Download as pdf or txt
You might also like
- NBME FORM 26-AnswersDocument52 pagesNBME FORM 26-Answersmed student50% (8)
- Angelito L. Ramos Jr. RN Clinical InstructorDocument68 pagesAngelito L. Ramos Jr. RN Clinical Instructorraymondblade18100% (17)
- Pleural EffusionDocument49 pagesPleural EffusionLyra Lorca86% (7)
- Su ND: Ly (/ /min, /minDocument3 pagesSu ND: Ly (/ /min, /minAlex ChenNo ratings yet
- LD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomDocument5 pagesLD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomAlex ChenNo ratings yet
- Su ND: Item: ADocument8 pagesSu ND: Item: AHawkElseNo ratings yet
- Item:: 0. LD: 2777 Prevoous Next Lab Values Notes Calculator Reverse Color Text ZoomDocument10 pagesItem:: 0. LD: 2777 Prevoous Next Lab Values Notes Calculator Reverse Color Text ZoomHawkElseNo ratings yet
- Su ND: Eft e E. FDocument3 pagesSu ND: Eft e E. FAlex ChenNo ratings yet
- Ono Oano: / /min, /min /DL /MM'Document22 pagesOno Oano: / /min, /min /DL /MM'ايات عبدالرحمنNo ratings yet
- 23 Sur Deviated Nasal SeptumDocument3 pages23 Sur Deviated Nasal SeptumSardar jiNo ratings yet
- Su ND: o o o o oDocument3 pagesSu ND: o o o o oAlex ChenNo ratings yet
- Su ND: ItemDocument3 pagesSu ND: ItemHawkElseNo ratings yet
- UW 2024 - OphthalmologyDocument204 pagesUW 2024 - Ophthalmology부산No ratings yet
- 142 Ped Cystic FibrosisDocument9 pages142 Ped Cystic FibrosisritaNo ratings yet
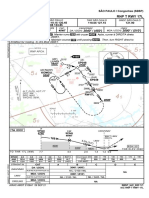
- SBSP Rnp-T-Rwy-17l Iac 20231130Document1 pageSBSP Rnp-T-Rwy-17l Iac 20231130carine mirandaNo ratings yet
- 1 Q PDFDocument44 pages1 Q PDFMysheb SSNo ratings yet
- 030 Med CytomegalovirusDocument5 pages030 Med CytomegalovirusArun Kumar ChaudharyNo ratings yet
- SBSP Rnp-T-Rwy-17l Iac 20210909Document1 pageSBSP Rnp-T-Rwy-17l Iac 20210909Patrick ReisNo ratings yet
- ATS EngDocument1 pageATS EngOctavianus LinNo ratings yet
- 143 Ped DehydrationDocument4 pages143 Ped DehydrationritaNo ratings yet
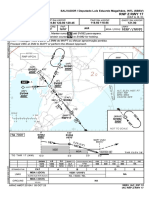
- SBSV Rnp-Z-Rwy-17 Iac 20231005Document1 pageSBSV Rnp-Z-Rwy-17 Iac 20231005Ulisses MalheirosNo ratings yet
- Digital Capacitance Meter: Electronic Instrumentati NDocument8 pagesDigital Capacitance Meter: Electronic Instrumentati NRama ChandraNo ratings yet
- SBGW Rnp-A-Rwy-20 Iac 20221229Document2 pagesSBGW Rnp-A-Rwy-20 Iac 20221229filozoeiraNo ratings yet
- 0067 27Document5 pages0067 27Alex ChenNo ratings yet
- 144 Ped Foreign Body IngestionDocument3 pages144 Ped Foreign Body IngestionritaNo ratings yet
- 103R PanelDocument23 pages103R Panelprobal nandyNo ratings yet
- SBGW Rwy-02-20 Vac 20220324Document2 pagesSBGW Rwy-02-20 Vac 20220324Samuel ÍcaroNo ratings yet
- First FloorDocument1 pageFirst FloorQawi Pg SofryNo ratings yet
- First FloorDocument1 pageFirst FloorQawi Pg SofryNo ratings yet
- Final Melendes Etapa 3Document4 pagesFinal Melendes Etapa 3fabian campillayNo ratings yet
- A25A WiringDocument14 pagesA25A Wiringprogas.ukraineNo ratings yet
- R SignDocument35 pagesR SignRichard Andrianjaka LuckyNo ratings yet
- Amalgamation Including AS 14 13 - Class NotesDocument11 pagesAmalgamation Including AS 14 13 - Class NotesMainak AdhikaryNo ratings yet
