Download as pdf or txt
You might also like
- AI Architectures A Culinary GuideDocument30 pagesAI Architectures A Culinary GuideskyonNo ratings yet
- Venture Bros: Innocence Cast AsideDocument73 pagesVenture Bros: Innocence Cast AsideZeb EcklesNo ratings yet
- Cerebellar Stroke in A COVID-19 Infected Patient. A Case ReportDocument6 pagesCerebellar Stroke in A COVID-19 Infected Patient. A Case ReportMuhammad Reza FirdausNo ratings yet
- How I Treat and Manage Strokes in Sickle Cell DiseaseDocument10 pagesHow I Treat and Manage Strokes in Sickle Cell DiseaseNinaNo ratings yet
- 2021-Acute Myocarditis After Administration of The BNT162b2 Vaccine Against COVID-19Document3 pages2021-Acute Myocarditis After Administration of The BNT162b2 Vaccine Against COVID-19seguridadyambiente641No ratings yet
- Seizure As The Presenting Symptom of COVID-19Document26 pagesSeizure As The Presenting Symptom of COVID-19Dota PlayerNo ratings yet
- Stroke 2Document30 pagesStroke 2somyahNo ratings yet
- Status of Sars-Cov-2 in Cerebrospinal Fluid of Patients With Covid-19 and StrokeDocument3 pagesStatus of Sars-Cov-2 in Cerebrospinal Fluid of Patients With Covid-19 and StrokeSanjay KumarNo ratings yet
- COVID 19 and Stroke Incidence and Etiological Description inDocument9 pagesCOVID 19 and Stroke Incidence and Etiological Description innascool2016No ratings yet
- Covid-Stroke 1 PDFDocument18 pagesCovid-Stroke 1 PDFMelya UmbulNo ratings yet
- To Study Hematological Profile in Covid-19 Patients in Relation With Prognosis and Outcome: - A Cross Sectional Observational StudyDocument7 pagesTo Study Hematological Profile in Covid-19 Patients in Relation With Prognosis and Outcome: - A Cross Sectional Observational StudyIJAR JOURNALNo ratings yet
- Computed Tomography Features of Cerebrovascular ComplicationsDocument6 pagesComputed Tomography Features of Cerebrovascular ComplicationsBiomédica Fabiane IngrideNo ratings yet
- Reversible Cerebral Vasoconstriction Syndrome Part 1 Epidemiology Pathogenesis and Clinical CourseAJNR2015Document8 pagesReversible Cerebral Vasoconstriction Syndrome Part 1 Epidemiology Pathogenesis and Clinical CourseAJNR2015Winston FontesNo ratings yet
- Mesa Et Al., ICN.Document9 pagesMesa Et Al., ICN.Maria Jose Zuluaga RobayoNo ratings yet
- The Female Predominant Persistent Inmune Dysregulation of The Post Covid Syndrome - Ganesh - 2021Document11 pagesThe Female Predominant Persistent Inmune Dysregulation of The Post Covid Syndrome - Ganesh - 2021Isis StoreNo ratings yet
- (RCT) Cardiovascular Injuries After Covid-19 InfectionDocument7 pages(RCT) Cardiovascular Injuries After Covid-19 InfectionPatrick NunsioNo ratings yet
- Renal Resistive Index As A Predictor of Acute Kidney Injury and Mortality in COVID-19 Critically Ill PatientsDocument8 pagesRenal Resistive Index As A Predictor of Acute Kidney Injury and Mortality in COVID-19 Critically Ill PatientsEko NoviantiNo ratings yet
- JCM 11 06258Document13 pagesJCM 11 06258deja234No ratings yet
- EM in Patients With Covid19Document39 pagesEM in Patients With Covid19kenmitaNo ratings yet
- Miller Fisher Syndrome and Polyneuritis CranialisDocument6 pagesMiller Fisher Syndrome and Polyneuritis CranialisDUVAN FELIPE ARIZA TENORIONo ratings yet
