Download as pdf or txt
You might also like
- Seller Code of Conduct AppealDocument4 pagesSeller Code of Conduct AppealMAHER FAHADNo ratings yet
- ASTA Membership Directory 2022Document18 pagesASTA Membership Directory 2022Vasanthi Muthayan100% (1)
- Delta Planer ManualDocument44 pagesDelta Planer ManualstiellNo ratings yet
- Colorado Insurance HandbookDocument36 pagesColorado Insurance Handbookbomama01No ratings yet
- Meta-Analysis of Randomized Controlled Trials of The Efficacy of Propolis Mouthwash in Cancer Therapy-Induced Oral MucositisDocument9 pagesMeta-Analysis of Randomized Controlled Trials of The Efficacy of Propolis Mouthwash in Cancer Therapy-Induced Oral MucositisandikaisnaeniNo ratings yet
- Original Article: AbstractDocument3 pagesOriginal Article: Abstractyohanes22No ratings yet
- ZZZZZZZZZZZZZZDocument8 pagesZZZZZZZZZZZZZZchloramphenicolNo ratings yet
- Charalambous2018 OkDocument9 pagesCharalambous2018 Okdayana nopridaNo ratings yet
- The Effect of Topical Chamomile in The Prevention of Chemotherapy-Induced Oral Mucositis: A Randomized Clinical TrialDocument30 pagesThe Effect of Topical Chamomile in The Prevention of Chemotherapy-Induced Oral Mucositis: A Randomized Clinical Trialemmanuelle leal capelliniNo ratings yet
- 172tonutraj WoundDocument4 pages172tonutraj Woundfa_ndriNo ratings yet
- 39 UyifDocument12 pages39 UyifGeorgia.annaNo ratings yet
- Rro 02 796 PDFDocument4 pagesRro 02 796 PDFalejandromfunes1749No ratings yet
- Effect of Thai Fruit Mesocarp Extracts On Growth of Helicobacter Pylori and Their Antiadhesion Activities To Hep2 CellsDocument6 pagesEffect of Thai Fruit Mesocarp Extracts On Growth of Helicobacter Pylori and Their Antiadhesion Activities To Hep2 CellsDediSatriaNo ratings yet
- Single-Dose Azithromycin Versus Benzathine Benzylpenicillin For Treatment of Yaws in Children in Papua New Guinea: An Open-Label, Non-Inferiority, Randomised TrialDocument7 pagesSingle-Dose Azithromycin Versus Benzathine Benzylpenicillin For Treatment of Yaws in Children in Papua New Guinea: An Open-Label, Non-Inferiority, Randomised TrialOlivia Halim KumalaNo ratings yet
- Effect of Oral Cryotherapy in Preventing Chemotherapy Induced Oral Stomatitis Among Childhood Acute Lymphoblastic LeukemiaDocument10 pagesEffect of Oral Cryotherapy in Preventing Chemotherapy Induced Oral Stomatitis Among Childhood Acute Lymphoblastic LeukemiaIjahss JournalNo ratings yet
- DS 8971746Document10 pagesDS 8971746Waode Rifa AdhianiNo ratings yet
- Current Treatment of Oral Candidiasis: A Literature ReviewDocument12 pagesCurrent Treatment of Oral Candidiasis: A Literature ReviewgilangNo ratings yet
- Pharmaceutics 12 00446Document24 pagesPharmaceutics 12 00446Nikita jainNo ratings yet
- Curra 2021Document9 pagesCurra 2021Chouaib MeraoumiaNo ratings yet
- Feasibility of Eliminating Ocular Chlamydia Trachomatis With Repeat Mass Antibiotic TreatmentsDocument5 pagesFeasibility of Eliminating Ocular Chlamydia Trachomatis With Repeat Mass Antibiotic TreatmentsAmelia RoziantyNo ratings yet
- Jurnal 2Document6 pagesJurnal 2Devie AyuNo ratings yet
- Oral Ivermectin Versus Malathion Lotion For Difficult-to-Treat Head LiceDocument10 pagesOral Ivermectin Versus Malathion Lotion For Difficult-to-Treat Head LiceM Iqbal RahadyantoNo ratings yet
- 3920 B 20 XavierDocument7 pages3920 B 20 Xavierكرار حيدر وهيبNo ratings yet
- PharmacovigilanceinClinicalDentistry SCDocument6 pagesPharmacovigilanceinClinicalDentistry SCIoana AntonesiNo ratings yet
- Salihu, Hajarat Oyiza: Efficacy and Hypertoxicity of Guava Mistletoe On CancerDocument11 pagesSalihu, Hajarat Oyiza: Efficacy and Hypertoxicity of Guava Mistletoe On CancerPeter DindahNo ratings yet
