Download as pdf or txt
You might also like
- Test Certificate of BitumenDocument1 pageTest Certificate of BitumenAmit Prasad50% (2)
- Case 3-2020: A 44-Year-Old Man With Weight Loss, Diarrhea, and Abdominal PainDocument10 pagesCase 3-2020: A 44-Year-Old Man With Weight Loss, Diarrhea, and Abdominal PainAlvaro Andres Flores JimenezNo ratings yet
- NEJM Case Report 40-2017Document10 pagesNEJM Case Report 40-2017A. Rauf100% (1)
- Case 2-2019 - A 36-Year-Old Man With Rash, Abdominal Pain, and Lymphadenopathy - Chen Et Al - 2019Document9 pagesCase 2-2019 - A 36-Year-Old Man With Rash, Abdominal Pain, and Lymphadenopathy - Chen Et Al - 2019nejdNo ratings yet
- Case 31 - 2019Document12 pagesCase 31 - 2019Gustavo AngelesNo ratings yet
- Case 2-2013: A 20-Year-Old Man With Recurrent Ear Pain, Fever, and HeadacheDocument11 pagesCase 2-2013: A 20-Year-Old Man With Recurrent Ear Pain, Fever, and HeadachedrfmentNo ratings yet
- 10 1056@NEJMcpc1913468 PDFDocument10 pages10 1056@NEJMcpc1913468 PDFAbdelkader HociniNo ratings yet
- Case 15-2017: A 27-Year-Old Woman With Anemia, Thrombocytosis, and Skin Lesions After Travel AbroadDocument10 pagesCase 15-2017: A 27-Year-Old Woman With Anemia, Thrombocytosis, and Skin Lesions After Travel AbroadGénesis LeónNo ratings yet
- Case 1-2010Document11 pagesCase 1-2010isravg94No ratings yet
- NEJM 5 Colitis UlcerosaDocument11 pagesNEJM 5 Colitis Ulcerosa0228154No ratings yet
- Caso 24 2016NEJMcpc1503829Document14 pagesCaso 24 2016NEJMcpc1503829claudia montesNo ratings yet
- Case 8-2019: A 58-Year-Old Woman With Vision Loss, Headaches, and Oral UlcersDocument10 pagesCase 8-2019: A 58-Year-Old Woman With Vision Loss, Headaches, and Oral UlcersHossam MagdyNo ratings yet
- Journal Nejmcpc1208145Document10 pagesJournal Nejmcpc1208145Irmagian PaleonNo ratings yet
- Nejmcpc 2300910Document9 pagesNejmcpc 2300910carb0ne14rNo ratings yet
- Nej M CPC 2115849Document13 pagesNej M CPC 2115849Dinesh KumaarNo ratings yet
- Faring It IsDocument10 pagesFaring It Isnanda tsalasaniNo ratings yet
- Nejmcpc 2027096Document10 pagesNejmcpc 2027096Camille MalilayNo ratings yet
- Caso Clínico para A P1 - Vale 1 Ponto ExtraDocument11 pagesCaso Clínico para A P1 - Vale 1 Ponto ExtraNubia Ferrari GuedesNo ratings yet
- Nej M CPC 1209935Document9 pagesNej M CPC 1209935drfmentNo ratings yet
- Acute Kidney FailureDocument8 pagesAcute Kidney FailureJuan Diego Ferreyros ArroyoNo ratings yet
- Caso Clinico - SepsisDocument9 pagesCaso Clinico - SepsisJavier EspezuaNo ratings yet
- Caso Especial Grupo 1Document18 pagesCaso Especial Grupo 1Josè BermúdezNo ratings yet
- A 43-Year-Old Man With Diabetes, Hypogonadism, Cirrhosis, Arthralgias, and FatigueDocument8 pagesA 43-Year-Old Man With Diabetes, Hypogonadism, Cirrhosis, Arthralgias, and FatigueLara SousaNo ratings yet
- Nej M CPC 2100282Document10 pagesNej M CPC 2100282Paulo Ricardo D. PereiraNo ratings yet
- Case 11-2009 - A 47-Year-Old Man With Fever, Headache, Rash, and VomitingDocument9 pagesCase 11-2009 - A 47-Year-Old Man With Fever, Headache, Rash, and VomitingcmirceaNo ratings yet
- Caso NEJM 27-2017Document9 pagesCaso NEJM 27-2017Leonardo PgNo ratings yet
- Nej M CPC 2309382Document8 pagesNej M CPC 2309382mnf6bb2tckNo ratings yet
- Aula 2 - Artigo PDFDocument9 pagesAula 2 - Artigo PDFGabriella CarmoNo ratings yet
- Case 3-2019 - A 70-Year-Old Woman With Fever, Headache, and Progressive Encephalopathy - Zachary Et Al - 2019Document8 pagesCase 3-2019 - A 70-Year-Old Woman With Fever, Headache, and Progressive Encephalopathy - Zachary Et Al - 2019nejdNo ratings yet
- NEJMcpc 2312731Document11 pagesNEJMcpc 2312731cehborrotoNo ratings yet
