Download as pdf or txt
You might also like
- Bishop Rehabilitation Inspection ReportDocument18 pagesBishop Rehabilitation Inspection ReportJames MulderNo ratings yet
- Bankarts LesionDocument6 pagesBankarts Lesionkrissh20No ratings yet
- All Arthroscopic Anatomic Repair of An Avulsed Popliteus Tendon in A Multiple Ligamentinjured KneeDocument4 pagesAll Arthroscopic Anatomic Repair of An Avulsed Popliteus Tendon in A Multiple Ligamentinjured Kneechandan noelNo ratings yet
- 4 Arthroscopic Bankart Repair With Inferior To Superior Capsular Shift in Lateral Decubitus Position 1723226228Document6 pages4 Arthroscopic Bankart Repair With Inferior To Superior Capsular Shift in Lateral Decubitus Position 1723226228César ArveláezNo ratings yet
- Arthroscopic Treatment of A Reverse Hill-Sachs Lesion: Richard E. Duey, M.D., and Stephen S. Burkhart, M.DDocument5 pagesArthroscopic Treatment of A Reverse Hill-Sachs Lesion: Richard E. Duey, M.D., and Stephen S. Burkhart, M.DArisKumarNo ratings yet
- Operative Approaches For Total HipDocument9 pagesOperative Approaches For Total HipEduardo GonzalezNo ratings yet
- Arthroscopic Recognition and Repair or The Torn Subescapulari TendonDocument7 pagesArthroscopic Recognition and Repair or The Torn Subescapulari TendonNashNo ratings yet
- Management of Anterior Shoulder Instability Without Bone Loss: Arthroscopic and Mini-Open TechniquesDocument7 pagesManagement of Anterior Shoulder Instability Without Bone Loss: Arthroscopic and Mini-Open TechniquesHari WangsaNo ratings yet
- 1 s2.0 S2212628719301665 MainDocument4 pages1 s2.0 S2212628719301665 MainRafael Jardim de MouraNo ratings yet
- Microsurgery: Medial Plantar Flap For Reconstruction of Heel DefectDocument5 pagesMicrosurgery: Medial Plantar Flap For Reconstruction of Heel DefectRazaria DailyneNo ratings yet
- I. Introduction To The Upper ExtremityDocument10 pagesI. Introduction To The Upper ExtremityKailash KhatriNo ratings yet
- Dryer1980 1Document2 pagesDryer1980 1Dr LAUMONERIENo ratings yet
- Long Head Biceps Tendondnatural Patch For Massive Irreparable Rotator Cuff TearsDocument6 pagesLong Head Biceps Tendondnatural Patch For Massive Irreparable Rotator Cuff TearsDita Putri DamayantiNo ratings yet
- Triceps Rupture After Olecranon Fixation With Proximal Ulna Plate and Suture AugmentationDocument5 pagesTriceps Rupture After Olecranon Fixation With Proximal Ulna Plate and Suture AugmentationSiddharth AgrawalNo ratings yet
- Mini Open Arthroscopically Assisted BrisDocument6 pagesMini Open Arthroscopically Assisted BrisBruno EstevesNo ratings yet
- What Process Is Best Seen Using A Perpendicular CR With The Elbow in Acute Flexion and With The Posterior Aspect of The Humerus Adjacent To The Image ReceptorDocument22 pagesWhat Process Is Best Seen Using A Perpendicular CR With The Elbow in Acute Flexion and With The Posterior Aspect of The Humerus Adjacent To The Image ReceptorKalpana ParajuliNo ratings yet
- Direct Anterior Total Hip ArthroplastyDocument13 pagesDirect Anterior Total Hip Arthroplasty21701101006 Rosita SariNo ratings yet
- Subtalar Arthrodesis Van Dijck 2012Document7 pagesSubtalar Arthrodesis Van Dijck 2012liviu tomoiagaNo ratings yet
- Recurrent Traumatic Elbow Dislocation: Francis M.DDocument4 pagesRecurrent Traumatic Elbow Dislocation: Francis M.DDr LAUMONERIENo ratings yet
- Posterior Approaches To The Tibial PlateauDocument5 pagesPosterior Approaches To The Tibial Plateauana starcevicNo ratings yet
- Hardinge ModifiedDocument5 pagesHardinge ModifiedscribdfoaktNo ratings yet
- Knot Induced Glenoid Erosion JSES 2006Document3 pagesKnot Induced Glenoid Erosion JSES 2006harpreet singhNo ratings yet
- Fractures of The Scapula: Charles D. NewtonDocument12 pagesFractures of The Scapula: Charles D. NewtonasheneyNo ratings yet
- Anatomy of The Terminal Branch of The Posterior Circumflex Humeral ArteryDocument4 pagesAnatomy of The Terminal Branch of The Posterior Circumflex Humeral ArterymotohumeresNo ratings yet
- Johnson 2005Document2 pagesJohnson 2005dgmf999No ratings yet
- Thaker 2021Document5 pagesThaker 2021Maria Jonnalin SantosNo ratings yet