- Microbiology of Chronic Suppurative Otitis Media in A Tertiary Care Setup of Uttarakhand State, IndiaDocument10 pagesMicrobiology of Chronic Suppurative Otitis Media in A Tertiary Care Setup of Uttarakhand State, IndiaMas YettyNo ratings yet
- Treatment of Scabies: Comparison of Permethrin 5% Versus IvermectinDocument4 pagesTreatment of Scabies: Comparison of Permethrin 5% Versus IvermectinWilliam WijayaNo ratings yet
- G Chemo-NoviDocument9 pagesG Chemo-Noviamila.zukanovicNo ratings yet
- Jurnal Kulit 1 (Aloe-Vera)Document7 pagesJurnal Kulit 1 (Aloe-Vera)Alifan HaqiNo ratings yet
- Microbial Contamination of Nonsterile Pharmaceuticals in Public Hospital SettingsDocument8 pagesMicrobial Contamination of Nonsterile Pharmaceuticals in Public Hospital SettingsOghenekome Ereromebe AkpogumeNo ratings yet
- Antimicrobial Effect of Honey Produced by On Some Common Human PathogensDocument6 pagesAntimicrobial Effect of Honey Produced by On Some Common Human Pathogensreal_septiady_madrid3532No ratings yet
- 2023.badr - AOVE MucosisitDocument6 pages2023.badr - AOVE Mucosisitv8w7g2xyjcNo ratings yet
- The Inhibitory Effect of Mesembryanthemum Edule Bolus Essential Oil On Some Pathogenic Fungal IsolatesDocument7 pagesThe Inhibitory Effect of Mesembryanthemum Edule Bolus Essential Oil On Some Pathogenic Fungal IsolatesDaniel MarţuneacNo ratings yet
- Antibacteril and Antifungal Activities of Punica Granatum Peel Extracts Against Oral PathogensDocument6 pagesAntibacteril and Antifungal Activities of Punica Granatum Peel Extracts Against Oral Pathogensmichael DariasNo ratings yet
- The Effect of Cryotherapy On The Prevention of Oral Mucositis and On TheDocument7 pagesThe Effect of Cryotherapy On The Prevention of Oral Mucositis and On ThePaola GilNo ratings yet
- 1 s2.0 S187638201930383X MainDocument8 pages1 s2.0 S187638201930383X MainArthur RamadhaniNo ratings yet
- MagicMouthwash For OralMucositis Sol Stanford PDFDocument2 pagesMagicMouthwash For OralMucositis Sol Stanford PDFManuel ArenasNo ratings yet
- Biopharmaceutical Studies On Gastroretentive Oral Dosage Forms For Eradication of Helicobacter PyloriDocument14 pagesBiopharmaceutical Studies On Gastroretentive Oral Dosage Forms For Eradication of Helicobacter PyloriFarhan IqbalNo ratings yet
- Use of Therapeutic Laser For Prevention and Treatment of Oral MucositisDocument6 pagesUse of Therapeutic Laser For Prevention and Treatment of Oral Mucositishendra ardiantoNo ratings yet
- Basat. DHA-PQP, AL, MalariaDocument10 pagesBasat. DHA-PQP, AL, Malariabaitur_rohmah8372No ratings yet
- Emollient Enhancement of The Skin Barrier From Birth Offers Effective Atopic Dermatitis PreventionDocument6 pagesEmollient Enhancement of The Skin Barrier From Birth Offers Effective Atopic Dermatitis PreventionAditya Praja'schNo ratings yet
- Wabe NT 2011Document7 pagesWabe NT 2011Agus PrimaNo ratings yet
- Efficacy and Safety of Oral Cefixime For The Short-Term Treatment of Typhoid Fever in A Group of Egyptian ChildrenDocument14 pagesEfficacy and Safety of Oral Cefixime For The Short-Term Treatment of Typhoid Fever in A Group of Egyptian ChildrenTafiqul Islam ShohagNo ratings yet
- Efficacy and Safety of Topical Versus Systemic Isotretinoin For Acne Vulgaris Treatment A Systematic ReviewDocument12 pagesEfficacy and Safety of Topical Versus Systemic Isotretinoin For Acne Vulgaris Treatment A Systematic ReviewAthenaeum Scientific PublishersNo ratings yet
- Sample of Journal & Critique PresenationDocument42 pagesSample of Journal & Critique PresenationMonika shankarNo ratings yet
- Health20110100011 52045487Document7 pagesHealth20110100011 52045487Vjai RajuNo ratings yet
- Aust J Dermatology - 2023 - AcneDocument4 pagesAust J Dermatology - 2023 - Acnesara3elena3manolacheNo ratings yet
- Bahan JurnalDocument6 pagesBahan JurnalDwi ApriyantiNo ratings yet
