Download as pdf or txt
You might also like
- School Counseling Core Curriculum Action Plan (Career)Document1 pageSchool Counseling Core Curriculum Action Plan (Career)Cristina VasquezNo ratings yet
- Sensory Systems Guide - The OT ButterflyDocument13 pagesSensory Systems Guide - The OT ButterflyMartha Patricia López Pimentel100% (1)
- ANT - DX-1710-2690-65-18i-M-R - (A264518R0v01-1881) DatasheetDocument2 pagesANT - DX-1710-2690-65-18i-M-R - (A264518R0v01-1881) DatasheetDayane Thiere100% (1)
- Ali, P. 2008. Professional Development and The Role of Mentorship. Nursing StandardDocument5 pagesAli, P. 2008. Professional Development and The Role of Mentorship. Nursing Standardsiti akbariNo ratings yet
- MuboboboDocument8 pagesMuboboboMartín Real L.No ratings yet
- Electromagnetic Interference and CompatibilityDocument10 pagesElectromagnetic Interference and CompatibilityYuvaraja50% (2)
- Effective Classroom ManagementDocument24 pagesEffective Classroom ManagementAmbrosious100% (1)
- 4-The Problem and Power of ProfessionalismDocument10 pages4-The Problem and Power of Professionalismzoghbi.antoinette42No ratings yet
- Ericsson 2000Document34 pagesEricsson 2000PabloNo ratings yet
- Informal Mentoring Between Faculty and Medical.7Document5 pagesInformal Mentoring Between Faculty and Medical.7dettolittaNo ratings yet
- BrochureDocument1 pageBrochureSa Rah Kamad DagendelNo ratings yet
- Does Mindfulness Training Enhance The Professional Development of Residents? A Qualitative StudyDocument6 pagesDoes Mindfulness Training Enhance The Professional Development of Residents? A Qualitative StudySeda Şahin ÖnerNo ratings yet
- Boundaries, Multiple Roles, and The Professional RelationshipDocument37 pagesBoundaries, Multiple Roles, and The Professional RelationshipMuhammad Abuelezz100% (1)
- Walkthrough Matrix: Ecotech Center, Lahug, Cebu City October 11-13, 2017Document8 pagesWalkthrough Matrix: Ecotech Center, Lahug, Cebu City October 11-13, 2017Queenie Marie Obial AlasNo ratings yet
- Perspective The Doctor As Performer A Proposal.40Document5 pagesPerspective The Doctor As Performer A Proposal.40Monique VandresenNo ratings yet
- Diass MelcsDocument7 pagesDiass MelcsbeatrizmariemaranguitNo ratings yet
- Relacion Entre El Burnout y Estudiantes de Medicina HumanaDocument4 pagesRelacion Entre El Burnout y Estudiantes de Medicina HumanaJair Benavente AsinNo ratings yet
- Competency in Conducting Cognitive-Behavioral Therapy Foundational, Functional, and Supervisory AspectsDocument8 pagesCompetency in Conducting Cognitive-Behavioral Therapy Foundational, Functional, and Supervisory AspectsCeeta IndustriesNo ratings yet
- Data On Diversity Journal ArticleDocument11 pagesData On Diversity Journal ArticlekavinpobpraserttanakitNo ratings yet
- Coaching Versus Therapy: A PerspectiveDocument9 pagesCoaching Versus Therapy: A PerspectivePuljić DragoNo ratings yet
- ExpertiseDocument13 pagesExpertiseOlya TsarevNo ratings yet
- Educ 704 - Career Intervention Action PlanDocument2 pagesEduc 704 - Career Intervention Action Planapi-402457653No ratings yet
- Examining Per-Pro Distinction With ApaDocument10 pagesExamining Per-Pro Distinction With Apaapi-683959564No ratings yet
- 5C003 - Learner Assignment Guidance - Handout - V1Document13 pages5C003 - Learner Assignment Guidance - Handout - V1sorlen008No ratings yet
- Level 1 Student Perceptions About Employability Career Planning and Careers GuidanceDocument3 pagesLevel 1 Student Perceptions About Employability Career Planning and Careers GuidanceLoredanaLola93No ratings yet
- Parting The Clouds Three Professionalism.14Document6 pagesParting The Clouds Three Professionalism.14Giancarlo Becerra BravoNo ratings yet
- Statement of The Problem Statistical Treatment FindingsDocument6 pagesStatement of The Problem Statistical Treatment Findingsangelo36No ratings yet