- Admission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailureDocument18 pagesAdmission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailurePuja Nastia LubisNo ratings yet
- 2.prevalence and Impact of - Myocardial InjuryDocument14 pages2.prevalence and Impact of - Myocardial Injuryrest_a2003No ratings yet
- Manuscrito Stroke and CovidDocument6 pagesManuscrito Stroke and CovidDeysi Daniela Ordinola CalleNo ratings yet
- 1 s2.0 S0002914916305574 MainDocument6 pages1 s2.0 S0002914916305574 MainDavid Jimmy Kurniawan RejosaputroNo ratings yet
- Creutzfeld JacobDocument8 pagesCreutzfeld JacobAllal SalimNo ratings yet
- Creutzfeld JacobDocument8 pagesCreutzfeld JacobAllal SalimNo ratings yet
- PIIS0022510X20304998Document7 pagesPIIS0022510X20304998dhea handyaraNo ratings yet
- Reversible Cerebral Vasoconstriction Syndrome, Part 1: Epidemiology, Pathogenesis, and Clinical CourseDocument8 pagesReversible Cerebral Vasoconstriction Syndrome, Part 1: Epidemiology, Pathogenesis, and Clinical CourseAlfath Zulfa FadhilahNo ratings yet
- 3 - Tuberculous Meningitis in Adults - Review of 48 Cases 1996 (Modelo para o Trabalho)Document7 pages3 - Tuberculous Meningitis in Adults - Review of 48 Cases 1996 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- Ischemic Stroke Associated With Novel Coronavirus 2019 A Report of Three CasesDocument6 pagesIschemic Stroke Associated With Novel Coronavirus 2019 A Report of Three CasesDewianggreini DandaNo ratings yet
- Simon 2016Document12 pagesSimon 2016yoNo ratings yet
- 12 11 PBDocument168 pages12 11 PBYS NateNo ratings yet
- BRCA in Premenopausal Breast CancerDocument8 pagesBRCA in Premenopausal Breast CancerErwin Chiquete, MD, PhDNo ratings yet
- Cardiac Pathology 6 Months After Hospitalization For COVID-19 and Association With The Acute Disease SeverityDocument11 pagesCardiac Pathology 6 Months After Hospitalization For COVID-19 and Association With The Acute Disease SeverityArdhia Kusuma PutriNo ratings yet
- Ijmsv 14 P 1241Document10 pagesIjmsv 14 P 1241Milan PetrikNo ratings yet
- COVID-19 Update: Covid-19-Associated Coagulopathy: Richard C. BeckerDocument14 pagesCOVID-19 Update: Covid-19-Associated Coagulopathy: Richard C. Beckersumenep nursalamNo ratings yet
- Neurosurg Focus Article Pe9Document10 pagesNeurosurg Focus Article Pe9ropelessgerm12No ratings yet
- Update On The Neurology of COVID 19: LettertotheeditorDocument3 pagesUpdate On The Neurology of COVID 19: Lettertotheeditorgevowo3277No ratings yet
- Canavero, Isabella 2016 - GAK - Data HF TDK Ada, AF Neg TDK AdaDocument12 pagesCanavero, Isabella 2016 - GAK - Data HF TDK Ada, AF Neg TDK AdahavanaesterNo ratings yet
- Clinica ArticuloDocument10 pagesClinica Articulojoel PeraltaNo ratings yet
- Prognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19Document15 pagesPrognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19Basilio BabarNo ratings yet
- Jurnal RDocument2 pagesJurnal RALberta YosheNo ratings yet
- Initial Loss of Consciousness and Risk of Delayed Cerebral Ischemia After Aneurysmal Subarachnoid HemorrhageDocument8 pagesInitial Loss of Consciousness and Risk of Delayed Cerebral Ischemia After Aneurysmal Subarachnoid HemorrhageAzka SamalNo ratings yet
