
Mono100a-17 New
Mono100a-17 New
You might also like
- Lecture 25 - LipidsDocument58 pagesLecture 25 - Lipidsapi-19824406No ratings yet
- Synthesis and Aromatase Inhibition by Potential Metabolites of Exemestane (6-Methylenandrosta-L, 4-Diene-3,17-Dione)Document6 pagesSynthesis and Aromatase Inhibition by Potential Metabolites of Exemestane (6-Methylenandrosta-L, 4-Diene-3,17-Dione)Nimra Naveed ShaikhNo ratings yet
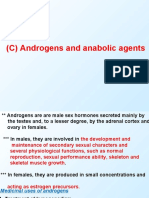
- (C) Androgens and Anabolic AgentsDocument24 pages(C) Androgens and Anabolic AgentsIsmail MustafaNo ratings yet
- Chapter 1 Definition and Classification of Lipids 1972Document51 pagesChapter 1 Definition and Classification of Lipids 1972aldofedeuriel152005No ratings yet
- (2022 11 10) 張訓碩-生藥學 (terpenoids)Document49 pages(2022 11 10) 張訓碩-生藥學 (terpenoids)tw910124No ratings yet
- Untul Pamantului ArticoleDocument2 pagesUntul Pamantului ArticoleRoxana FloreaNo ratings yet
- Organic ChemistryDocument44 pagesOrganic ChemistryKushashwa Ravi ShrimaliNo ratings yet
- ZZZ (0) Modified Trichothecenes (XXXX 325)Document24 pagesZZZ (0) Modified Trichothecenes (XXXX 325)amaroluisNo ratings yet
- Biosintesis of TerpenoidDocument19 pagesBiosintesis of TerpenoidIntanFrinaUtamiyantiNo ratings yet
- SurfactantsDocument11 pagesSurfactantstNo ratings yet
- Aplikasi Kromatografi GasDocument7 pagesAplikasi Kromatografi GasDessi Hikma AnindyaNo ratings yet
- The Metabolism of O - (4 - B R O M O - 2, 5 - Dichlorophenyl) O-Methyl Phenylphosphonothioate (Leptophos) in White Mice and On Cotton PlantsDocument15 pagesThe Metabolism of O - (4 - B R O M O - 2, 5 - Dichlorophenyl) O-Methyl Phenylphosphonothioate (Leptophos) in White Mice and On Cotton PlantsSh1vaNo ratings yet
- The Phenolic Acids of Pzsz"achia F'eraDocument4 pagesThe Phenolic Acids of Pzsz"achia F'eraNanasaheb PatilNo ratings yet
- Guide to Trivial Names, Trade Names and Synonyms for Substances Used in Analytical Nomenclature: International Union of Pure and Applied Chemistry: Analytical Chemistry DivisionFrom EverandGuide to Trivial Names, Trade Names and Synonyms for Substances Used in Analytical Nomenclature: International Union of Pure and Applied Chemistry: Analytical Chemistry DivisionNo ratings yet
- 5 Domon 1984Document6 pages5 Domon 1984Enciu MariaNo ratings yet
- Synthesis of Some New Substituted 1,2,4-Triazole and 1,3,4-Thiadiazole and Study of Their Activities On Some Strains of BacteriaDocument8 pagesSynthesis of Some New Substituted 1,2,4-Triazole and 1,3,4-Thiadiazole and Study of Their Activities On Some Strains of BacteriaAmer KasidehNo ratings yet
- 3,4 AdciojnDocument4 pages3,4 AdciojnCalamidad Loco PeligroNo ratings yet
- Selected Medicinal PlantsDocument10 pagesSelected Medicinal PlantsNegar RzdNo ratings yet
- Art 06Document6 pagesArt 06Onkar SankajjiNo ratings yet
- Articulo MentolDocument4 pagesArticulo Mentoljuan_k5950No ratings yet
- Ring Opening of Cyclic Anhydrides: Synthesis of Achiral Half-Esters Using Lewis AcidsDocument4 pagesRing Opening of Cyclic Anhydrides: Synthesis of Achiral Half-Esters Using Lewis AcidsNaveed UR RehmanNo ratings yet
- 7819 PDFDocument8 pages7819 PDFirmaNo ratings yet
