Download as docx, pdf, or txt
You might also like
- BLS Provider Manual 2020 PDFDocument121 pagesBLS Provider Manual 2020 PDFNur Yaya100% (2)
- Resuscitation Triangle Roles: Compressor Team LeaderDocument1 pageResuscitation Triangle Roles: Compressor Team Leaderhkjhks100% (1)
- African American Rescue PlanDocument54 pagesAfrican American Rescue PlanKaylyn ReneeNo ratings yet
- RFDDocument34 pagesRFDLEA CORPUZNo ratings yet
- Psychosocial Processing - : (Stress Debriefing)Document36 pagesPsychosocial Processing - : (Stress Debriefing)Vanessa Devota Veloso - Ramirez100% (1)
- System Analysis and Design: Pamantasan NG Lungsod NG MaynilaDocument32 pagesSystem Analysis and Design: Pamantasan NG Lungsod NG MaynilacorinaalonzoNo ratings yet
- Comparision of All FMCG CompaniesDocument2 pagesComparision of All FMCG CompaniesPuneeth KumarNo ratings yet
- Pricon - Product at Glance - General CatalogDocument19 pagesPricon - Product at Glance - General Catalogophtho india incNo ratings yet
- Municipal Ordinance No. 25-2021 DRRM-HDocument5 pagesMunicipal Ordinance No. 25-2021 DRRM-HJason Lape0% (1)
- Disaster ManagementDocument80 pagesDisaster ManagementAmzar SaniNo ratings yet
- Fe Del Mundo Global Health Institute: Philip P. Ines, RNDocument2 pagesFe Del Mundo Global Health Institute: Philip P. Ines, RNYosef OxinioNo ratings yet
- 7trinity 3governanceDocument28 pages7trinity 3governanceSurendra NandaNo ratings yet
- Chapter 3 A.3. Coordination Protection ClusterDocument5 pagesChapter 3 A.3. Coordination Protection ClusterMaria Rose AquinoNo ratings yet
- Hse-P-20. Medevac OficinaDocument7 pagesHse-P-20. Medevac Oficinalady varonNo ratings yet
- Program : Psupt Samuel A ErandioDocument2 pagesProgram : Psupt Samuel A ErandioEmmanuel BatinganNo ratings yet
- OPH Welcome Packet - Apr2021Document15 pagesOPH Welcome Packet - Apr2021Osmar PadillaNo ratings yet
- PRIMARY AND SECONDARY SURVEY ER TRIAGE BLS ACLS - PPTX 1Document20 pagesPRIMARY AND SECONDARY SURVEY ER TRIAGE BLS ACLS - PPTX 1Ansherina Murillo AguilarNo ratings yet
- User AnalysisDocument4 pagesUser AnalysisBharath SrinivasanNo ratings yet
- PGS Conferment ProgramDocument2 pagesPGS Conferment ProgramSohaira DimapintoNo ratings yet
- Cheng IPCRDocument2 pagesCheng IPCRAngelie Mae Ajoste-AbelonNo ratings yet
- Levels of Ecological OrganizationDocument1 pageLevels of Ecological OrganizationFrenzoe Nillas DemecilloNo ratings yet
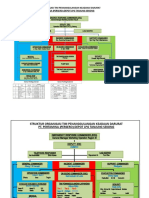
- Struktur Organisasi Tim Penanggulangan Keadaan Darurat Pt. Pertamina (Persero) Depot LPG Tanjung SekongDocument4 pagesStruktur Organisasi Tim Penanggulangan Keadaan Darurat Pt. Pertamina (Persero) Depot LPG Tanjung SekongArjuna RizqyNo ratings yet
- CAs Selection GradeDocument15 pagesCAs Selection GradekskchariNo ratings yet
- RifeMedic 8 Program List 2023Document84 pagesRifeMedic 8 Program List 2023pierre van wykNo ratings yet
- Rusvuz MedDocument12 pagesRusvuz MedhermeniodropshippingNo ratings yet
- Road Crash Information Sheet FinalDocument1 pageRoad Crash Information Sheet FinalARCHIE AJIASNo ratings yet
- Perio Samanvay Lect 1Document1 pagePerio Samanvay Lect 1harithrra vNo ratings yet