- Catch Up Friday Gr9 Feb 23Document4 pagesCatch Up Friday Gr9 Feb 23milafer dabanNo ratings yet
- Evolution of Nursing Science ImplicationDocument5 pagesEvolution of Nursing Science ImplicationKhadira MohammedNo ratings yet
- Pink Pastel Textured Compay Mind Map BrainstormDocument2 pagesPink Pastel Textured Compay Mind Map BrainstormWindhy CabadingNo ratings yet
- Career MobDocument23 pagesCareer Mobbinaysah18No ratings yet
- Dominance of The Leptoprosopic Face and Mesorrhine.40-1Document3 pagesDominance of The Leptoprosopic Face and Mesorrhine.40-1Godwin SundayNo ratings yet
- Career Ability Placement Surveyfor High School StudentsDocument9 pagesCareer Ability Placement Surveyfor High School StudentsSara RahmanNo ratings yet
- Gráfico Cuadro Comparativo Moderno Juvenil Azul y RosaDocument7 pagesGráfico Cuadro Comparativo Moderno Juvenil Azul y RosaCELENIA BELEN TOAPANTA CAUJANo ratings yet
- DonaldHSaklofsk 2013 22FormalMethodsInAsse TheOxfordHandbookOfCh PDFDocument36 pagesDonaldHSaklofsk 2013 22FormalMethodsInAsse TheOxfordHandbookOfCh PDFAndy MirandaNo ratings yet
- Definition of Nursing According To TheoristsDocument2 pagesDefinition of Nursing According To TheoristsScribdTranslationsNo ratings yet
- ABECourse SyllabusDocument9 pagesABECourse SyllabusCarlo GuinitaNo ratings yet
- Trimex-Ied-Bsba 2019Document163 pagesTrimex-Ied-Bsba 2019ErichSantosValdeviesoNo ratings yet
- A New Era in Graduate Medical Education A Novel.33Document3 pagesA New Era in Graduate Medical Education A Novel.33drhusseinfaour3126No ratings yet
- PR 1 Rol Matrix TemplateDocument8 pagesPR 1 Rol Matrix TemplateMjhay AguilarNo ratings yet
- Older People's Experiences of Falling and Perceived Risk of Falls in The CommunityDocument1 pageOlder People's Experiences of Falling and Perceived Risk of Falls in The Communitysabao kizuiteNo ratings yet
- Course Outline DIASSDocument5 pagesCourse Outline DIASScindy juntongNo ratings yet
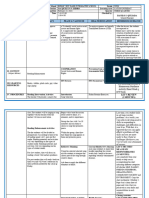
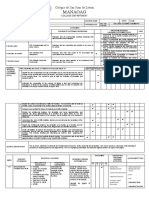
- Manaoag: Colegio de San Juan de LetranDocument8 pagesManaoag: Colegio de San Juan de LetranEugene A. EstacioNo ratings yet
- Expertise: K. Anders Ericsson and Tyler J. TowneDocument13 pagesExpertise: K. Anders Ericsson and Tyler J. TowneaudreyvaniasonjayaNo ratings yet
- Syllabus-OBE - Ge 6 Art Appreciation BUSINESS ADMINISTRATIONDocument11 pagesSyllabus-OBE - Ge 6 Art Appreciation BUSINESS ADMINISTRATIONVanessa L. VinluanNo ratings yet
- Grade 11 Catch Up FridayDocument5 pagesGrade 11 Catch Up FridayMELISSA NANONGNo ratings yet
- Counselling Session-2Document1 pageCounselling Session-2dezeulNo ratings yet
- Survey Research.32Document9 pagesSurvey Research.32Una LeymanNo ratings yet
- Guidelines and Essential Elements For PrebriefingDocument6 pagesGuidelines and Essential Elements For PrebriefingStibaliz Beristain SánchezNo ratings yet
- Birla Institute of Technology and Science, Pilani: Pilani Campus AUGS/ AGSR DivisionDocument6 pagesBirla Institute of Technology and Science, Pilani: Pilani Campus AUGS/ AGSR DivisionHarshNo ratings yet
- 1994, David Roland - How Professional Performers Manage Performance AnxietyDocument11 pages1994, David Roland - How Professional Performers Manage Performance AnxietyEko A. SaputroNo ratings yet
- 2023 Passalacqua ExpertiseDocument10 pages2023 Passalacqua Expertisedario susanoNo ratings yet
- Psychological LiteracyDocument10 pagesPsychological LiteracyViktorija PetunovaNo ratings yet
- Acis 3Document9 pagesAcis 3Maryam AlkanderyNo ratings yet
- Local Media7579940144065994400Document16 pagesLocal Media7579940144065994400Leonel James SuraltaNo ratings yet
- The Habits of Mind: Frameworks BriefsDocument6 pagesThe Habits of Mind: Frameworks BriefsAntonioNo ratings yet