- Terpenes Importance General Structure and Biosynthesis PDFDocument9 pagesTerpenes Importance General Structure and Biosynthesis PDFAlejandra AvilaNo ratings yet
- Scrobipalpuloides Absoluta: Sex Pheromone of Tomato Pest (Lepidoptera: Gelechiidae)Document14 pagesScrobipalpuloides Absoluta: Sex Pheromone of Tomato Pest (Lepidoptera: Gelechiidae)Giovana Mamani HuayhuaNo ratings yet
- Isolation and Identification of Methyl Cinnamate From Syrian Ocimum Basilicum PDFDocument7 pagesIsolation and Identification of Methyl Cinnamate From Syrian Ocimum Basilicum PDFAnnamari ArdeleanuNo ratings yet
- Tsai 2012Document6 pagesTsai 2012kontiki500No ratings yet
- Aminouracil PresentationDocument30 pagesAminouracil Presentationabdo aboalkherNo ratings yet
- Solid-Phase Synthesis of Substituted 1,2,3-Triazoles: Florencio Zaragoza and Susanne Vejle PetersenDocument4 pagesSolid-Phase Synthesis of Substituted 1,2,3-Triazoles: Florencio Zaragoza and Susanne Vejle PetersenAndrés HidalgoNo ratings yet
- 7Shu-Geng Cao Valerie H.L. SNG Xiao-Hua Wu Keng-Yeow Sim B.H. - Novel Cytotoxic Polyprenylated Xanthonoids From GarcinDocument10 pages7Shu-Geng Cao Valerie H.L. SNG Xiao-Hua Wu Keng-Yeow Sim B.H. - Novel Cytotoxic Polyprenylated Xanthonoids From GarcinMunir AliNo ratings yet
- Development and Validation of Stability Indicating RP-HPLC Method For Simultaneous Estimation of Sofosbuvir and Ledipasvir in Tablet Dosage FormDocument4 pagesDevelopment and Validation of Stability Indicating RP-HPLC Method For Simultaneous Estimation of Sofosbuvir and Ledipasvir in Tablet Dosage FormBaru Chandrasekhar RaoNo ratings yet
- 399 1409 1 PBDocument10 pages399 1409 1 PBNadilla AlfitriNo ratings yet
- Progestins (Progestagens)Document15 pagesProgestins (Progestagens)Ismail MustafaNo ratings yet
- Steroidal 2Document15 pagesSteroidal 2Ismail MustafaNo ratings yet
- Gonadal Hormone & Inhibitor FixDocument41 pagesGonadal Hormone & Inhibitor FixDamara ArfianNo ratings yet
- Alcohol, Phenol and Ether 06-12-2020Document51 pagesAlcohol, Phenol and Ether 06-12-2020gaganshishodia2No ratings yet
- Cooper1979 PDFDocument3 pagesCooper1979 PDFJ Venkat RamanNo ratings yet
- Drugs of The Future 2002, 27 (2) 143-158Document16 pagesDrugs of The Future 2002, 27 (2) 143-158Rajesh TammanaNo ratings yet
- Week 1Document28 pagesWeek 1Putwi Widya CitradewiNo ratings yet
- Simple IUPAC NomenclatureDocument15 pagesSimple IUPAC Nomenclatureapi-3757218100% (6)
- Fitoterapia: Kohei Kamiya, Wakako Hamabe, Shogo Tokuyama, Toshiko SatakeDocument4 pagesFitoterapia: Kohei Kamiya, Wakako Hamabe, Shogo Tokuyama, Toshiko SatakeamirulNo ratings yet
- IntroductionDocument16 pagesIntroductionAkhtar RazaNo ratings yet
- Nooshin Ghaffari-Nia and Alireza Hassanabadi : Research Paper 291Document3 pagesNooshin Ghaffari-Nia and Alireza Hassanabadi : Research Paper 291Zina ZinaNo ratings yet
- LipidsDocument13 pagesLipidsMishyree AndatuanNo ratings yet
- Synthesis and Analgesic Evaluation of Some 5 - (B - (10-Phenothiazinyl) Ethyl) - 1 - (Acyl) - 1,2,3,4-TetrazolesDocument7 pagesSynthesis and Analgesic Evaluation of Some 5 - (B - (10-Phenothiazinyl) Ethyl) - 1 - (Acyl) - 1,2,3,4-TetrazolesWalid EbaiedNo ratings yet
