage No.1/2Shiva KumarNo ratings yet
- Medical Reimbursement Dipika Vasava 2019-20Document2 pagesMedical Reimbursement Dipika Vasava 2019-20praful2604No ratings yet
- Membership/ Renewal Form: Indian Association of Permanent MakeupDocument2 pagesMembership/ Renewal Form: Indian Association of Permanent MakeupAmit SharmaNo ratings yet
- MembershipApplicationForm Feb2010Document3 pagesMembershipApplicationForm Feb2010Prithvraj GopinathanNo ratings yet
- Application No: Regular: Vidyanagar - Mumbai Academic Year: 2019-2020Document2 pagesApplication No: Regular: Vidyanagar - Mumbai Academic Year: 2019-2020Kx Åmït SïñghNo ratings yet
- Member Application - The Association of SurgeonsDocument1 pageMember Application - The Association of SurgeonsCraj RajNo ratings yet
- Bar Council of Kerala Application For Admission As An Advocate On The Roll of The Bar Council of KeralaDocument3 pagesBar Council of Kerala Application For Admission As An Advocate On The Roll of The Bar Council of KeralaAjinRajNo ratings yet
- DR - Gopinath Saravanan - MIAP - ApplicationDocument2 pagesDR - Gopinath Saravanan - MIAP - ApplicationDr.Gopinath Saravanan67% (3)
- Application Form No. 16Document3 pagesApplication Form No. 16Iskolar TimeNo ratings yet
- Pravara Institute of Medical Sciences: Application Form For PIMS - AICET - 2008 PGDocument3 pagesPravara Institute of Medical Sciences: Application Form For PIMS - AICET - 2008 PGanon-998406No ratings yet
- I S O O I: Ndian Ociety F RAL MplantologistsDocument3 pagesI S O O I: Ndian Ociety F RAL MplantologistsBalwantNo ratings yet
- ASPICON 2019 BrochureDocument3 pagesASPICON 2019 BrochureAjay BansalNo ratings yet
- Drug StudyDocument3 pagesDrug StudyKristine Faith AzcuetaNo ratings yet
- Pharmaceutical Sales & Marketing Legal and Ethical ConsiderationsDocument41 pagesPharmaceutical Sales & Marketing Legal and Ethical ConsiderationsqmnwebNo ratings yet
- Timolol 2Document19 pagesTimolol 2Atthapu ThirupathaiahNo ratings yet
- Cephalosporins in Veterinary MedicineDocument23 pagesCephalosporins in Veterinary MedicineSunil100% (3)
- Occupations Vocabulary Esl Multiple Choice Tests For KidsDocument6 pagesOccupations Vocabulary Esl Multiple Choice Tests For KidsJanna RickNo ratings yet
- Folium Menthae PiperitaeDocument8 pagesFolium Menthae PiperitaeDestiny Vian DianNo ratings yet
- Alpha Spending FunctionDocument10 pagesAlpha Spending FunctionEcaterina AdascaliteiNo ratings yet
- BFMDocument18 pagesBFMGis GeorgeNo ratings yet
- Amines: Group 8Document14 pagesAmines: Group 8Aeriel Mcfernz AbercaNo ratings yet
- FavotriptanDocument12 pagesFavotriptansandyriaaaNo ratings yet
- Daftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDocument17 pagesDaftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiFirda LestariNo ratings yet
- Fentanyl Analouge SynthDocument11 pagesFentanyl Analouge SynthamesffNo ratings yet
- Determination of Isoniazid and Pyridoxine Hydrochloride Levels in Tablets With Ultraviolet Spectrophotometry by Successive Ratio DerivativeDocument7 pagesDetermination of Isoniazid and Pyridoxine Hydrochloride Levels in Tablets With Ultraviolet Spectrophotometry by Successive Ratio Derivativelemustarbatch60No ratings yet
- Principle, Advantages, Disadvantages, Applications of Different Sterilisation Methods and in Process ControlDocument40 pagesPrinciple, Advantages, Disadvantages, Applications of Different Sterilisation Methods and in Process ControlAnonymous GcUIZCKNo ratings yet
- English Task Give DirectionDocument4 pagesEnglish Task Give DirectionSindi LestariNo ratings yet
- BHP CraniotomyDocument8 pagesBHP Craniotomyintan purnama sariNo ratings yet
- Lecture 2 - Pharma HOTC Drug LawsDocument20 pagesLecture 2 - Pharma HOTC Drug LawsyahyaNo ratings yet
- Process Validation Guidelines PDFDocument13 pagesProcess Validation Guidelines PDFran_ooNo ratings yet
- Dyrenium Triamterene Drug CardDocument1 pageDyrenium Triamterene Drug CardSheri490No ratings yet
- Pain ManagementDocument162 pagesPain ManagementFASIKAW GIZAWNo ratings yet
- AESGP Conference - October 2019 - ProgrammeDocument3 pagesAESGP Conference - October 2019 - ProgrammeaesgpNo ratings yet
- The Science Issue - Edibles Magazine Edition 45Document33 pagesThe Science Issue - Edibles Magazine Edition 45Edibles MagazineNo ratings yet
- Dendrite International: Submitted by Group 8 Kavita Patil Kavya Gupta Narender Tanya Jain Tasya KatiyarDocument6 pagesDendrite International: Submitted by Group 8 Kavita Patil Kavya Gupta Narender Tanya Jain Tasya KatiyarTanya JainNo ratings yet
- Clinical Safety Data Management Periodic Safety UpdateDocument19 pagesClinical Safety Data Management Periodic Safety UpdatedopamNo ratings yet
- Nishtha (FMCG Industry)Document17 pagesNishtha (FMCG Industry)Nishtha BansalNo ratings yet
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- P List Sampharindo 2019Document10 pagesP List Sampharindo 2019pierosca tsaNo ratings yet
- Chapter 13. Heartburn and DyspepsiaDocument22 pagesChapter 13. Heartburn and DyspepsiaMonica CiorneiNo ratings yet
- Cryo Derm ENG 1Document15 pagesCryo Derm ENG 1beaumedicNo ratings yet