- Personality Assessment and CarDocument24 pagesPersonality Assessment and CarraminemekNo ratings yet
- The Key Informat TechniqueDocument6 pagesThe Key Informat TechniquePierina FrancoNo ratings yet
- Professionalism in The Dental Office, Part One: I Chairside Conscience IDocument3 pagesProfessionalism in The Dental Office, Part One: I Chairside Conscience IKingjokerNo ratings yet
- Curriculum VitaeDocument2 pagesCurriculum VitaeSAIMA SHAHZADINo ratings yet
- What Is Professionalism in Occupational Therapy? A Concept AnalysisDocument14 pagesWhat Is Professionalism in Occupational Therapy? A Concept AnalysisNataliaNo ratings yet
- Expertise in Psychotherapy An Elusive GoalDocument14 pagesExpertise in Psychotherapy An Elusive Goalpuntasabiertas106No ratings yet
- Reflections of A Gay Male PsychotherapistDocument9 pagesReflections of A Gay Male PsychotherapistJulio César Cristancho GarcíaNo ratings yet
- Planning 10th-1qDocument1 pagePlanning 10th-1qAbigail Sisalema BastidasNo ratings yet
- The Models of Skill Acquisition and Expertise Development: A Quick Reference of SummariesFrom EverandThe Models of Skill Acquisition and Expertise Development: A Quick Reference of SummariesNo ratings yet
- 53VML 30MV Ball Float Vent ValvesDocument2 pages53VML 30MV Ball Float Vent ValvesJose DevilzeusNo ratings yet
- Kemasan HNA NO Produk SyrupDocument2 pagesKemasan HNA NO Produk SyruprianNo ratings yet
- Personal Hygiene: How To Keep Your Body CleanDocument13 pagesPersonal Hygiene: How To Keep Your Body CleanneleaNo ratings yet
- Engines MaterialsDocument20 pagesEngines MaterialsMarkos100% (1)
- Recycling Wastes Into Valuable Organic fertilizers:VERMICOMPOSTINGDocument9 pagesRecycling Wastes Into Valuable Organic fertilizers:VERMICOMPOSTINGMuhammad ShayanNo ratings yet
- Obsessive Love - WikipediaDocument3 pagesObsessive Love - WikipediaIslam AhmedNo ratings yet
- ISO 9001-2000 Training (Engl)Document61 pagesISO 9001-2000 Training (Engl)Mihai Florin IacobescuNo ratings yet
- Aquac Uno HDocument218 pagesAquac Uno Hivancalderon867374No ratings yet
- Maui ProjectDocument2 pagesMaui Projectapi-358478577No ratings yet
- Wordlist Level2Document3 pagesWordlist Level2SamiyaNo ratings yet
- Autodesk BuildDocument53 pagesAutodesk BuildSturla SighvatssonNo ratings yet
- CL-1200i (1000P) &2600i&2800i - Service Manual - V1.0 - ENDocument803 pagesCL-1200i (1000P) &2600i&2800i - Service Manual - V1.0 - ENmanal al-hattaliNo ratings yet
- Cellular RespirationDocument10 pagesCellular RespirationXavier LecarosNo ratings yet
- Adaptation To Physical Environment: Climate, Water, and SoilDocument52 pagesAdaptation To Physical Environment: Climate, Water, and SoilClarkNo ratings yet
- Problem Set No.1Document3 pagesProblem Set No.1paolo sulitNo ratings yet
- GSG 300 EditedDocument10 pagesGSG 300 Editedvtz2ruhNo ratings yet
- Amet MajestyDocument3 pagesAmet MajestySR MonicasreeNo ratings yet
- Geography Chapter 7 Land SupplyDocument9 pagesGeography Chapter 7 Land SupplydenrabyNo ratings yet
- HECAT Module AODDocument26 pagesHECAT Module AODririhenaNo ratings yet
- Penguin - Magnetic Drive Pump M SeiresDocument4 pagesPenguin - Magnetic Drive Pump M SeiresMiguel Angel LòpezNo ratings yet
- NSK Wheel Bearings: Produced Worldwide To One StandardDocument6 pagesNSK Wheel Bearings: Produced Worldwide To One StandardCarlo AguiluzNo ratings yet
- 333 Obooko thr0019Document507 pages333 Obooko thr0019ripak_debnathNo ratings yet
- Design of A Solar Absorption Cooling System in A Greek Hospital PDFDocument8 pagesDesign of A Solar Absorption Cooling System in A Greek Hospital PDFYazid Al ShehriNo ratings yet
- QM 34 - TanksDocument10 pagesQM 34 - Tanksmohamed elmasryNo ratings yet
- Msc1813ep MeduDocument2 pagesMsc1813ep MedumichaelsudjonoNo ratings yet