- Ethyl 4 - (Triphenylphosphoranylidene) - Acetoacetate: O Tro Oh O Tro Co Et ODocument4 pagesEthyl 4 - (Triphenylphosphoranylidene) - Acetoacetate: O Tro Oh O Tro Co Et OPhạm Gia KhánhNo ratings yet
- Pnas00107 0188Document8 pagesPnas00107 0188Jamie HendersonNo ratings yet
- The Acetate Pathway: Fatty Acid and Polyketide: A. Eka Purnama Putri Fitokimia I 2017Document43 pagesThe Acetate Pathway: Fatty Acid and Polyketide: A. Eka Purnama Putri Fitokimia I 2017dhewiantyNo ratings yet
- BjvjfguDocument6 pagesBjvjfguClaudia Vivi AnantaNo ratings yet
- Tema 13 EngDocument18 pagesTema 13 EngChristian Artero AndreuNo ratings yet
- Isoquinoline Alkaloids From Michelia Fuscata: H. T. Li, C. L. Kao, C. R. Tsai, W. J. Li, and C. Y. ChenDocument4 pagesIsoquinoline Alkaloids From Michelia Fuscata: H. T. Li, C. L. Kao, C. R. Tsai, W. J. Li, and C. Y. Chenp6trqpc4qkNo ratings yet
- Iridoid and Phenylethanoid Glycosides From Euphrasia Pectinata (#142919) - 124342Document10 pagesIridoid and Phenylethanoid Glycosides From Euphrasia Pectinata (#142919) - 124342Hashemi Akhter100% (1)
- 3 Review of Literature (13 37) of Hemidesmus IndicusDocument26 pages3 Review of Literature (13 37) of Hemidesmus Indicusmithun_nm100% (1)
- Amphimedonoic Acid and Psammaplysene E Novel Brominated A - 2017 - TetrahedronDocument4 pagesAmphimedonoic Acid and Psammaplysene E Novel Brominated A - 2017 - TetrahedronC1Muhammad Iqbal FarozinNo ratings yet
- Total Synthesis of Ent - (+) - Cinanthrenol A: Original ArticleDocument7 pagesTotal Synthesis of Ent - (+) - Cinanthrenol A: Original ArticleQuốc NguyễnNo ratings yet
- Isoeugenol Ester Derivatives As Future Potential DrugDocument6 pagesIsoeugenol Ester Derivatives As Future Potential DrugIJRASETPublicationsNo ratings yet
- Molbank 2014 M819Document3 pagesMolbank 2014 M819Anouar AlamiNo ratings yet
- An Efficient Procedure For The Demethylation of Aryl-Methyl Ethers in Optically Pure Unusual Amino Acids PDFDocument4 pagesAn Efficient Procedure For The Demethylation of Aryl-Methyl Ethers in Optically Pure Unusual Amino Acids PDFFelipe MonteroNo ratings yet
- Chemrj 2016 01 02 06 10Document5 pagesChemrj 2016 01 02 06 10editor chemrjNo ratings yet
- Wjoc 2 1 1 PDFDocument8 pagesWjoc 2 1 1 PDFWalid Ebid ElgammalNo ratings yet
- Introduction to Steroid Chemistry: The Commonwealth and International Library: a Course in Organic ChemistryFrom EverandIntroduction to Steroid Chemistry: The Commonwealth and International Library: a Course in Organic ChemistryNo ratings yet
- Bio-Identical Hormones - New Beginnings-Half P VertDocument1 pageBio-Identical Hormones - New Beginnings-Half P VertsafinditNo ratings yet
- Sakala Step 2 CK GYN 2018 Color Handout 2 - PageDocument12 pagesSakala Step 2 CK GYN 2018 Color Handout 2 - PageJurian F. Kaunang100% (1)
- Lista de Precios Europa QualityDocument2 pagesLista de Precios Europa QualitylapiamaNo ratings yet
- Clomiphene and How Does It WorkhbudlDocument2 pagesClomiphene and How Does It Workhbudlspleenvelvet24No ratings yet
- HY Obgyn MehlmanmedicalDocument127 pagesHY Obgyn MehlmanmedicalalmostpetergriffinNo ratings yet
- High Estrogen in Men After Injectable Testosterone Therapy: The Low T ExperienceDocument6 pagesHigh Estrogen in Men After Injectable Testosterone Therapy: The Low T ExperienceMarko BukalNo ratings yet
