Download as docx, pdf, or txt
You might also like
- Psychiatric Nursing Ebook 8th Edition Ebook PDFDocument61 pagesPsychiatric Nursing Ebook 8th Edition Ebook PDFcarey.sowder235100% (46)
- Integrated Pharmacology - Page, Curtis, Sutter, Walker, HoffmanDocument601 pagesIntegrated Pharmacology - Page, Curtis, Sutter, Walker, HoffmanCarlos BojorquezNo ratings yet
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- 2 0CommDiseaseIMPTVisionDocument3 pages2 0CommDiseaseIMPTVisionAndrea Patricia DaquialNo ratings yet
- Main Submitter SpeechDocument2 pagesMain Submitter SpeechArham100% (1)
- HSB Pneumonia Antibiotic AlgorithmDocument4 pagesHSB Pneumonia Antibiotic AlgorithmDr.Senthil KumarNo ratings yet
- Drug Study AZITHROMYCINDocument2 pagesDrug Study AZITHROMYCINDannah BulliandayNo ratings yet
- Clostridoides DifficileDocument2 pagesClostridoides Difficileyabhas chhetriNo ratings yet
- PHARMA MIDTERM 2ndyrnsgDocument38 pagesPHARMA MIDTERM 2ndyrnsgquincy fajardoNo ratings yet
- SHC ABSSSI ED CDU GuidelineDocument4 pagesSHC ABSSSI ED CDU GuidelineHector Sanchez LacayoNo ratings yet
- IMG EmpAposterDocument1 pageIMG EmpAposterChiu LeoNo ratings yet
- Superficial Fungal InfectionsDocument33 pagesSuperficial Fungal InfectionsBriana NdayisabaNo ratings yet
- Pal EarningsDocument107 pagesPal EarningsSarah Ong SiuNo ratings yet
- MetronidazoleDocument2 pagesMetronidazoleGwyn RosalesNo ratings yet
- Thrombolic, Thrombocytopenic Purpurvhemoclytic Uremic Syndrome (SeizuresDocument1 pageThrombolic, Thrombocytopenic Purpurvhemoclytic Uremic Syndrome (Seizuresgeorgeloto12No ratings yet
- Infectious Diseases USMLE Notes (Free Trial)Document1 pageInfectious Diseases USMLE Notes (Free Trial)Laura Tapia100% (1)
- Macrolide Drug StudyDocument3 pagesMacrolide Drug StudyEmagra AzilNo ratings yet
- Furosemide Drug Study CompressDocument1 pageFurosemide Drug Study CompressAngelica TolledoNo ratings yet
- SmfnduhDocument2 pagesSmfnduhKapy KapsNo ratings yet
- CandidiasisDocument5 pagesCandidiasisGallel PanumNo ratings yet
- Drug Study-ClindamycinDocument3 pagesDrug Study-ClindamycinDUMANGENG ELLAINE D.100% (1)
- CNS Infection GuidanceDocument2 pagesCNS Infection GuidanceGus LionsNo ratings yet
- CNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Document1 pageCNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Fitri RachmadaniNo ratings yet
- Diphteria, Pertussis and Staphylococcal Infections-1Document15 pagesDiphteria, Pertussis and Staphylococcal Infections-1Nwosu Ogbonna GabrielNo ratings yet
- LidocaineDocument4 pagesLidocaineAhmad Fauzi100% (1)
- Antibiotic Pocket GuideDocument19 pagesAntibiotic Pocket GuideNaomi Liang100% (1)
- COVID - Management 14 April 2021Document20 pagesCOVID - Management 14 April 2021Zain ZaidiNo ratings yet
- NCP & Drug Study (Karisha Guevarra)Document17 pagesNCP & Drug Study (Karisha Guevarra)Karisha GuevarraNo ratings yet
- 2018 Ohp Syphilis Staging and Treatment 2018 053018Document3 pages2018 Ohp Syphilis Staging and Treatment 2018 053018Pravin SurendranNo ratings yet
- Clindamycin Drug Study WWW RNpedia ComDocument4 pagesClindamycin Drug Study WWW RNpedia ComChristian LlerinNo ratings yet
- INFECTIONSDocument4 pagesINFECTIONSRico Shaun CalapreNo ratings yet
- Onco Emergencies TLS (Increased U, K, Phos Decreased Ca) HyperleukocytosisDocument18 pagesOnco Emergencies TLS (Increased U, K, Phos Decreased Ca) HyperleukocytosisMaceyJamesNo ratings yet
