
Mathematical Model of Blood Glucose Dynamics by Emulating The Pathophysiology of Glucose Metabolism in Type 2 Diabetes Mellitus
Mathematical Model of Blood Glucose Dynamics by Emulating The Pathophysiology of Glucose Metabolism in Type 2 Diabetes Mellitus
You might also like
- Case Study Ectopic PregnancyDocument37 pagesCase Study Ectopic PregnancyJoule Peirre83% (6)
- Helix Installation Manual Rev 002Document112 pagesHelix Installation Manual Rev 002Edgar Mendoza100% (2)
- Market Research On Male Grooming IndustryDocument30 pagesMarket Research On Male Grooming IndustryMonalisa SethiNo ratings yet
- 4-The Impact of Body Image On Self-Esteem in AdolescentsDocument11 pages4-The Impact of Body Image On Self-Esteem in AdolescentsClinical and Counselling Psychology ReviewNo ratings yet
- From Metabolomics To FluxomicsDocument10 pagesFrom Metabolomics To FluxomicscamartinezriNo ratings yet
- RM ProtocolDocument4 pagesRM Protocolcifha diasNo ratings yet
- Palumbo 13Document13 pagesPalumbo 13Margarete Ap SantosNo ratings yet
- Transcriptomic and Proteomic Analysis of Potential Therapeutic Target Genes in The Liver of Metformin Treated Sprague Dawley Rats With Type 2 Diabetes Mellitusijmm-41!06!3327Document15 pagesTranscriptomic and Proteomic Analysis of Potential Therapeutic Target Genes in The Liver of Metformin Treated Sprague Dawley Rats With Type 2 Diabetes Mellitusijmm-41!06!3327ErickNo ratings yet
- 110 320 1 PB PDFDocument10 pages110 320 1 PB PDFMirna AisyahNo ratings yet
- 110 320 1 PB PDFDocument10 pages110 320 1 PB PDFMirna AisyahNo ratings yet
- Diabetes MellitusDocument17 pagesDiabetes MellitusIkekielNo ratings yet
- tmp22D3 TMPDocument9 pagestmp22D3 TMPFrontiersNo ratings yet
- Quasi-Model-Based Control of Type 1 Diabetes MelliDocument14 pagesQuasi-Model-Based Control of Type 1 Diabetes MellifhamdiNo ratings yet
- Simplified Mathematical Model of Glucose-Insulin SystemDocument12 pagesSimplified Mathematical Model of Glucose-Insulin SystemBrasoveanu GheorghitaNo ratings yet
- Else 2020 Conference 2Document7 pagesElse 2020 Conference 2Chestionar SanatateNo ratings yet
- ImplantDocument8 pagesImplantTabishur RahmanNo ratings yet
- Glucose Variability - FullDocument12 pagesGlucose Variability - FullAlina PopaNo ratings yet
- Research ArticleDocument8 pagesResearch ArticlebegumbahceciNo ratings yet
- A Phenomenological-Based Semi-Physical Model of The Kidneys and Its Role inDocument32 pagesA Phenomenological-Based Semi-Physical Model of The Kidneys and Its Role inronni bermudezNo ratings yet
- Metabolites 13 00222 v3Document12 pagesMetabolites 13 00222 v3Salva SVNo ratings yet
- Measurement of Glucose Homeostasis in VivoDocument10 pagesMeasurement of Glucose Homeostasis in Vivo19400668No ratings yet
- Thorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsDocument12 pagesThorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsgercampeNo ratings yet
- Robust PBPK/PD-Based Model PredictiveDocument13 pagesRobust PBPK/PD-Based Model PredictivenhatvpNo ratings yet
- BMC Systems BiologyDocument25 pagesBMC Systems BiologyLateecka R KulkarniNo ratings yet
- Comparison of The Accuracy of The Hemocue Glucose Analyzer With The Yellow Springs Instrument Glucose Oxidase Analyzer, Particularly in HypoglycemiaDocument7 pagesComparison of The Accuracy of The Hemocue Glucose Analyzer With The Yellow Springs Instrument Glucose Oxidase Analyzer, Particularly in HypoglycemiaSeven NightNo ratings yet
- Comparison Between PID-Fuzzy and Numerical Methods Based On Linear Algebra Controllers For Glucose Control in Type 1 Diabetes TreatmentDocument7 pagesComparison Between PID-Fuzzy and Numerical Methods Based On Linear Algebra Controllers For Glucose Control in Type 1 Diabetes Treatmentkaveendra.rcitNo ratings yet