- Recovery of Spermatogenesis Following Testosterone Replacement Therapy or Anabolic-Androgenic Steroid UseDocument8 pagesRecovery of Spermatogenesis Following Testosterone Replacement Therapy or Anabolic-Androgenic Steroid UseMariana CreciunNo ratings yet
- Pcol Lec (Midterms)Document10 pagesPcol Lec (Midterms)Daddy RulesNo ratings yet
- Female Reproductive System DrugsDocument5 pagesFemale Reproductive System DrugsSabrina LouiseNo ratings yet
- Estrogen DR DeanDocument8 pagesEstrogen DR DeanMochammad Halim NNo ratings yet
- Product Name CAS Number Prices in USD : Product Name Specification S Iu/mg US$/eachDocument2 pagesProduct Name CAS Number Prices in USD : Product Name Specification S Iu/mg US$/eachZhangNo ratings yet
- JLK Skenario 3 c.4 Kelompok 10Document16 pagesJLK Skenario 3 c.4 Kelompok 10NOVI UMAMI UMAMINo ratings yet
- William Lllewellyn's Anabolics, 11th Edition 2017 361 390Document30 pagesWilliam Lllewellyn's Anabolics, 11th Edition 2017 361 390Hamada MansourNo ratings yet
- Gonadal Hormones and InhibitorsDocument10 pagesGonadal Hormones and InhibitorsCarlos NiñoNo ratings yet
- Testosterone Replacement Therapy, A Recipe For Success - John Crisler, D.O.Document8 pagesTestosterone Replacement Therapy, A Recipe For Success - John Crisler, D.O.gstrohlNo ratings yet
- Steroid Half Life'sDocument6 pagesSteroid Half Life'sTomPark1No ratings yet
- Recent Advances in Contraception: Dr. Siddhartha Dutta Mamc, New DelhiDocument51 pagesRecent Advances in Contraception: Dr. Siddhartha Dutta Mamc, New DelhiJalajarani SelvaNo ratings yet
- Pharmacology - Repro (EDITED)Document25 pagesPharmacology - Repro (EDITED)AditiNo ratings yet
- Superovulasi PDFDocument68 pagesSuperovulasi PDFHayatul IlmiNo ratings yet
- Gonadal Hormones & Inhibitors Contraceptives: DR Dhoro Clinical PharmacologyDocument34 pagesGonadal Hormones & Inhibitors Contraceptives: DR Dhoro Clinical PharmacologykelvinNo ratings yet
- Combined Hormonal Contraceptives and Migraine - An Update On The EvidenceDocument8 pagesCombined Hormonal Contraceptives and Migraine - An Update On The EvidenceRoberto López MataNo ratings yet
- Arimidex (Anastrozole)Document11 pagesArimidex (Anastrozole)sami saleem MOTIVATIONNo ratings yet
- 1867EC Diasorin Liaison XL Add Values - IA3109-IA3112Document3 pages1867EC Diasorin Liaison XL Add Values - IA3109-IA3112concocdocNo ratings yet
- 20210824174819fechamento 1 Semestre Fixacao PMPFDocument94 pages20210824174819fechamento 1 Semestre Fixacao PMPFGabriel SilvaNo ratings yet
- Biology Grade 13 TMDocument7 pagesBiology Grade 13 TMJamunanantha PranavanNo ratings yet
- Female Precocious Puberty AlgorithmDocument1 pageFemale Precocious Puberty AlgorithmRICHI ADITYANo ratings yet
- Testosterone SuspensionDocument4 pagesTestosterone Suspensionmehrdad_44No ratings yet
- Hormonal Contraceptives in CanadaDocument3 pagesHormonal Contraceptives in CanadaNida Saghir AhmedNo ratings yet
- Gender Affirming Hormone Therapy GuidelinesDocument9 pagesGender Affirming Hormone Therapy GuidelinesAji VillanuevaNo ratings yet
- Pharmacology of Testosterone: Made By: Miangul Ali GoharDocument21 pagesPharmacology of Testosterone: Made By: Miangul Ali GoharAli GoharNo ratings yet























































