- Clinical Characteristics and Risk Factors of Cardiac Involvement in COVID-19Document11 pagesClinical Characteristics and Risk Factors of Cardiac Involvement in COVID-19Yerlis OspinoNo ratings yet
- Epidemiology of Covid - 19 Hemodialysis Patients at The Military Hospital of RabatDocument7 pagesEpidemiology of Covid - 19 Hemodialysis Patients at The Military Hospital of RabatIJAR JOURNALNo ratings yet
- Infective EndocarditisDocument5 pagesInfective Endocarditismustafa malvi100% (1)
- Accepted: Title: COVID-19 Infection Associated With Encephalitis in An AdolescentDocument13 pagesAccepted: Title: COVID-19 Infection Associated With Encephalitis in An AdolescentLia NadaNo ratings yet
- Unusual Pattern of Arterial Macrothrombosis Causing Stroke in A Young Adult Recovered From COVID-19Document5 pagesUnusual Pattern of Arterial Macrothrombosis Causing Stroke in A Young Adult Recovered From COVID-19Audrey Beatrice ReyesNo ratings yet
- Bilateral Pulmonary Embolism Mimicking Acute Chest Syndrome in A Patient With Sickle Cell Disease: Acase Report and Review of The LiteratureDocument4 pagesBilateral Pulmonary Embolism Mimicking Acute Chest Syndrome in A Patient With Sickle Cell Disease: Acase Report and Review of The LiteratureIJAR JOURNALNo ratings yet
- SARS-CoV-2 Viremia Is Associated With Distinct Proteomic Pathways and Predicts COVID-19 OutcomesDocument13 pagesSARS-CoV-2 Viremia Is Associated With Distinct Proteomic Pathways and Predicts COVID-19 OutcomesYoga Nugraha WNo ratings yet
- Artigo Neuromeningeal Cryptococcosis in A Patient Not Infected With HumanDocument4 pagesArtigo Neuromeningeal Cryptococcosis in A Patient Not Infected With HumanRENATA SANTOS ASSUNCAONo ratings yet
- Abstak Neurointervention EditDocument2 pagesAbstak Neurointervention Editzefri suhendarNo ratings yet
- 2017 Article 777Document10 pages2017 Article 777wlNo ratings yet
- Large Vessel Occlusion Secondary To COVID-19 Hypercoagulability in A Young Patient: A Case Report and Literature ReviewDocument6 pagesLarge Vessel Occlusion Secondary To COVID-19 Hypercoagulability in A Young Patient: A Case Report and Literature Reviewdevi ramadiantiNo ratings yet
- Case 17-2020: A 68-Year-Old Man With Covid-19 and Acute Kidney InjuryDocument10 pagesCase 17-2020: A 68-Year-Old Man With Covid-19 and Acute Kidney Injurymichal ben meronNo ratings yet
- Actionable Diagnosis of Neuroleptospirosis by Next-Generation SequencingDocument10 pagesActionable Diagnosis of Neuroleptospirosis by Next-Generation SequencingJorge AlvarezNo ratings yet
- 2021 Acute Respiratory Distress Syndrome Update, WDocument8 pages2021 Acute Respiratory Distress Syndrome Update, WOLIVERA MOLLINEDO CAMILA ZESIANo ratings yet
- Prune BellyDocument4 pagesPrune BellyErwin Chiquete, MD, PhDNo ratings yet
- Myocarditis After Covid-19 Vaccination in A Large Health Care OrganizationDocument8 pagesMyocarditis After Covid-19 Vaccination in A Large Health Care OrganizationPDFReadAndDevelopNo ratings yet
- 1.1 CovidakiDocument10 pages1.1 CovidakiKev Jose Ruiz RojasNo ratings yet
- YessDocument5 pagesYessalingh98No ratings yet
- Cardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesFrom EverandCardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesNo ratings yet