- Neo Mob 601 001Document1 pageNeo Mob 601 001Edwin PrinceNo ratings yet
- OpthalmologyDocument45 pagesOpthalmologyWill HNo ratings yet
- Emt 2Document25 pagesEmt 2Raghvendra SinghNo ratings yet
- A-103 - (R0) - First Floor Plan - 28.03.2020Document1 pageA-103 - (R0) - First Floor Plan - 28.03.2020Deepanshu GargNo ratings yet
- 4 300 Kgs Udl 300 Kgs Udl: Available Area 36000 7060 7060 7060 7060Document1 page4 300 Kgs Udl 300 Kgs Udl: Available Area 36000 7060 7060 7060 7060Paturu VijayNo ratings yet
- Aermec Dual ChillersDocument80 pagesAermec Dual ChillerscarloNo ratings yet
- Nvent Eriflex Flexibar Advanced - From 125 A To 2800 A As Per IecDocument1 pageNvent Eriflex Flexibar Advanced - From 125 A To 2800 A As Per Iecnajib elhakymNo ratings yet
- The Dynamics of A Simple Servomechanism For Angular Position ControlDocument2 pagesThe Dynamics of A Simple Servomechanism For Angular Position ControlHaroune DjemaiouneNo ratings yet
- Pages From TrussDocument1 pagePages From TrussDương TrầnNo ratings yet
- FireNet Series Battery Calculator V3.057Document7 pagesFireNet Series Battery Calculator V3.057mujahid_islam85No ratings yet
- Chapter-3: MethodologyDocument16 pagesChapter-3: Methodology임광식No ratings yet
- Ms Lecture 4 PDFDocument11 pagesMs Lecture 4 PDFAkash GolwalkarNo ratings yet
- 6ORZO/::Rugvdqg0Xvlfe/ - 2+1/ (1121 & &PDM) & &PDMDocument4 pages6ORZO/::Rugvdqg0Xvlfe/ - 2+1/ (1121 & &PDM) & &PDMandreaavenaNo ratings yet
- 2022-09-13 Cajas Electricidad Domoticas X Wifi - AMAZONDocument4 pages2022-09-13 Cajas Electricidad Domoticas X Wifi - AMAZONmr. guyNo ratings yet
- Logika PCBDocument2 pagesLogika PCBbobannesicNo ratings yet
- 15- for print Karlancer محافظDocument1 page15- for print Karlancer محافظmani saghiNo ratings yet
- PRQP N - A (C.TL - I: (: - Ko"'Ponen Mol)Document11 pagesPRQP N - A (C.TL - I: (: - Ko"'Ponen Mol)zainulNo ratings yet
- Velino Classic EsquemaDocument24 pagesVelino Classic EsquemaPedro Cristian Lagos CarvachoNo ratings yet
- Jensen Transformers 1977Document114 pagesJensen Transformers 1977Hugues ValotNo ratings yet
- 205BRS Overview V0 1 DraftDocument1 page205BRS Overview V0 1 DraftNicolau LuanaNo ratings yet
- SBGR - Iac Ils P Cat II - III Rwy 09r - Iac - 20211202Document1 pageSBGR - Iac Ils P Cat II - III Rwy 09r - Iac - 20211202thiagodesouzacostaNo ratings yet
- Page 7Document1 pagePage 7api-3839892No ratings yet
- EC Legend Final CoachingDocument61 pagesEC Legend Final CoachingVirna Grace MonteroNo ratings yet
- ERC160160-2 InterfacingDocument1 pageERC160160-2 InterfacingWagner SilvaNo ratings yet
- CagliariDocument12 pagesCagliarimarinaiomen0909No ratings yet
- BA4022710-01 - MTeC EPT303 WiringDiagrammDocument1 pageBA4022710-01 - MTeC EPT303 WiringDiagrammCristina AntohiNo ratings yet
- Excavation Process 1 (CST-04)Document1 pageExcavation Process 1 (CST-04)LE ANH TRANNo ratings yet
- CCB AW and AD Monitoring 04072023Document1 pageCCB AW and AD Monitoring 04072023dayat marzukiNo ratings yet
- Synoptique Note de Calcul Caneco HT Boucle HtaDocument1 pageSynoptique Note de Calcul Caneco HT Boucle HtabadriNo ratings yet
- ECG For OsceDocument69 pagesECG For OsceElenaCNo ratings yet