Download as pdf or txt
You might also like
- Lecture 25 - LipidsDocument58 pagesLecture 25 - Lipidsapi-19824406No ratings yet
- Synthesis and Aromatase Inhibition by Potential Metabolites of Exemestane (6-Methylenandrosta-L, 4-Diene-3,17-Dione)Document6 pagesSynthesis and Aromatase Inhibition by Potential Metabolites of Exemestane (6-Methylenandrosta-L, 4-Diene-3,17-Dione)Nimra Naveed ShaikhNo ratings yet
- (C) Androgens and Anabolic AgentsDocument24 pages(C) Androgens and Anabolic AgentsIsmail MustafaNo ratings yet
- Chapter 1 Definition and Classification of Lipids 1972Document51 pagesChapter 1 Definition and Classification of Lipids 1972aldofedeuriel152005No ratings yet
- (2022 11 10) 張訓碩-生藥學 (terpenoids)Document49 pages(2022 11 10) 張訓碩-生藥學 (terpenoids)tw910124No ratings yet
- Untul Pamantului ArticoleDocument2 pagesUntul Pamantului ArticoleRoxana FloreaNo ratings yet
- Organic ChemistryDocument44 pagesOrganic ChemistryKushashwa Ravi ShrimaliNo ratings yet
- ZZZ (0) Modified Trichothecenes (XXXX 325)Document24 pagesZZZ (0) Modified Trichothecenes (XXXX 325)amaroluisNo ratings yet
- Biosintesis of TerpenoidDocument19 pagesBiosintesis of TerpenoidIntanFrinaUtamiyantiNo ratings yet
- SurfactantsDocument11 pagesSurfactantstNo ratings yet
- Aplikasi Kromatografi GasDocument7 pagesAplikasi Kromatografi GasDessi Hikma AnindyaNo ratings yet
- The Metabolism of O - (4 - B R O M O - 2, 5 - Dichlorophenyl) O-Methyl Phenylphosphonothioate (Leptophos) in White Mice and On Cotton PlantsDocument15 pagesThe Metabolism of O - (4 - B R O M O - 2, 5 - Dichlorophenyl) O-Methyl Phenylphosphonothioate (Leptophos) in White Mice and On Cotton PlantsSh1vaNo ratings yet
- The Phenolic Acids of Pzsz"achia F'eraDocument4 pagesThe Phenolic Acids of Pzsz"achia F'eraNanasaheb PatilNo ratings yet
- Guide to Trivial Names, Trade Names and Synonyms for Substances Used in Analytical Nomenclature: International Union of Pure and Applied Chemistry: Analytical Chemistry DivisionFrom EverandGuide to Trivial Names, Trade Names and Synonyms for Substances Used in Analytical Nomenclature: International Union of Pure and Applied Chemistry: Analytical Chemistry DivisionNo ratings yet
- 5 Domon 1984Document6 pages5 Domon 1984Enciu MariaNo ratings yet
- Synthesis of Some New Substituted 1,2,4-Triazole and 1,3,4-Thiadiazole and Study of Their Activities On Some Strains of BacteriaDocument8 pagesSynthesis of Some New Substituted 1,2,4-Triazole and 1,3,4-Thiadiazole and Study of Their Activities On Some Strains of BacteriaAmer KasidehNo ratings yet
- 3,4 AdciojnDocument4 pages3,4 AdciojnCalamidad Loco PeligroNo ratings yet
- Selected Medicinal PlantsDocument10 pagesSelected Medicinal PlantsNegar RzdNo ratings yet
- Art 06Document6 pagesArt 06Onkar SankajjiNo ratings yet
- Articulo MentolDocument4 pagesArticulo Mentoljuan_k5950No ratings yet
- Ring Opening of Cyclic Anhydrides: Synthesis of Achiral Half-Esters Using Lewis AcidsDocument4 pagesRing Opening of Cyclic Anhydrides: Synthesis of Achiral Half-Esters Using Lewis AcidsNaveed UR RehmanNo ratings yet
- 7819 PDFDocument8 pages7819 PDFirmaNo ratings yet