- Tendon Transfers For Lateral Pinch: Albert A. Weiss, MD, and Scott H. Kozin, MDDocument11 pagesTendon Transfers For Lateral Pinch: Albert A. Weiss, MD, and Scott H. Kozin, MDFernando Martín Arce AlvaNo ratings yet
- A Posterosuperior Approach To The ShoulderDocument5 pagesA Posterosuperior Approach To The ShoulderEllan Giulianno FerreiraNo ratings yet
- Nonoperative and Operative Management ofDocument12 pagesNonoperative and Operative Management ofVladislav KotovNo ratings yet
- Shoulder Arthroplasty Neer 1955Document13 pagesShoulder Arthroplasty Neer 1955Jorge LourençoNo ratings yet
- PCL's Avulsion FractureDocument22 pagesPCL's Avulsion FractureNey da OnneyNo ratings yet
- Achot 2016 3 141 146Document6 pagesAchot 2016 3 141 146Christopher Freddy Bermeo RiveraNo ratings yet
- Aaos 2002Document120 pagesAaos 2002Yusufa ArdyNo ratings yet
- Arthroscopic "Panorama" View of The Subacromial Space Via Deltoid Fascia ReleaseDocument5 pagesArthroscopic "Panorama" View of The Subacromial Space Via Deltoid Fascia ReleaseMoustafa MohamedNo ratings yet
- THR Surgical ApproachesDocument5 pagesTHR Surgical ApproachesMaria Magdalena SmeuNo ratings yet
- Occipital Bi-Transtentorial-Falcine Approach For Falcotentorial MeningiomaDocument3 pagesOccipital Bi-Transtentorial-Falcine Approach For Falcotentorial MeningiomaMarcelo LambertiNo ratings yet
- Arthroscopic Ramp Repair No-Implant, Pass, Park, and Tie Technique Using Knee Scorpion, GustaDocument8 pagesArthroscopic Ramp Repair No-Implant, Pass, Park, and Tie Technique Using Knee Scorpion, GustaAlhoi lesley davidsonNo ratings yet
- Arthroscopic-Assisted Pectoralis Minor Transfer For Irreparable Anterosuperior Massive Rotator Cuff TearDocument6 pagesArthroscopic-Assisted Pectoralis Minor Transfer For Irreparable Anterosuperior Massive Rotator Cuff TearGabriel Arturo Lorca OsorioNo ratings yet
- Johnson 2005Document2 pagesJohnson 2005dgmf999No ratings yet
- Arthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalDocument6 pagesArthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalMoustafa MohamedNo ratings yet
- Title of OperationDocument4 pagesTitle of Operationjanice aguilarNo ratings yet
- The Use of A Reverse Flow Sural Fasciocutaneous Flap in A Patient With Multiple Trauma: A CaseDocument5 pagesThe Use of A Reverse Flow Sural Fasciocutaneous Flap in A Patient With Multiple Trauma: A CasewennyNo ratings yet
- Far-Lateral Approach: Alhakam Abd Almawla M.D., M.SC., D.Sc. Professor of Neurosurgery Damascus UniversityDocument10 pagesFar-Lateral Approach: Alhakam Abd Almawla M.D., M.SC., D.Sc. Professor of Neurosurgery Damascus UniversityNadia BordaşNo ratings yet
- CHAPTER 19 - Mini Open Rota - 2008 - Surgical Techniques of The Shoulder ElbowDocument7 pagesCHAPTER 19 - Mini Open Rota - 2008 - Surgical Techniques of The Shoulder ElbowJaime Vázquez ZárateNo ratings yet
- Endoscopic Calcaneoplasty Combined With Achilles Tendon RepairDocument4 pagesEndoscopic Calcaneoplasty Combined With Achilles Tendon RepairHumza ZahidNo ratings yet
- Grashey ViewDocument23 pagesGrashey Viewsindami.nabilaNo ratings yet
- Youngszalay 2002Document5 pagesYoungszalay 2002Morozovschi VitalieNo ratings yet
- 1 s2.0 S2212628723001974 MainDocument9 pages1 s2.0 S2212628723001974 MainRonald QuezadaNo ratings yet
- Werner2006 2 PDFDocument5 pagesWerner2006 2 PDFAlexandraNo ratings yet
- Eightball Corner PocketDocument2 pagesEightball Corner Pocketpradeep danielNo ratings yet
- Ijar JournalDocument4 pagesIjar JournalGuna NikhilNo ratings yet
- Leech Aveng Von Gs 2016Document12 pagesLeech Aveng Von Gs 2016Andrés Urrego NietoNo ratings yet
- Analysis of A Retrieved Delta III Total Shoulder ProsthesisDocument5 pagesAnalysis of A Retrieved Delta III Total Shoulder ProsthesisS.ENo ratings yet
- Bladder Exstrophy and Epispadias: Dominic Frimberger, John P. GearhartDocument18 pagesBladder Exstrophy and Epispadias: Dominic Frimberger, John P. Gearhartranz ibonkNo ratings yet
- J Neurosurg Case Lessons Article CASE2190Document4 pagesJ Neurosurg Case Lessons Article CASE2190chaiimaefrNo ratings yet
