Download as pdf or txt
You might also like
- Case04.Epilepsy-Tonic ClonicDocument38 pagesCase04.Epilepsy-Tonic Clonicshivani7448No ratings yet
- Epilepsy: Assistant Lecturer: Tasneem Ahmed HamedDocument47 pagesEpilepsy: Assistant Lecturer: Tasneem Ahmed HamedAbdelrahman IbrahimNo ratings yet
- Module II 1 - EpilepsyDocument38 pagesModule II 1 - Epilepsyaysha jasimNo ratings yet
- ABP NSU PHR511 Epilepsy March 2023Document40 pagesABP NSU PHR511 Epilepsy March 2023Sajia Abedin 1821432649No ratings yet
- Anti Epileptic AgentsDocument64 pagesAnti Epileptic AgentsPrincess VanquirayNo ratings yet
- MNS Care For MO - Neurological DisordersDocument42 pagesMNS Care For MO - Neurological DisordersfatehmaanNo ratings yet
- Central Nervous System (CNS) Pharmacology (PCL 401) Antiepileptic/Anticonvulsants DrugsDocument33 pagesCentral Nervous System (CNS) Pharmacology (PCL 401) Antiepileptic/Anticonvulsants DrugsJoseph JohnNo ratings yet
- Antiepileptic Drugs (Anti-Seizure Drugs) - IDocument39 pagesAntiepileptic Drugs (Anti-Seizure Drugs) - Inouramansour235No ratings yet
- Diagnosis of EpilepsyDocument6 pagesDiagnosis of EpilepsythapanNo ratings yet
- Anti Epileptic AgentsDocument78 pagesAnti Epileptic AgentsPrincess VanquirayNo ratings yet
- Tinjauan Pustaka EpilepsiDocument34 pagesTinjauan Pustaka EpilepsisyahrurroziNo ratings yet
- Antiseizure DrugsDocument3 pagesAntiseizure DrugsCarissa Mae Tapec EstradaNo ratings yet
- Talak KejangDocument52 pagesTalak KejangRiga Medina IINo ratings yet
- Anti-Epileptic DrugsDocument70 pagesAnti-Epileptic DrugsNAYEEMA JAMEEL ANUVANo ratings yet
- Management of Seizures in Palliative Care: Journal ClubDocument63 pagesManagement of Seizures in Palliative Care: Journal ClubleungsukhingNo ratings yet
- 1.2 Anti-Seizure DrugsDocument43 pages1.2 Anti-Seizure DrugsRaymond LundaNo ratings yet
- EpilepsyDocument73 pagesEpilepsyabenezer g/kirstosNo ratings yet
- Antiepileptic Drugs: Department of Pharmacology Zhang Yan-MeiDocument28 pagesAntiepileptic Drugs: Department of Pharmacology Zhang Yan-MeiDrMohammed AlyNo ratings yet
- Drug Induced Movement DisorderDocument136 pagesDrug Induced Movement DisorderYamini DevendranNo ratings yet
- Seizure Triggers: Maria Raquel Lopez. M.D Miami VhaDocument25 pagesSeizure Triggers: Maria Raquel Lopez. M.D Miami VhashakkiryousufNo ratings yet
- Neuropharmacology III: Anticonvulsants What Are Seizures?Document6 pagesNeuropharmacology III: Anticonvulsants What Are Seizures?Urugonda VenumadhavNo ratings yet
- Module 8Document5 pagesModule 8Yuki Xairah TunayNo ratings yet
- The Medical and Surgical Treatment of EpilepsyDocument37 pagesThe Medical and Surgical Treatment of EpilepsyTammie YoungNo ratings yet
- AnticonvulsantsDocument50 pagesAnticonvulsantsvimalaNo ratings yet
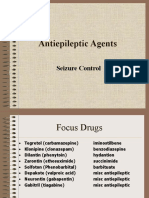
- Antiepileptic Agents: Seizure ControlDocument25 pagesAntiepileptic Agents: Seizure ControlnetandeeNo ratings yet
- Farmakologi Dari Obat EpilepsiDocument82 pagesFarmakologi Dari Obat EpilepsiDion SaputraNo ratings yet
- Psychopharmacology - Dr. Citra Ayu Aprilia, M.kes - Rabu 19 Oktober 2022 - 07.00 - 08.50 - EditDocument99 pagesPsychopharmacology - Dr. Citra Ayu Aprilia, M.kes - Rabu 19 Oktober 2022 - 07.00 - 08.50 - EditCITRA AYU APRILIANo ratings yet
- Epilepsy and Seizure DisordersDocument160 pagesEpilepsy and Seizure DisordersIM100% (1)
- Anxiolytics & AntidepressantsDocument34 pagesAnxiolytics & AntidepressantsIconMaicoNo ratings yet