- Chronic Myeloid Leukemia: Chronic Phase Presenting As Extramedullary PresentationDocument6 pagesChronic Myeloid Leukemia: Chronic Phase Presenting As Extramedullary PresentationOjas MahajanNo ratings yet
- Koch 2011Document9 pagesKoch 2011andrescortez150No ratings yet
- Detection and Molecular Characterization of A Novel Large Babesia Species in A Dog 2004 VeterinarDocument10 pagesDetection and Molecular Characterization of A Novel Large Babesia Species in A Dog 2004 VeterinarGabriela Victoria MartinescuNo ratings yet
- Pancytopenia - A Clinicopathological Analysis of 132 CasesDocument11 pagesPancytopenia - A Clinicopathological Analysis of 132 CasesKaye Antonette AntioquiaNo ratings yet
- CML PresentationDocument55 pagesCML PresentationИван НегарэNo ratings yet
- Case 21-2012: A 27-Year-Old Man With Fatigue, Weakness, Weight Loss, and Decreased LibidoDocument13 pagesCase 21-2012: A 27-Year-Old Man With Fatigue, Weakness, Weight Loss, and Decreased Libidodamian velmonteNo ratings yet
- Nej M CPC 2103461Document10 pagesNej M CPC 2103461monaNo ratings yet
- Fmed 07 617786Document5 pagesFmed 07 617786Ashifa AshfaNo ratings yet
- Fmed 07 617786Document5 pagesFmed 07 617786Ashifa AshfaNo ratings yet
- A Case of Acute Tuberculous Pleuropneumonia in A Patient With Acute Lymphoblastic LeukemiaDocument9 pagesA Case of Acute Tuberculous Pleuropneumonia in A Patient With Acute Lymphoblastic LeukemiaEasti EmoraNo ratings yet
- Iron Overload and Hepatic Fibrosis in Response - JMDocument1 pageIron Overload and Hepatic Fibrosis in Response - JMBastomy EkaNo ratings yet
- Ancylostoma Duodenale Presented As Severe Anaemia: A Case Report in A Tertiary Care Centre, North-East IndiaDocument5 pagesAncylostoma Duodenale Presented As Severe Anaemia: A Case Report in A Tertiary Care Centre, North-East IndiaIJAR JOURNALNo ratings yet
- Circulating Biomarkers For Long-TermDocument9 pagesCirculating Biomarkers For Long-TermSofia AraujoNo ratings yet
- Clinical Case of A Man With Abdominal Pain and HematocheziaDocument13 pagesClinical Case of A Man With Abdominal Pain and HematocheziaLoralie Evangeline Perez-MirandaNo ratings yet
- ContrastDocument6 pagesContrastYahya AlmalkiNo ratings yet
- ReportViewer 1Document4 pagesReportViewer 1Shehriyar KhanNo ratings yet
- Caso 2Document10 pagesCaso 2Luanna DávilaNo ratings yet
- Ofx163 1546Document2 pagesOfx163 1546crisNo ratings yet
- HLND 2017Document15 pagesHLND 2017Lauren ReckNo ratings yet
- Hu Et Al-2017-Journal of Cellular PhysiologyDocument37 pagesHu Et Al-2017-Journal of Cellular PhysiologySorop AndreiNo ratings yet
- Shortness of Breath in A 74-Year-Old WomanDocument5 pagesShortness of Breath in A 74-Year-Old WomanNicole Villanueva, BSN - Level 3ANo ratings yet
- Clinical Hematology Case StudyDocument6 pagesClinical Hematology Case StudyRomie SolacitoNo ratings yet
- Incidence of Bronchiolitis Associated HospitalizatDocument2 pagesIncidence of Bronchiolitis Associated HospitalizatBastomy EkaNo ratings yet
- Diagnosis of Blood and Bone Marrow DisordersFrom EverandDiagnosis of Blood and Bone Marrow DisordersSa A. WangNo ratings yet
- Nejmcpc 1208152Document10 pagesNejmcpc 1208152FrinkooFrinkoBNo ratings yet
- Eli SpotDocument20 pagesEli SpotAdel HamadaNo ratings yet
- Serum Neuroinflammatory Disease-Induced Central Nervous System Proteins Predict Clinical Onset of Experimental Autoimmune EncephalomyelitisDocument15 pagesSerum Neuroinflammatory Disease-Induced Central Nervous System Proteins Predict Clinical Onset of Experimental Autoimmune EncephalomyelitisIchim MadalinaNo ratings yet
- Zika MeningoensefalitisDocument4 pagesZika MeningoensefalitisBangun Said SantosoNo ratings yet
- Uso CorticoidesDocument9 pagesUso CorticoidesRolando Lopez ZegarraNo ratings yet