- Johnson 2005Document2 pagesJohnson 2005dgmf999No ratings yet
- A Modified Direct Lateral Approach in Total Hip ArthroplastyDocument5 pagesA Modified Direct Lateral Approach in Total Hip ArthroplastyAbhishek JirelNo ratings yet
- Buccinator Myomucosal Flap-1Document6 pagesBuccinator Myomucosal Flap-1JamesNo ratings yet
- Scapular Dyskinesia, The Forgotten Culprit of Shoulder Pain and How To RehabilitateDocument6 pagesScapular Dyskinesia, The Forgotten Culprit of Shoulder Pain and How To RehabilitateQuiroprácticaParaTodosNo ratings yet
- Posterior Iliac Crest Bone HarvestDocument7 pagesPosterior Iliac Crest Bone HarvestDiego Rivas-VazquezNo ratings yet
- LumbarDocument8 pagesLumbarokirby6No ratings yet
- Fiqh Al AmraadhDocument27 pagesFiqh Al AmraadhtisuchiNo ratings yet
- Ruinous A Dark Paranormal Romance The Marked Mage Chronicles Book 4 Victoria Evers All ChapterDocument67 pagesRuinous A Dark Paranormal Romance The Marked Mage Chronicles Book 4 Victoria Evers All Chaptermichael.canela199100% (10)
- Harga RadiologiDocument4 pagesHarga RadiologiyennyNo ratings yet
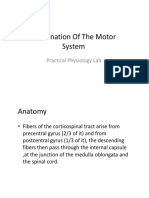
- Examination of The Motor System: Practical Physiology LabDocument20 pagesExamination of The Motor System: Practical Physiology Labحسين سعد حاتم خضيرNo ratings yet
- Lab No4Document5 pagesLab No4Usama JavedNo ratings yet
- Remedies Available in TortDocument7 pagesRemedies Available in TortNO ONE MENo ratings yet
- A Light in The Void PDFDocument348 pagesA Light in The Void PDFBaby GeoNo ratings yet
- 2 ConstructionsafetyDocument51 pages2 ConstructionsafetyMicar MicarNo ratings yet
- High-Yield Anatomy Notes For FCPS Part 1 (MUST HAVE)Document12 pagesHigh-Yield Anatomy Notes For FCPS Part 1 (MUST HAVE)Dr-Sanjay SinghaniaNo ratings yet
- Human Body and Skeleton Medical VocabularyDocument3 pagesHuman Body and Skeleton Medical VocabularyanaNo ratings yet
- Short Communication Walking Index For Spinal Cord Injury (WISCI II) : Scale RevisionDocument3 pagesShort Communication Walking Index For Spinal Cord Injury (WISCI II) : Scale RevisionКазанцева АсяNo ratings yet
- 11 Organ SystemsDocument2 pages11 Organ Systemsjonar parinasNo ratings yet
- Temporomandibular Joint Clinical AnatomyDocument43 pagesTemporomandibular Joint Clinical AnatomyPriyaNo ratings yet
- Reading 2 Chapter 3Document2 pagesReading 2 Chapter 3Vinh HuỳnhNo ratings yet
- Female PelvisDocument37 pagesFemale Pelvismedical chroniclesNo ratings yet
- Pedrettis Occupational Therapy Practice Skills For Physical Dysfunction 7th Edition Pendleton Test BankDocument25 pagesPedrettis Occupational Therapy Practice Skills For Physical Dysfunction 7th Edition Pendleton Test BankStaceyBellewax100% (45)
- Elbow ComplexDocument17 pagesElbow ComplexLeslie RognstadNo ratings yet
- Early Management: Admit To Burns UnitDocument1 pageEarly Management: Admit To Burns UnitErica A. Gallegos AriasNo ratings yet
- Footmotion Plating System Brochure PDFDocument9 pagesFootmotion Plating System Brochure PDFavillouNo ratings yet
- Ankle-Foot OrthosesDocument8 pagesAnkle-Foot OrthosesSangeetha GnaneswaranNo ratings yet
- Head Injury PPT 160219094543Document49 pagesHead Injury PPT 160219094543Claire De VeraNo ratings yet
- Recalls of Paper 2 - 11/9/2018: ConsentDocument6 pagesRecalls of Paper 2 - 11/9/2018: ConsentGiovanni Henry0% (1)
- ISPO Classification System For Congenital Upper Limb ReductionsDocument1 pageISPO Classification System For Congenital Upper Limb ReductionswinNo ratings yet
- Cusi v. Philippine National RailwaysDocument12 pagesCusi v. Philippine National Railwaysjames lebronNo ratings yet
- Group3 Duaplex360-032222Document6 pagesGroup3 Duaplex360-032222lumley beachNo ratings yet
- Workcover Guides Evaluation Permanent Impairment 3rd Edition 0970Document104 pagesWorkcover Guides Evaluation Permanent Impairment 3rd Edition 0970workcovervictim8242No ratings yet
- Trauma Conclave 2021 - Agenda Without LinkDocument2 pagesTrauma Conclave 2021 - Agenda Without LinkDebangshu KumarNo ratings yet
- Cranial NervesDocument14 pagesCranial NervesAdrija ChatterjeeNo ratings yet