- Mdrrmo Capdev 2021Document1 pageMdrrmo Capdev 2021mdrrmclinamonNo ratings yet
- Abc-Hsse-Ofaa-31-Occupational First Aid Assessment FormDocument1 pageAbc-Hsse-Ofaa-31-Occupational First Aid Assessment FormFrancis Mier SereñoNo ratings yet
- 01 Jmri - 2017 PDFDocument313 pages01 Jmri - 2017 PDFVicente MartinezNo ratings yet
- QR-ADM-1015 - Training PlanDocument2 pagesQR-ADM-1015 - Training PlanHR SundiaNo ratings yet
- Assignment 3 Operational PlanningDocument6 pagesAssignment 3 Operational PlanningMingming MamingawNo ratings yet
- Personal Agenda Talents: Close CombatDocument1 pagePersonal Agenda Talents: Close CombatOwain RichardsNo ratings yet
- Notes On Cor Ad 2019 1Document48 pagesNotes On Cor Ad 2019 1Gierald TubilNo ratings yet
- School OF Planni NG & Archi Tecture: Lakshmi Das. PDocument19 pagesSchool OF Planni NG & Archi Tecture: Lakshmi Das. PLekshmi KrishnadasNo ratings yet
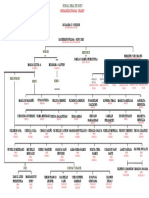
- Lobo Rural Health Unit Organizational ChartDocument2 pagesLobo Rural Health Unit Organizational Chartlobomho.infoNo ratings yet
- The Transactinides PDFDocument1 pageThe Transactinides PDFWade HarrisNo ratings yet
- 1.2 Problem Solving ApproachDocument8 pages1.2 Problem Solving ApproachAshwin JudalNo ratings yet
- Seven R'S of Logistics: Right ProductDocument1 pageSeven R'S of Logistics: Right ProductKatherine BernalNo ratings yet
- Adobe Scan Apr 08, 2021Document7 pagesAdobe Scan Apr 08, 2021Kuldeep YadavNo ratings yet
- ConsiDocument1 pageConsiDineshNo ratings yet
- RHU Organizational ChartDocument1 pageRHU Organizational ChartBryant AndunganNo ratings yet
- Jems201707 DL PDFDocument70 pagesJems201707 DL PDFPierre FlorentínNo ratings yet
- Guidelines To Fill in Health Examination: Borang RME / IPT Malaysia/HELPDocument5 pagesGuidelines To Fill in Health Examination: Borang RME / IPT Malaysia/HELPaizadashkaNo ratings yet
- Introduction To Human Resource Mnagement:: Meaning Objectives NeedDocument9 pagesIntroduction To Human Resource Mnagement:: Meaning Objectives NeedHasnain BaberNo ratings yet
- Translation of Nursing Practice Into The Electronic Healthcare Record Systems: Now & in Our FutureDocument17 pagesTranslation of Nursing Practice Into The Electronic Healthcare Record Systems: Now & in Our FutureChildren's National Medical CenterNo ratings yet
- VA Management and Care FMC FreeDocument180 pagesVA Management and Care FMC FreeRasangi Sumudu Clare SuraweeraNo ratings yet
- Dolor 2022Document34 pagesDolor 2022Jorge HdzNo ratings yet
- Compassionate Apothecary OpinionDocument8 pagesCompassionate Apothecary OpinionfalklawNo ratings yet
- 5.8 Incident Site Management CompressedDocument66 pages5.8 Incident Site Management CompressedMuhamad Izuan Abdul MananNo ratings yet
- Alien Character Sheet Printerfriendly (Fillable)Document1 pageAlien Character Sheet Printerfriendly (Fillable)Car LamNo ratings yet
- Sdo DRRM StructureDocument6 pagesSdo DRRM StructureJf JohnNo ratings yet
- HG3221DDocument2 pagesHG3221DVicky pawarNo ratings yet
- HRDD Duties and FunctionsDocument25 pagesHRDD Duties and FunctionsLDD Aklan PPONo ratings yet