- F8DB F089:Fungal InfectionsDocument6 pagesF8DB F089:Fungal InfectionsPharmacist Ehab HammadNo ratings yet
- CandidiasisDocument27 pagesCandidiasisfarmasi_hmNo ratings yet
- AmikinDocument2 pagesAmikinLIEZEL GRACE VELAYONo ratings yet
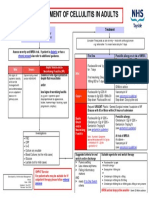
- Cellulitis 2014 FinalDocument1 pageCellulitis 2014 FinalIntan Mega PratidianaNo ratings yet
- Empiric Antibiotic ListDocument2 pagesEmpiric Antibiotic ListpasswordNo ratings yet
- Gentamicin Sulfate-Drug StudyDocument3 pagesGentamicin Sulfate-Drug StudyDaisy Palisoc82% (11)
- PCP Treatment GeneralDocument1 pagePCP Treatment GeneralLegolas gantengNo ratings yet
- Drug Study Amoxicillin PDFDocument4 pagesDrug Study Amoxicillin PDFMc SantosNo ratings yet
- Candidiasis 161115175237Document1 pageCandidiasis 161115175237Cikw KuzhaNo ratings yet
- MeningitisDocument5 pagesMeningitisdqnxfdw6bjNo ratings yet
- NICU ABX ChartDocument11 pagesNICU ABX ChartdrchiNo ratings yet
- Vancomycin DRUGSTUDYDocument3 pagesVancomycin DRUGSTUDYEmagra AzilNo ratings yet
- Drug StudyDocument10 pagesDrug StudyJessica GlitterNo ratings yet
- Drug Data Classificatio N Indications Contraindicatio N Adverse Effects Nursing ResponsibilitiesDocument1 pageDrug Data Classificatio N Indications Contraindicatio N Adverse Effects Nursing ResponsibilitiesJake Yvan DizonNo ratings yet
- Derm TreatmentsDocument5 pagesDerm Treatmentsemilyjvaldez99No ratings yet
- Section 14 Cellulitis ProtDocument1 pageSection 14 Cellulitis Protqusai100No ratings yet
- Del Rosario Ryan D. BSN 4C1-7 Mr. Daniel Mon Mamanao: Measles Pre-Eruptive StageDocument5 pagesDel Rosario Ryan D. BSN 4C1-7 Mr. Daniel Mon Mamanao: Measles Pre-Eruptive Stageryandelrosario9yahooNo ratings yet
- DrugStudy FluconazoleCasilaoDocument4 pagesDrugStudy FluconazoleCasilaoArone SebastianNo ratings yet
- Protcolo NacDocument2 pagesProtcolo NacJdmp Lopez MorenoNo ratings yet
- Mindanao State University - Iligan Institute of Technology Student: ALEXA MURIEL L. MOZAR Section: BLOCK 261Document2 pagesMindanao State University - Iligan Institute of Technology Student: ALEXA MURIEL L. MOZAR Section: BLOCK 261Alexandra AntondyNo ratings yet
- DRUGSTUDYDocument8 pagesDRUGSTUDYWinnie Salazar AriolaNo ratings yet
- Calici Viri DaeDocument5 pagesCalici Viri DaeGabrielle IsnardNo ratings yet
- Covid 19 Severe Disease ManagmentDocument1 pageCovid 19 Severe Disease ManagmentAbdullah KhanNo ratings yet
- Drug Study - HemoDocument2 pagesDrug Study - HemoReyna Chame GarcinezNo ratings yet
- 18.1 - Infectious DiseasesDocument129 pages18.1 - Infectious DiseasesWarda TajammalNo ratings yet
- VancomycinDocument2 pagesVancomycinRomwella May AlgoNo ratings yet
- Treatment of STDsDocument6 pagesTreatment of STDsSa MaNo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Take One Nursing Final Coaching Ms CriticalDocument29 pagesTake One Nursing Final Coaching Ms Criticalnot your medz duranNo ratings yet
- Bagong DrugsDocument7 pagesBagong DrugsmcensoredNo ratings yet
- The Most Common Drugs Used in The EarDocument4 pagesThe Most Common Drugs Used in The EarAzizurahmanNo ratings yet
- Health 9 - Q2 - Mod2-TheRiskandProtectiveFactorsofUsingDrugs-v1Document20 pagesHealth 9 - Q2 - Mod2-TheRiskandProtectiveFactorsofUsingDrugs-v1Grace Paculba Baldicana100% (7)