- Terpenes Importance General Structure and Biosynthesis PDFDocument9 pagesTerpenes Importance General Structure and Biosynthesis PDFAlejandra AvilaNo ratings yet
- Scrobipalpuloides Absoluta: Sex Pheromone of Tomato Pest (Lepidoptera: Gelechiidae)Document14 pagesScrobipalpuloides Absoluta: Sex Pheromone of Tomato Pest (Lepidoptera: Gelechiidae)Giovana Mamani HuayhuaNo ratings yet
- Isolation and Identification of Methyl Cinnamate From Syrian Ocimum Basilicum PDFDocument7 pagesIsolation and Identification of Methyl Cinnamate From Syrian Ocimum Basilicum PDFAnnamari ArdeleanuNo ratings yet
- Tsai 2012Document6 pagesTsai 2012kontiki500No ratings yet
- Aminouracil PresentationDocument30 pagesAminouracil Presentationabdo aboalkherNo ratings yet
- Solid-Phase Synthesis of Substituted 1,2,3-Triazoles: Florencio Zaragoza and Susanne Vejle PetersenDocument4 pagesSolid-Phase Synthesis of Substituted 1,2,3-Triazoles: Florencio Zaragoza and Susanne Vejle PetersenAndrés HidalgoNo ratings yet
- 7Shu-Geng Cao Valerie H.L. SNG Xiao-Hua Wu Keng-Yeow Sim B.H. - Novel Cytotoxic Polyprenylated Xanthonoids From GarcinDocument10 pages7Shu-Geng Cao Valerie H.L. SNG Xiao-Hua Wu Keng-Yeow Sim B.H. - Novel Cytotoxic Polyprenylated Xanthonoids From GarcinMunir AliNo ratings yet
- Development and Validation of Stability Indicating RP-HPLC Method For Simultaneous Estimation of Sofosbuvir and Ledipasvir in Tablet Dosage FormDocument4 pagesDevelopment and Validation of Stability Indicating RP-HPLC Method For Simultaneous Estimation of Sofosbuvir and Ledipasvir in Tablet Dosage FormBaru Chandrasekhar RaoNo ratings yet
- 399 1409 1 PBDocument10 pages399 1409 1 PBNadilla AlfitriNo ratings yet
- Progestins (Progestagens)Document15 pagesProgestins (Progestagens)Ismail MustafaNo ratings yet
- Steroidal 2Document15 pagesSteroidal 2Ismail MustafaNo ratings yet
- Gonadal Hormone & Inhibitor FixDocument41 pagesGonadal Hormone & Inhibitor FixDamara ArfianNo ratings yet
- Alcohol, Phenol and Ether 06-12-2020Document51 pagesAlcohol, Phenol and Ether 06-12-2020gaganshishodia2No ratings yet
- Cooper1979 PDFDocument3 pagesCooper1979 PDFJ Venkat RamanNo ratings yet
- Drugs of The Future 2002, 27 (2) 143-158Document16 pagesDrugs of The Future 2002, 27 (2) 143-158Rajesh TammanaNo ratings yet
- Week 1Document28 pagesWeek 1Putwi Widya CitradewiNo ratings yet
- Simple IUPAC NomenclatureDocument15 pagesSimple IUPAC Nomenclatureapi-3757218100% (6)
- Fitoterapia: Kohei Kamiya, Wakako Hamabe, Shogo Tokuyama, Toshiko SatakeDocument4 pagesFitoterapia: Kohei Kamiya, Wakako Hamabe, Shogo Tokuyama, Toshiko SatakeamirulNo ratings yet
- IntroductionDocument16 pagesIntroductionAkhtar RazaNo ratings yet
- Nooshin Ghaffari-Nia and Alireza Hassanabadi : Research Paper 291Document3 pagesNooshin Ghaffari-Nia and Alireza Hassanabadi : Research Paper 291Zina ZinaNo ratings yet
- LipidsDocument13 pagesLipidsMishyree AndatuanNo ratings yet
- Synthesis and Analgesic Evaluation of Some 5 - (B - (10-Phenothiazinyl) Ethyl) - 1 - (Acyl) - 1,2,3,4-TetrazolesDocument7 pagesSynthesis and Analgesic Evaluation of Some 5 - (B - (10-Phenothiazinyl) Ethyl) - 1 - (Acyl) - 1,2,3,4-TetrazolesWalid EbaiedNo ratings yet