- Antiepileptic DrugsDocument65 pagesAntiepileptic DrugsZarish IftikharNo ratings yet
- Epilepsy 34Document102 pagesEpilepsy 34Dian zaini PutraNo ratings yet
- Seminar On SEDocument49 pagesSeminar On SEmubarak abdulkadirNo ratings yet
- IV. Antiepileptic DrugsDocument31 pagesIV. Antiepileptic DrugsDanica AbarquezNo ratings yet
- SeizuresDocument15 pagesSeizuresStevenNo ratings yet
- Anti Epileptic DrugsDocument89 pagesAnti Epileptic DrugsInderjeet SohalNo ratings yet
- Therapy (LLL)Document432 pagesTherapy (LLL)Biruk DesalegnNo ratings yet
- Treatment of Schizophrenia and Management of Drug SideDocument83 pagesTreatment of Schizophrenia and Management of Drug SideAbelNo ratings yet
- Online Content: Stopping Medicines - AntipsychoticsDocument3 pagesOnline Content: Stopping Medicines - AntipsychoticsLouiseNo ratings yet
- Anti ConvulsantsDocument72 pagesAnti ConvulsantsPournima BhalekarNo ratings yet
- Pain, Multiple Organ Failre, Hepatic EncphalopathyDocument42 pagesPain, Multiple Organ Failre, Hepatic Encphalopathyيارب Ya RaBNo ratings yet
- Nausea Vomiting - DhitaDocument78 pagesNausea Vomiting - DhitaweNo ratings yet
- SeizuresDocument19 pagesSeizuresSandhya BasnetNo ratings yet
- The Practical Management of Status Epilepticus: David Y. Gosal, Neuro SPR, Manchester Neurosciences CentreDocument51 pagesThe Practical Management of Status Epilepticus: David Y. Gosal, Neuro SPR, Manchester Neurosciences CentreontakecilNo ratings yet
- Epilepsy & Antiepileptic Drugs: Dr. Siva Priya Sonali Thanushanthan Tivashkar Srinaath SidhantasahooDocument40 pagesEpilepsy & Antiepileptic Drugs: Dr. Siva Priya Sonali Thanushanthan Tivashkar Srinaath Sidhantasahoothanush_15No ratings yet
- Presented By: Mr. EbDocument65 pagesPresented By: Mr. EbEbson De la RochaNo ratings yet
- Conscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantDocument84 pagesConscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantKhaled GharaibehNo ratings yet
- Approach To DeliriumDocument23 pagesApproach To DeliriumyashaswiniguNo ratings yet
- Epilepsy NewDocument24 pagesEpilepsy Newrichardkikondo5No ratings yet
- Alcohol w1Document17 pagesAlcohol w1Blogz HuckerNo ratings yet
- Anxiolytic and Hypnotic AgentsDocument50 pagesAnxiolytic and Hypnotic AgentsMoxie Macado100% (1)
- Pharmacology PremedicationDocument12 pagesPharmacology PremedicationspringshemantNo ratings yet
- Anti-Convulsants/Antiepileptic Drugs: Prepared By: DR Sana FaheemDocument23 pagesAnti-Convulsants/Antiepileptic Drugs: Prepared By: DR Sana Faheemaziz aliNo ratings yet
- Anti Psychotic DrugDocument25 pagesAnti Psychotic DrugANI SAMNo ratings yet
- Anesthesia For Electroconvulsive Therapy - UjoDocument17 pagesAnesthesia For Electroconvulsive Therapy - UjopujoNo ratings yet
- Drugs For ObesityDocument41 pagesDrugs For ObesityBiplav SinghNo ratings yet
- HeadacheDocument24 pagesHeadacheshayma khanNo ratings yet
- CHAPTER 19: Drugs Used For Seizure DisordersDocument19 pagesCHAPTER 19: Drugs Used For Seizure DisordersAziil LiizaNo ratings yet
- Opiod AnalgesicsDocument13 pagesOpiod Analgesicschebetnaomi945No ratings yet
- PrognosisDocument8 pagesPrognosisallkhusairy6tuansiNo ratings yet
- Medical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcFrom EverandMedical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcNo ratings yet
- D E R M: Litt'sDocument706 pagesD E R M: Litt'sshintaNo ratings yet