- Government Mediated Access Price PhilippinesDocument4 pagesGovernment Mediated Access Price PhilippinesKristin0% (2)
- The Effect of Housing and Gender On Preference For Morphine-Sucrose Solutions in RatsDocument5 pagesThe Effect of Housing and Gender On Preference For Morphine-Sucrose Solutions in RatsqweqweqweqwzaaaNo ratings yet
- NPTE CArdio NotesDocument27 pagesNPTE CArdio NotesAubrey Vale SagunNo ratings yet
- Colegio de San Gabriel Arcangel: Learning Activity Sheet (Las)Document3 pagesColegio de San Gabriel Arcangel: Learning Activity Sheet (Las)Jonille EchevarriaNo ratings yet
- College of Nursing: Cebu Normal UniversityDocument3 pagesCollege of Nursing: Cebu Normal UniversityShiva TorinsNo ratings yet
- Pharmacy and Therapeutic CommitteeDocument14 pagesPharmacy and Therapeutic CommitteerjNo ratings yet
- Japanese Apricot (Ume) : A Novel Therapeutic Approach For The Treatment of PeriodontitisDocument14 pagesJapanese Apricot (Ume) : A Novel Therapeutic Approach For The Treatment of PeriodontitisGeorgiGugicevNo ratings yet
- Berberine Ameliorates Hyperglycemia in Alloxan-Induced Diabetic C57BL/6 Mice Through Activation of Akt Signaling PathwayDocument8 pagesBerberine Ameliorates Hyperglycemia in Alloxan-Induced Diabetic C57BL/6 Mice Through Activation of Akt Signaling PathwaySunny Side Up SunNo ratings yet
- Implications of Antimicrobial Resistance During Acne Treatment: Review ArticleDocument3 pagesImplications of Antimicrobial Resistance During Acne Treatment: Review Articleoctavio oliveiraNo ratings yet
- Sustainable Uses and Prospects of Medicinal Plants ALGRAWANY 2023Document465 pagesSustainable Uses and Prospects of Medicinal Plants ALGRAWANY 2023Ricercatore dì veritàNo ratings yet
- Liver Complications - SLEDocument5 pagesLiver Complications - SLEFanny PritaningrumNo ratings yet
- Medicinal Uses of Mushroom: Amit PrasadDocument21 pagesMedicinal Uses of Mushroom: Amit PrasadAmit PrasadNo ratings yet
- Targeted Drug DeliveryDocument10 pagesTargeted Drug DeliveryYuzak GuntoroNo ratings yet
- Peer Review Report (Lopinavir/Ritonavir (40mg/10mg) Oral Granules For Oral Suspension)Document6 pagesPeer Review Report (Lopinavir/Ritonavir (40mg/10mg) Oral Granules For Oral Suspension)Ranga NdhlovuNo ratings yet
- Chapter 16: Schizophrenia: Tomorrow: Chapter 17: Mood Disorders and SuicideDocument65 pagesChapter 16: Schizophrenia: Tomorrow: Chapter 17: Mood Disorders and SuicideRainier Moreno-LacalleNo ratings yet
- LIMEDocument2 pagesLIMEvkamlesh7199No ratings yet
- Konsep Nyeri Dan Manajemen NyeriDocument36 pagesKonsep Nyeri Dan Manajemen NyeriFira AlumanNo ratings yet
- Synthetic Iso Avones and Doping: A Novel Class of Aromatase Inhibitors?Document8 pagesSynthetic Iso Avones and Doping: A Novel Class of Aromatase Inhibitors?loki gurjarNo ratings yet
- Antimalarial Medicinal PlantsDocument329 pagesAntimalarial Medicinal Plantsdjikineaminata20No ratings yet
- Jurnal AnestesiDocument5 pagesJurnal AnestesiridwanNo ratings yet
- Module # 5 Pharmacology NursingDocument45 pagesModule # 5 Pharmacology Nursingannyeong_123No ratings yet
- Original Investigation: JamaDocument11 pagesOriginal Investigation: JamaAdel SALLAMNo ratings yet
- Hospital Pharmacy LabDocument179 pagesHospital Pharmacy LabJohn Carlo Cabueñas RagmaNo ratings yet