- 14 Best Hypoallergenic Cat BreedDocument11 pages14 Best Hypoallergenic Cat BreedJunna May AradoNo ratings yet
- Kuji-In Overview - 9 Hand SealsDocument12 pagesKuji-In Overview - 9 Hand SealsRecuperatu Mente100% (1)
- Flangeless Horseshoe Maxillary Complete Denture - A Prosthodontic Solution To Maxillary ToriDocument3 pagesFlangeless Horseshoe Maxillary Complete Denture - A Prosthodontic Solution To Maxillary ToriMohammad Abdulmon’emNo ratings yet
- +3 Arts&Science UN Trained IIDocument270 pages+3 Arts&Science UN Trained IIAmarendra OjhaNo ratings yet
- Robert J Wieland BooksDocument2 pagesRobert J Wieland BooksRamon Guzmán CNo ratings yet
- Fresh Foods Ordering ProcessDocument5 pagesFresh Foods Ordering ProcessSagarPatelNo ratings yet
- Coop Learning ActivitiesDocument198 pagesCoop Learning ActivitiesJanine Mosca GonzalesNo ratings yet
- G.R. No. 203986 PEOPLE Vs JERSON DASMARINAS GONZALESDocument16 pagesG.R. No. 203986 PEOPLE Vs JERSON DASMARINAS GONZALESRuel FernandezNo ratings yet
- On Double Laplace Transform and Double Sumudu TransformDocument6 pagesOn Double Laplace Transform and Double Sumudu TransformAJER JOURNALNo ratings yet
- 5kV 10kV Test Lead An en V01Document16 pages5kV 10kV Test Lead An en V01Vishwanath TodurkarNo ratings yet
- Vonoprazan: A Novel and Potent Alternative in The Treatment of Acid Related DiseasesDocument10 pagesVonoprazan: A Novel and Potent Alternative in The Treatment of Acid Related DiseasesmNo ratings yet
- Unfe 65 Intersex Factsheet ENGLISHDocument2 pagesUnfe 65 Intersex Factsheet ENGLISHRinio SimeonidouNo ratings yet
- ST Clare PrayersDocument3 pagesST Clare PrayersLiza Lauriana D'SouzaNo ratings yet
- Affidavit Lost StockDocument4 pagesAffidavit Lost StockRon DiMambroNo ratings yet
- How To Maintain Throat HygieneDocument9 pagesHow To Maintain Throat Hygieneankita singhNo ratings yet
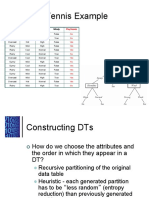
- Play Tennis Example: Outlook Temperature Humidity WindyDocument29 pagesPlay Tennis Example: Outlook Temperature Humidity Windyioi123No ratings yet
- Benford's Law For Auditors: Overview and The BasicsDocument42 pagesBenford's Law For Auditors: Overview and The BasicsPolizeroNo ratings yet
- THE UlTIMATE SAFARIDocument5 pagesTHE UlTIMATE SAFARIapi-19776105100% (1)
- What Is Special EducationDocument2 pagesWhat Is Special EducationImelda Nantin GarciaNo ratings yet
- Kisi Kisi B.inggris Pts Sem 1 Kelas 9Document5 pagesKisi Kisi B.inggris Pts Sem 1 Kelas 9Stevany TracysiliaNo ratings yet
- Tutorial QuestionsDocument6 pagesTutorial QuestionsEribeta TeiaNo ratings yet
- Feature Writing HandoutDocument54 pagesFeature Writing HandoutRose Liren LabradorNo ratings yet
- Seismic Waves Grade 10 Cont - EarthquakeDocument48 pagesSeismic Waves Grade 10 Cont - EarthquakeClaudette Mae NazNo ratings yet
- Alignment GPC and UNSPSCDocument17 pagesAlignment GPC and UNSPSCputrinatariNo ratings yet
- The Ghost HunterDocument175 pagesThe Ghost HunterjoyNo ratings yet
- Advanced 1 Midterm Written BDocument6 pagesAdvanced 1 Midterm Written BCarolina Aguido FerreiraNo ratings yet
- PAT Bhs Inggris VIIDocument4 pagesPAT Bhs Inggris VIIMtss Zainul BaharNo ratings yet
- Ejercicios PE (Resueltos)Document14 pagesEjercicios PE (Resueltos)Monserrat50% (4)