- Serous Membrane: Jump To Navigation Jump To SearchDocument12 pagesSerous Membrane: Jump To Navigation Jump To SearchsakuraleeshaoranNo ratings yet
- Pregnancy Induced HypertensionDocument4 pagesPregnancy Induced HypertensioncfgrtwifhNo ratings yet
- Diapo CardioDocument55 pagesDiapo Cardioapi-667225436No ratings yet
- J American Geriatrics Society - 2023 - American Geriatrics Society 2023 Updated AGS Beers Criteria For PotentiallyDocument30 pagesJ American Geriatrics Society - 2023 - American Geriatrics Society 2023 Updated AGS Beers Criteria For PotentiallyIstiNo ratings yet
- Compre PE and ROSDocument7 pagesCompre PE and ROSBatch V Med 2 SY 21-22No ratings yet
- APEA QBank AANP Review Latest 2022Document22 pagesAPEA QBank AANP Review Latest 2022Oleg KnazNo ratings yet
- Vivid T8Document4 pagesVivid T8muhammed kaletNo ratings yet
- LAPORAN BULANAN PRAKTEK MANDIRI Dr. YUDI SUSANTO BULAN OKT 2022Document4 pagesLAPORAN BULANAN PRAKTEK MANDIRI Dr. YUDI SUSANTO BULAN OKT 2022Syafari SkmNo ratings yet
- Obstetric ShockDocument14 pagesObstetric ShockANUM NOORINo ratings yet
- Dosage Forms and StrengthsDocument10 pagesDosage Forms and StrengthsSinta Chaira MaulanisaNo ratings yet
- Pasmedicine 2019Document183 pagesPasmedicine 2019Ibrahim FoondunNo ratings yet
- Nursing ManagementDocument10 pagesNursing ManagementMohamed Abd El MonemNo ratings yet
- Glucagon-Like Peptide 1 수용체작용제 최신지견Document8 pagesGlucagon-Like Peptide 1 수용체작용제 최신지견이호원No ratings yet
- Skin Autofluorescence-Indicated Advanced Glycation End Products As Predictors of Cardiovascular and All Cause Mortality in High Risk Subjects A Systematic Review and Meta AnalysisDocument19 pagesSkin Autofluorescence-Indicated Advanced Glycation End Products As Predictors of Cardiovascular and All Cause Mortality in High Risk Subjects A Systematic Review and Meta Analysisli_87No ratings yet
- Actilyse®: AlteplaseDocument13 pagesActilyse®: AlteplaseinassNo ratings yet
- BP, Heart Rate of DogDocument24 pagesBP, Heart Rate of DogVidhiNo ratings yet
- JOUR294 Lesson Plan 7Document4 pagesJOUR294 Lesson Plan 7dimitrius hanumansinghNo ratings yet
- Laporan Peringkat Diagnosa Harian 07012020 101256Document1 pageLaporan Peringkat Diagnosa Harian 07012020 101256I Putu Surada SuradaNo ratings yet
- HascvdDocument92 pagesHascvdbatangas_ynad_29900% (1)
- Nervous System ReviewerDocument26 pagesNervous System ReviewerAllea Marie SabacNo ratings yet
- SlideKit STEMI TreatmentDocument71 pagesSlideKit STEMI TreatmentandreaNo ratings yet
- The 12 Lead Ecg HandoutDocument5 pagesThe 12 Lead Ecg HandoutReza MajidiNo ratings yet
- Paper 1 Longer Answer QuestionsDocument26 pagesPaper 1 Longer Answer Questionsaadilmiah2019No ratings yet
- Genetice Disorders: Genetic Disorder Is A Disease or Disorder Caused by Damage or Change and Mutation On Individual's DNADocument46 pagesGenetice Disorders: Genetic Disorder Is A Disease or Disorder Caused by Damage or Change and Mutation On Individual's DNAAna Subol AñonuevoNo ratings yet
- CCrISP 7 Shock and HaemorrhageDocument27 pagesCCrISP 7 Shock and HaemorrhageDrSayk YousufNo ratings yet
- Epistaxis Diagnosis and Treatment Update A Review PDFDocument4 pagesEpistaxis Diagnosis and Treatment Update A Review PDFekoNo ratings yet