- Periodontology 2000 - 2023 - Herrera - Europe S Contribution To The Evaluation of The Use of Systemic Antimicrobials in TheDocument28 pagesPeriodontology 2000 - 2023 - Herrera - Europe S Contribution To The Evaluation of The Use of Systemic Antimicrobials in TheEngku Ahmad MuzhaffarNo ratings yet
- A Study On The Drug Prescribing Pattern in Acute, Recurrent and Chronic Pharyngitis at A Tertiary Care HospitalDocument5 pagesA Study On The Drug Prescribing Pattern in Acute, Recurrent and Chronic Pharyngitis at A Tertiary Care HospitalFriskyShandy BadiNo ratings yet
- Hasanbeigi Et AlDocument4 pagesHasanbeigi Et AlAhmad BukhariNo ratings yet
- Archana DeviDocument5 pagesArchana DeviTsubakiHariuNo ratings yet
- Prescripción Antibiótica EndodonciaDocument7 pagesPrescripción Antibiótica EndodonciaPaola AndreaNo ratings yet
- BP ChemoDocument20 pagesBP ChemoLeticia Quiñonez VivasNo ratings yet
- Developments in Therapy and Diagnosis of Yaws and Future ProspectsDocument8 pagesDevelopments in Therapy and Diagnosis of Yaws and Future ProspectsOlivia Halim KumalaNo ratings yet
- Oral Care in Ventilation MechanicDocument8 pagesOral Care in Ventilation MechanicRusida LiyaniNo ratings yet
- Efficacy and Safety of Plant-Based Therapy On Recurrent Aphthous Stomatitis and Oral Mucositis in The Past Decade: A Systematic ReviewDocument10 pagesEfficacy and Safety of Plant-Based Therapy On Recurrent Aphthous Stomatitis and Oral Mucositis in The Past Decade: A Systematic ReviewRohaniNo ratings yet
- Public Health 309Document5 pagesPublic Health 309Blue TechNo ratings yet
- New England Journal Medicine: The ofDocument7 pagesNew England Journal Medicine: The ofNanny HerwantoNo ratings yet
- Safety, Analgesic, and Anti-Inflammatory Effects of Aqueous and Methanolic Leaf Extracts of Hypericum Revolutum Subsp. KenienseDocument11 pagesSafety, Analgesic, and Anti-Inflammatory Effects of Aqueous and Methanolic Leaf Extracts of Hypericum Revolutum Subsp. KenienseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Development and Validation of The Oral Mucositis Risk Assessment Scale in Hematology PatientsDocument6 pagesDevelopment and Validation of The Oral Mucositis Risk Assessment Scale in Hematology PatientsPaola GilNo ratings yet
- JIAP July 2018 - Effectiveness of Pomegranate Mouthrinse in Reducing Bacterial Plaque, Gingival Inflammation and Total Salivary Proteins Over A Period of 90 Days - A Double-Blind Randomized TrialDocument5 pagesJIAP July 2018 - Effectiveness of Pomegranate Mouthrinse in Reducing Bacterial Plaque, Gingival Inflammation and Total Salivary Proteins Over A Period of 90 Days - A Double-Blind Randomized TrialVenosha RajenNo ratings yet
- Chaidemenos Et Al-2011-Journal of The European Academy of Dermatology and VenereologyDocument5 pagesChaidemenos Et Al-2011-Journal of The European Academy of Dermatology and VenereologyMario CastroNo ratings yet
- Plant Disease Management Strategies for Sustainable Agriculture through Traditional and Modern ApproachesFrom EverandPlant Disease Management Strategies for Sustainable Agriculture through Traditional and Modern ApproachesImran Ul HaqNo ratings yet
- Omega 3 e ELADocument7 pagesOmega 3 e ELAcarolineNo ratings yet
- w3 e CaquexiaDocument8 pagesw3 e CaquexiacarolineNo ratings yet
- Caffeic Acid Phenethyl Ester and Ethanol Extract of PropolisDocument21 pagesCaffeic Acid Phenethyl Ester and Ethanol Extract of PropoliscarolineNo ratings yet
- Antineoplastic Effects of Chlorella Pyrenoidosa in The BreastDocument10 pagesAntineoplastic Effects of Chlorella Pyrenoidosa in The BreastcarolineNo ratings yet
- Testa 2006Document49 pagesTesta 2006carolineNo ratings yet
- Dietary Intake of Cancer Patients On RadiotherapyDocument4 pagesDietary Intake of Cancer Patients On RadiotherapycarolineNo ratings yet