- Types of Insulin: NOTE: Exact Onset, Action, and Duration Are Dependent On The Generic/brand UsedDocument3 pagesTypes of Insulin: NOTE: Exact Onset, Action, and Duration Are Dependent On The Generic/brand Usedask1400No ratings yet
- Culture Aerobic: Final Laboratory ReportDocument3 pagesCulture Aerobic: Final Laboratory Reportdr.diagnostics.labNo ratings yet
- Vaccination MF218710Document1 pageVaccination MF218710Zin KoNo ratings yet
- JC GenericDocument8 pagesJC Genericchairez doroteoNo ratings yet
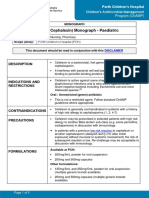
- Cefalexin (Cephalexin) Monograph - Paediatric: DescriptionDocument5 pagesCefalexin (Cephalexin) Monograph - Paediatric: Descriptioneinas omerNo ratings yet
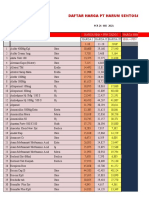
- Daftar Harga PT Harum Sentosa: Harga Hna + PPN Gado2 Harga Hna + PPN Khusus HarsenDocument40 pagesDaftar Harga PT Harum Sentosa: Harga Hna + PPN Gado2 Harga Hna + PPN Khusus HarsenFahmi HaryadinNo ratings yet
- Hirsutism: Diagnosis and TreatmentDocument6 pagesHirsutism: Diagnosis and TreatmentAnonymous ysrxggk21cNo ratings yet
- Iv Computation QuestionsDocument4 pagesIv Computation QuestionsJasmine YntigNo ratings yet
- Bromhexine HCL Syrup 4 MGDocument1 pageBromhexine HCL Syrup 4 MGTrishiaNo ratings yet
- Drugstoavoidlist 3 PDFDocument3 pagesDrugstoavoidlist 3 PDFBradNo ratings yet
- Clinical Trial Roadmap Template - WsDocument4 pagesClinical Trial Roadmap Template - WsDaniel AlejandroNo ratings yet
- Asic InformationDocument2 pagesAsic InformationJaymark Pineda TiglaoNo ratings yet
- Pharmacology SEQDocument1 pagePharmacology SEQZEESHAN YOUSUFNo ratings yet
- Insulin RegularDocument1 pageInsulin RegularChristopher LeeNo ratings yet
- Acetylcysteine (Fluimucil)Document2 pagesAcetylcysteine (Fluimucil)Chelsy MurielNo ratings yet
- HexpharmDocument4 pagesHexpharmMuhammad FaridNo ratings yet
- Topical Corticosteroids: HighlightsDocument3 pagesTopical Corticosteroids: HighlightsNico Handreas TiantoNo ratings yet
- Equations Sheet - v2Document9 pagesEquations Sheet - v2angelamnsr100% (1)
- M2C19 Types of InsulinDocument2 pagesM2C19 Types of Insulinirnumambreen15No ratings yet
- Generics Act of 1988Document15 pagesGenerics Act of 1988aica baesNo ratings yet
- 2020 Ed Dilution ProtocolDocument72 pages2020 Ed Dilution ProtocolTuan SharatulNo ratings yet
- Pioglitazone (Actos, Lilly) : May Be Confused With Actidose, ActonelDocument3 pagesPioglitazone (Actos, Lilly) : May Be Confused With Actidose, Actonelshidyakg100% (1)
- Bismuth SubsalicylateDocument7 pagesBismuth SubsalicylateHendroNo ratings yet
- A Folha6-Adenda-Salvia DivinorumDocument1 pageA Folha6-Adenda-Salvia DivinorumglauberNo ratings yet
- Hydroxychloroquine PELDocument3 pagesHydroxychloroquine PELscribd_deepak100% (1)
- Required Dose Weight in Kgs X Dosage Per KG: Clark's Rule Young's Rule Fried's Rule Average Adult DoseDocument1 pageRequired Dose Weight in Kgs X Dosage Per KG: Clark's Rule Young's Rule Fried's Rule Average Adult DoseNicolai MabituinNo ratings yet
- Editorial: Dental Caries and OsteoporosisDocument2 pagesEditorial: Dental Caries and OsteoporosisBagis Emre GulNo ratings yet
- Anti-Hiv Drug Discovery PDFDocument18 pagesAnti-Hiv Drug Discovery PDFMandapati JanakiramNo ratings yet
- PharmaLite - in Pharmacy Practice (PV Publication)Document276 pagesPharmaLite - in Pharmacy Practice (PV Publication)MD SALAHUDDIN SALAHUDDINNo ratings yet