- Ethyl 4 - (Triphenylphosphoranylidene) - Acetoacetate: O Tro Oh O Tro Co Et ODocument4 pagesEthyl 4 - (Triphenylphosphoranylidene) - Acetoacetate: O Tro Oh O Tro Co Et OPhạm Gia KhánhNo ratings yet
- Pnas00107 0188Document8 pagesPnas00107 0188Jamie HendersonNo ratings yet
- The Acetate Pathway: Fatty Acid and Polyketide: A. Eka Purnama Putri Fitokimia I 2017Document43 pagesThe Acetate Pathway: Fatty Acid and Polyketide: A. Eka Purnama Putri Fitokimia I 2017dhewiantyNo ratings yet
- BjvjfguDocument6 pagesBjvjfguClaudia Vivi AnantaNo ratings yet
- Tema 13 EngDocument18 pagesTema 13 EngChristian Artero AndreuNo ratings yet
- Isoquinoline Alkaloids From Michelia Fuscata: H. T. Li, C. L. Kao, C. R. Tsai, W. J. Li, and C. Y. ChenDocument4 pagesIsoquinoline Alkaloids From Michelia Fuscata: H. T. Li, C. L. Kao, C. R. Tsai, W. J. Li, and C. Y. Chenp6trqpc4qkNo ratings yet
- Iridoid and Phenylethanoid Glycosides From Euphrasia Pectinata (#142919) - 124342Document10 pagesIridoid and Phenylethanoid Glycosides From Euphrasia Pectinata (#142919) - 124342Hashemi Akhter100% (1)
- 3 Review of Literature (13 37) of Hemidesmus IndicusDocument26 pages3 Review of Literature (13 37) of Hemidesmus Indicusmithun_nm100% (1)
- Amphimedonoic Acid and Psammaplysene E Novel Brominated A - 2017 - TetrahedronDocument4 pagesAmphimedonoic Acid and Psammaplysene E Novel Brominated A - 2017 - TetrahedronC1Muhammad Iqbal FarozinNo ratings yet
- Total Synthesis of Ent - (+) - Cinanthrenol A: Original ArticleDocument7 pagesTotal Synthesis of Ent - (+) - Cinanthrenol A: Original ArticleQuốc NguyễnNo ratings yet
- Isoeugenol Ester Derivatives As Future Potential DrugDocument6 pagesIsoeugenol Ester Derivatives As Future Potential DrugIJRASETPublicationsNo ratings yet
- Molbank 2014 M819Document3 pagesMolbank 2014 M819Anouar AlamiNo ratings yet
- An Efficient Procedure For The Demethylation of Aryl-Methyl Ethers in Optically Pure Unusual Amino Acids PDFDocument4 pagesAn Efficient Procedure For The Demethylation of Aryl-Methyl Ethers in Optically Pure Unusual Amino Acids PDFFelipe MonteroNo ratings yet
- Chemrj 2016 01 02 06 10Document5 pagesChemrj 2016 01 02 06 10editor chemrjNo ratings yet
- Wjoc 2 1 1 PDFDocument8 pagesWjoc 2 1 1 PDFWalid Ebid ElgammalNo ratings yet
- Introduction to Steroid Chemistry: The Commonwealth and International Library: a Course in Organic ChemistryFrom EverandIntroduction to Steroid Chemistry: The Commonwealth and International Library: a Course in Organic ChemistryNo ratings yet
- Bio-Identical Hormones - New Beginnings-Half P VertDocument1 pageBio-Identical Hormones - New Beginnings-Half P VertsafinditNo ratings yet
- Sakala Step 2 CK GYN 2018 Color Handout 2 - PageDocument12 pagesSakala Step 2 CK GYN 2018 Color Handout 2 - PageJurian F. Kaunang100% (1)
- Lista de Precios Europa QualityDocument2 pagesLista de Precios Europa QualitylapiamaNo ratings yet
- Clomiphene and How Does It WorkhbudlDocument2 pagesClomiphene and How Does It Workhbudlspleenvelvet24No ratings yet
- HY Obgyn MehlmanmedicalDocument127 pagesHY Obgyn MehlmanmedicalalmostpetergriffinNo ratings yet
- High Estrogen in Men After Injectable Testosterone Therapy: The Low T ExperienceDocument6 pagesHigh Estrogen in Men After Injectable Testosterone Therapy: The Low T ExperienceMarko BukalNo ratings yet