- AR MulheresDocument8 pagesAR MulherescarolineNo ratings yet
- Drexel SL 30-40-50 AC MM F-626-0419Document140 pagesDrexel SL 30-40-50 AC MM F-626-0419Abel GonzalezNo ratings yet
- Comparacion Entre G.usbamp y Open BciDocument10 pagesComparacion Entre G.usbamp y Open BciFISORGNo ratings yet
- Eat Right Tip #1: Remove and Reduce The BadDocument4 pagesEat Right Tip #1: Remove and Reduce The BadPJK1-0619 Nurul Asyraf Bin Nurul AklaNo ratings yet
- The Prohibition of Alcohol in IslamDocument9 pagesThe Prohibition of Alcohol in IslamAsim Raheel KhanNo ratings yet
- Tugas English Afwa Jurnal 1910811011 GanjilDocument4 pagesTugas English Afwa Jurnal 1910811011 Ganjilsakna afwaNo ratings yet
- NIPON STEEL Solution For Offshore Oil and GasDocument21 pagesNIPON STEEL Solution For Offshore Oil and GasCharwin XiaoNo ratings yet
- Warehouse & Storage Techniques - Lecture 3Document29 pagesWarehouse & Storage Techniques - Lecture 3Muhammad AhsanNo ratings yet
- Chemistry PracticalsDocument15 pagesChemistry PracticalsKashish ChoudharyNo ratings yet
- Phase I II MetabolismDocument21 pagesPhase I II MetabolismIlva Kristiāna LangrateNo ratings yet
- Elems 05Document101 pagesElems 05Reynald de VeraNo ratings yet
- ToxicologyDocument197 pagesToxicologyRichelle Dianne Ramos-Giang100% (6)
- (Download PDF) The Monstrous Feminine in Contemporary Japanese Popular Culture Raechel Dumas Online Ebook All Chapter PDFDocument42 pages(Download PDF) The Monstrous Feminine in Contemporary Japanese Popular Culture Raechel Dumas Online Ebook All Chapter PDFdavid.messer693100% (15)
- Anterior Teeth Selection and Its ArrangementDocument48 pagesAnterior Teeth Selection and Its ArrangementAnonymous NFiQTb1No ratings yet
- Awareness Towards Tobacco Consumption A CommunityDocument7 pagesAwareness Towards Tobacco Consumption A CommunityAvijit DasNo ratings yet
- Best, 2019 - Selection and Management of Commonly Used Enteral Feeding TubesDocument5 pagesBest, 2019 - Selection and Management of Commonly Used Enteral Feeding TubesThuane SalesNo ratings yet
- Good News 1968 (Vol XVII No 11-12) Nov-DecDocument24 pagesGood News 1968 (Vol XVII No 11-12) Nov-DecHerbert W. ArmstrongNo ratings yet
- Technical Data Demag Hoist Units Volume 2: Double-Rail Crab EZDH 600 - EZDH 1000 Double-Rail Crab EZLDH 600 - EZLDH 2000Document88 pagesTechnical Data Demag Hoist Units Volume 2: Double-Rail Crab EZDH 600 - EZDH 1000 Double-Rail Crab EZLDH 600 - EZLDH 2000mohammad khoraminiaNo ratings yet
- Mounted On Rails or Rubber Tyres and Is Able To Straddle Several Rows of ContainersDocument2 pagesMounted On Rails or Rubber Tyres and Is Able To Straddle Several Rows of ContainersIcha AfNo ratings yet
- H. P. Lovecraft - PolarisDocument3 pagesH. P. Lovecraft - PolarisBárbara AlvesNo ratings yet
- Employee RetentionDocument23 pagesEmployee RetentionAdv Sunil JoshiNo ratings yet
- Comprehensive Report Card: About The Problems of Sub-Health TrendsDocument3 pagesComprehensive Report Card: About The Problems of Sub-Health TrendsFitriWidiastutiNo ratings yet
- Transducer Engineering 2 Marks With AnswersDocument13 pagesTransducer Engineering 2 Marks With AnswersSridharan DNo ratings yet
- BrainDocument41 pagesBrainNishanth Siva100% (1)
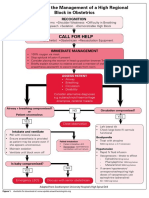
- Algorithm For The Management of A High Regional Block in ObstetricsDocument5 pagesAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNo ratings yet
- Seasonal and Inter-Market Differences in Prices of Small Ruminants in EthiopiaDocument18 pagesSeasonal and Inter-Market Differences in Prices of Small Ruminants in EthiopiaTauseefAhmadNo ratings yet
- Parables of Jesus Net BibleDocument2 pagesParables of Jesus Net Bibleapi-174346096No ratings yet