- Elbow Tree Chart ContDocument1 pageElbow Tree Chart ContRehab AbidNo ratings yet
- Accreditation, Mobilization, and Protection of Disaster Volunteers and National Service Reserve Corps, Civil Society Organization and The Private Sector (Section 13, PDRRM Act)Document30 pagesAccreditation, Mobilization, and Protection of Disaster Volunteers and National Service Reserve Corps, Civil Society Organization and The Private Sector (Section 13, PDRRM Act)Jannico Elinon DanoNo ratings yet
- AAR-NSED-edited 2Document3 pagesAAR-NSED-edited 2enriquetamayocayagoNo ratings yet
- MSFT6008 Reading7Document2 pagesMSFT6008 Reading7api-3703139No ratings yet
- Functional Analytical PsychotherapyDocument72 pagesFunctional Analytical PsychotherapyScribdTranslationsNo ratings yet
- Trauma TeamDocument42 pagesTrauma TeamAda Luisa Maguiña GuadalupeNo ratings yet
- POLICY GUIDELINESDocument2 pagesPOLICY GUIDELINESlabiaernestoNo ratings yet
- 13CHODocument67 pages13CHOlabiaernestoNo ratings yet
- HEALTH ADMINISTRATION OVERVIEWDocument17 pagesHEALTH ADMINISTRATION OVERVIEWlabiaernestoNo ratings yet
- Information ManagementDocument32 pagesInformation ManagementlabiaernestoNo ratings yet
- Annex C.1 AOP Situational and Gap Analysis Summary 15oct2021Document1 pageAnnex C.1 AOP Situational and Gap Analysis Summary 15oct2021labiaernestoNo ratings yet
- handout-3-2.1Document18 pageshandout-3-2.1labiaernestoNo ratings yet
- Sample ReportDocument2 pagesSample ReportlabiaernestoNo ratings yet
- MS-15-99Document106 pagesMS-15-99labiaernestoNo ratings yet
- MANAGEMENT AND ORGANIZATIONDocument86 pagesMANAGEMENT AND ORGANIZATIONlabiaernestoNo ratings yet
- CPG For AdultsDocument21 pagesCPG For AdultslabiaernestoNo ratings yet
- Monitoring Status LevelDocument10 pagesMonitoring Status LevellabiaernestoNo ratings yet
- Breakout - 4 Ease of Doing BusinessDocument24 pagesBreakout - 4 Ease of Doing BusinesslabiaernestoNo ratings yet
- Template B - Major Event Monitoring SheetDocument1 pageTemplate B - Major Event Monitoring SheetlabiaernestoNo ratings yet
- Eoc Ambulance Transport Policy - SopDocument14 pagesEoc Ambulance Transport Policy - SoplabiaernestoNo ratings yet
- Improving Access To Medicines by Popularising GeneDocument18 pagesImproving Access To Medicines by Popularising GenelabiaernestoNo ratings yet
- 007 Policies Infection ControlDocument16 pages007 Policies Infection ControllabiaernestoNo ratings yet
- Demuth Perception Theories1.1Document49 pagesDemuth Perception Theories1.1labiaernestoNo ratings yet
- Consumer PerceptionDocument23 pagesConsumer PerceptionlabiaernestoNo ratings yet
- Five Levels of Apa HeadingsDocument1 pageFive Levels of Apa HeadingslabiaernestoNo ratings yet
- Ey Innovation Public Sector enDocument28 pagesEy Innovation Public Sector enlabiaernestoNo ratings yet
- Housing Design and Construction TechnologyDocument13 pagesHousing Design and Construction TechnologySamyNo ratings yet
- Fire HazardDocument16 pagesFire HazardHacienda Cien LouisitaNo ratings yet
- Your Text Here: Emergency Response PlanDocument95 pagesYour Text Here: Emergency Response PlanRimNo ratings yet