- Recovery of Spermatogenesis Following Testosterone Replacement Therapy or Anabolic-Androgenic Steroid UseDocument8 pagesRecovery of Spermatogenesis Following Testosterone Replacement Therapy or Anabolic-Androgenic Steroid UseMariana CreciunNo ratings yet
- Pcol Lec (Midterms)Document10 pagesPcol Lec (Midterms)Daddy RulesNo ratings yet
- Female Reproductive System DrugsDocument5 pagesFemale Reproductive System DrugsSabrina LouiseNo ratings yet
- Estrogen DR DeanDocument8 pagesEstrogen DR DeanMochammad Halim NNo ratings yet
- Product Name CAS Number Prices in USD : Product Name Specification S Iu/mg US$/eachDocument2 pagesProduct Name CAS Number Prices in USD : Product Name Specification S Iu/mg US$/eachZhangNo ratings yet
- JLK Skenario 3 c.4 Kelompok 10Document16 pagesJLK Skenario 3 c.4 Kelompok 10NOVI UMAMI UMAMINo ratings yet
- William Lllewellyn's Anabolics, 11th Edition 2017 361 390Document30 pagesWilliam Lllewellyn's Anabolics, 11th Edition 2017 361 390Hamada MansourNo ratings yet
- Gonadal Hormones and InhibitorsDocument10 pagesGonadal Hormones and InhibitorsCarlos NiñoNo ratings yet
- Testosterone Replacement Therapy, A Recipe For Success - John Crisler, D.O.Document8 pagesTestosterone Replacement Therapy, A Recipe For Success - John Crisler, D.O.gstrohlNo ratings yet
- Steroid Half Life'sDocument6 pagesSteroid Half Life'sTomPark1No ratings yet
- Recent Advances in Contraception: Dr. Siddhartha Dutta Mamc, New DelhiDocument51 pagesRecent Advances in Contraception: Dr. Siddhartha Dutta Mamc, New DelhiJalajarani SelvaNo ratings yet
- Pharmacology - Repro (EDITED)Document25 pagesPharmacology - Repro (EDITED)AditiNo ratings yet
- Superovulasi PDFDocument68 pagesSuperovulasi PDFHayatul IlmiNo ratings yet
- Gonadal Hormones & Inhibitors Contraceptives: DR Dhoro Clinical PharmacologyDocument34 pagesGonadal Hormones & Inhibitors Contraceptives: DR Dhoro Clinical PharmacologykelvinNo ratings yet
- Combined Hormonal Contraceptives and Migraine - An Update On The EvidenceDocument8 pagesCombined Hormonal Contraceptives and Migraine - An Update On The EvidenceRoberto López MataNo ratings yet
- Arimidex (Anastrozole)Document11 pagesArimidex (Anastrozole)sami saleem MOTIVATIONNo ratings yet
- 1867EC Diasorin Liaison XL Add Values - IA3109-IA3112Document3 pages1867EC Diasorin Liaison XL Add Values - IA3109-IA3112concocdocNo ratings yet
- 20210824174819fechamento 1 Semestre Fixacao PMPFDocument94 pages20210824174819fechamento 1 Semestre Fixacao PMPFGabriel SilvaNo ratings yet
- Biology Grade 13 TMDocument7 pagesBiology Grade 13 TMJamunanantha PranavanNo ratings yet
- Female Precocious Puberty AlgorithmDocument1 pageFemale Precocious Puberty AlgorithmRICHI ADITYANo ratings yet
- Testosterone SuspensionDocument4 pagesTestosterone Suspensionmehrdad_44No ratings yet
- Hormonal Contraceptives in CanadaDocument3 pagesHormonal Contraceptives in CanadaNida Saghir AhmedNo ratings yet
- Gender Affirming Hormone Therapy GuidelinesDocument9 pagesGender Affirming Hormone Therapy GuidelinesAji VillanuevaNo ratings yet
- Pharmacology of Testosterone: Made By: Miangul Ali GoharDocument21 pagesPharmacology of Testosterone: Made By: Miangul Ali GoharAli GoharNo ratings yet