- Https:neuronaldo - Com.br:wp Content:uploads:2012:04:7 Actinomyces Paper JVDI Final 7 2015Document6 pagesHttps:neuronaldo - Com.br:wp Content:uploads:2012:04:7 Actinomyces Paper JVDI Final 7 2015Lucas XavierNo ratings yet
- Molecular Medicine: Genomics to Personalized HealthcareFrom EverandMolecular Medicine: Genomics to Personalized HealthcareRating: 5 out of 5 stars5/5 (1)
- Laparoscopic Bilateral Tubal LigationDocument2 pagesLaparoscopic Bilateral Tubal Ligationapi-3712326100% (1)
- Notes 20221031134541Document6 pagesNotes 20221031134541ppriyareddy10No ratings yet
- Water Proof Breathable FabricDocument13 pagesWater Proof Breathable Fabricjack omeNo ratings yet
- The Feasiblity of Using Indigenous DyestuffDocument2 pagesThe Feasiblity of Using Indigenous Dyestuffalvin90% (10)
- Quante CDocument4 pagesQuante CAnonymous faRVVGNNo ratings yet
- Thesis On A Homicide Ending ExplanationDocument4 pagesThesis On A Homicide Ending Explanationbkxgnsw4100% (2)
- William M Leahey - Bullying The BulliesDocument8 pagesWilliam M Leahey - Bullying The BullieswilliammleaheyNo ratings yet
- (Lib24.vn) Bai-Tap-Doc-Hieu-Tieng-Anh-Lop-6Document4 pages(Lib24.vn) Bai-Tap-Doc-Hieu-Tieng-Anh-Lop-6Hoa MỹNo ratings yet
- Comparacion Polar y VO2 MaxDocument3 pagesComparacion Polar y VO2 MaxZilanyaid MontoyaNo ratings yet
- Valvulas XT PDFDocument4 pagesValvulas XT PDFIsidro Gomez GarciaNo ratings yet
- Turmeric Powder Coriander Powder and Chilli Powder Processing IndustryDocument107 pagesTurmeric Powder Coriander Powder and Chilli Powder Processing IndustryAlexNo ratings yet
- ButaneDocument6 pagesButaneRatu Fajrina HanifaNo ratings yet
- Relationship Between Quality of Life and Social SupportDocument9 pagesRelationship Between Quality of Life and Social SupportDragos IvanNo ratings yet
- About Beximco Pharmaceuticals LimitedDocument9 pagesAbout Beximco Pharmaceuticals LimitedAsaduzzamannayanNo ratings yet
- RRLDocument6 pagesRRLTintin GatdulaNo ratings yet
- RRM's ProfileDocument2 pagesRRM's ProfilemanjinderenerconNo ratings yet
- Chapter 20: Medicine - Set ADocument4 pagesChapter 20: Medicine - Set ABernard Paul GuintoNo ratings yet
- DO Transfer PumpDocument40 pagesDO Transfer PumpUdana HettiarachchiNo ratings yet
- CAIE8 - Physics - PT3 - Revision WorksheetDocument11 pagesCAIE8 - Physics - PT3 - Revision WorksheetadityadabxNo ratings yet
- 09-22-2021 Original Complaint by Austin ISD Against District Over Covid-19 PoliciesDocument278 pages09-22-2021 Original Complaint by Austin ISD Against District Over Covid-19 PoliciesCBS Austin WebteamNo ratings yet
- Bedside OrientationDocument3 pagesBedside OrientationPhranie YhaaNo ratings yet
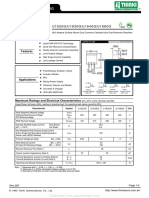
- U1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GDocument2 pagesU1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GTeles SilvaNo ratings yet
- Safety Standard For Horizontal Carousel Material Handling and Associated EquipmentDocument19 pagesSafety Standard For Horizontal Carousel Material Handling and Associated EquipmentIntegrated Systems DesignNo ratings yet
- SCIENCE P1 - (PHYSICS) G10-12 eBOOK PDFDocument209 pagesSCIENCE P1 - (PHYSICS) G10-12 eBOOK PDFPaul HymanNo ratings yet
- 2023 2024 Catalogue Unimed D1.3 231023Document145 pages2023 2024 Catalogue Unimed D1.3 231023octaviaNo ratings yet
- Criminal Law - DPP v. BeardDocument11 pagesCriminal Law - DPP v. BeardipragalbhNo ratings yet
- Pharmacology Powerpoint Group 1Document38 pagesPharmacology Powerpoint Group 1Daniel LaurenteNo ratings yet
- EC Lab ManualDocument5 pagesEC Lab ManualsruthyNo ratings yet
- Metode Penelitian EtnobiologiDocument31 pagesMetode Penelitian EtnobiologiAnonymous fbUJwFVPNo ratings yet