- Disaster Management PresentationDocument64 pagesDisaster Management Presentationsukhwinder singh100% (1)
- Report Zamboanga Peace CampDocument25 pagesReport Zamboanga Peace Campsheryl_morales100% (1)
- Guide On Reporting of COVID-19 Cases - Staff IntranetDocument1 pageGuide On Reporting of COVID-19 Cases - Staff Intranet湯皓升No ratings yet
- DRRR ReportDocument50 pagesDRRR ReportSTAR CHINEMA100% (1)
- Cluster State Focal Points - AugustDocument2 pagesCluster State Focal Points - AugustSteve NjengaNo ratings yet
- Barangay Peace Action TeamsDocument12 pagesBarangay Peace Action TeamsMarieta Alejo100% (2)
- History & Set Up: 1.1. Background InformationDocument32 pagesHistory & Set Up: 1.1. Background InformationNoopur Toshniwal KapoorNo ratings yet
- DM Plan Tahirpur Upazila Sunamgonj District - English Version-2014Document135 pagesDM Plan Tahirpur Upazila Sunamgonj District - English Version-2014CDMP BangladeshNo ratings yet
- TAE40116 WHS Policies and Procedures V4.0Document8 pagesTAE40116 WHS Policies and Procedures V4.0Monal PansalNo ratings yet
- Edukasi IPS: Peran Profesi Perawat Dalam Penanggulangan Bencana Di IndoneisiaDocument11 pagesEdukasi IPS: Peran Profesi Perawat Dalam Penanggulangan Bencana Di IndoneisiaFredy MarlisNo ratings yet
- Draft Guideline For First Responder Chemical and Technological HazardsDocument59 pagesDraft Guideline For First Responder Chemical and Technological HazardsToufik AhmedNo ratings yet
- Fire Fighting Sheet 1Document1 pageFire Fighting Sheet 1ayush dattaNo ratings yet
- Kair Fakir Toll Plaza - Rajesthan - November - 2023 - Monthly Call Summery Report - Zone 2Document6 pagesKair Fakir Toll Plaza - Rajesthan - November - 2023 - Monthly Call Summery Report - Zone 2kamina.yaar099No ratings yet
- High Power Committee Report On Revamping of Civil DefenceDocument115 pagesHigh Power Committee Report On Revamping of Civil DefencedgcivildefencebiharNo ratings yet
- Brgy. Bayabas BDRRMCDocument4 pagesBrgy. Bayabas BDRRMCantoniobose52No ratings yet
- PNP Transformation ProgramDocument43 pagesPNP Transformation ProgramPs Seven NeutronNo ratings yet
- Trainees Manual - RDANA - 2021-06-15-01-51-52-pmDocument65 pagesTrainees Manual - RDANA - 2021-06-15-01-51-52-pmCJ Acido100% (1)
- Sitxwhs003 Learner Guide v1.2 AcotDocument90 pagesSitxwhs003 Learner Guide v1.2 AcotKomal SharmaNo ratings yet
- Emergency Response Plan - Rev 0Document12 pagesEmergency Response Plan - Rev 0IslamAl-BazNo ratings yet
- Front PageDocument1 pageFront PagePan PanNo ratings yet
- S3b1 Malaysia PDFDocument68 pagesS3b1 Malaysia PDFlittle projectNo ratings yet
- Alnajim Alzahir Co. - Emergency Evacuation Drill On 10-May-2022Document12 pagesAlnajim Alzahir Co. - Emergency Evacuation Drill On 10-May-2022Abdullah TwfeeqNo ratings yet
- CSMR Reg 350-3 Mems BadgeDocument16 pagesCSMR Reg 350-3 Mems Badgemailbocks96No ratings yet
- Business Risk Profile vs. Defense-in-Depth Index Summary ReportDocument2 pagesBusiness Risk Profile vs. Defense-in-Depth Index Summary ReportLiliana CondreaNo ratings yet
- Vi - Facilities Physical Plant Evaluation FormDocument20 pagesVi - Facilities Physical Plant Evaluation FormAaron Paul CasabarNo ratings yet