- Sensors: Glucose Sensing Neurons in The Ventromedial HypothalamusDocument24 pagesSensors: Glucose Sensing Neurons in The Ventromedial HypothalamusNorbert SzilágyiNo ratings yet
- Ijmsv 17 P 2998Document7 pagesIjmsv 17 P 2998Shivpartap SinghNo ratings yet
- Gluconeogenic SubstratesDocument11 pagesGluconeogenic SubstratesBrayam AguilarNo ratings yet
- Divya 13Document20 pagesDivya 13Divya NadarNo ratings yet
- Single-Cell Metabolic Profiling of Human Cytotoxic T Cells: ArticlesDocument19 pagesSingle-Cell Metabolic Profiling of Human Cytotoxic T Cells: ArticlesShivaprakash Jagalur MuttNo ratings yet
- Endokrin DMT2Document4 pagesEndokrin DMT2Ikrima Firda MaharaniNo ratings yet
- Alm037 01 02Document10 pagesAlm037 01 02MarcelliaNo ratings yet
- Pharmaceutics 11 00336Document17 pagesPharmaceutics 11 00336Tyas PardedeNo ratings yet
- Ajtr 0143528Document8 pagesAjtr 0143528Mudasir ElahiNo ratings yet
- Applicability Results of A Nonlinear Model-Based RDocument10 pagesApplicability Results of A Nonlinear Model-Based RfhamdiNo ratings yet
- Journal Pone 0248280 PDFDocument17 pagesJournal Pone 0248280 PDFHafis KafitNo ratings yet
- Nutrient Regulation of InsulinDocument16 pagesNutrient Regulation of InsulinNickolasMarllesNo ratings yet
- Modelo Matematico InsulinaDocument14 pagesModelo Matematico InsulinaBerenice Ibarra Dra ZucaritasNo ratings yet
- Physiology of Glucose Homeostasis and Insulin Therapy in Type 1 and Type 2 Diabetes (2012)Document15 pagesPhysiology of Glucose Homeostasis and Insulin Therapy in Type 1 and Type 2 Diabetes (2012)drheayNo ratings yet
- 9-A System Model of Oral Glucose AbsorptionDocument7 pages9-A System Model of Oral Glucose AbsorptionVitorDiegoNo ratings yet
- Theoretical Biology and Medical Modelling: A Discrete Single Delay Model For The Intra-Venous Glucose Tolerance TestDocument16 pagesTheoretical Biology and Medical Modelling: A Discrete Single Delay Model For The Intra-Venous Glucose Tolerance TestRocsana Teodora MăriuNo ratings yet
- Diagnosing Insulin Resistance by Simple Quantitative Methods in Subjects With Normal Glucose MetabolismDocument6 pagesDiagnosing Insulin Resistance by Simple Quantitative Methods in Subjects With Normal Glucose MetabolismKiaraliz Rivera RosaNo ratings yet
- Applicability Results of A Nonlinear Model-Based Robust Blood Glucose Control AlgorithmDocument9 pagesApplicability Results of A Nonlinear Model-Based Robust Blood Glucose Control AlgorithmCifha Rajesh SaldhanhaNo ratings yet
- Dgad 668Document10 pagesDgad 668Michael UNo ratings yet
- Medication-Free Management Oftype 2 Diabetesmellitus: Empirical and Modeling-Based Case StudyDocument25 pagesMedication-Free Management Oftype 2 Diabetesmellitus: Empirical and Modeling-Based Case StudyIJAR JOURNALNo ratings yet
- Plasma Malondialdehyde Level and Erythrocytes Catalase Activity in Patients With Type 2 Diabetes MellitusDocument14 pagesPlasma Malondialdehyde Level and Erythrocytes Catalase Activity in Patients With Type 2 Diabetes MellitusKyae Mhon HtweNo ratings yet
- Time-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverDocument16 pagesTime-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverChanachai PuckNo ratings yet
- Adiponectin - Journey From An Adipocyte SecretoryDocument9 pagesAdiponectin - Journey From An Adipocyte SecretorygiannidietNo ratings yet
- ABM Clinical Protocol #1: Guidelines For Blood Glucose Monitoring and Treatment of Hypoglycemia in Term and Late-Preterm Neonates, Revised 2014Document7 pagesABM Clinical Protocol #1: Guidelines For Blood Glucose Monitoring and Treatment of Hypoglycemia in Term and Late-Preterm Neonates, Revised 2014Gita KurniasariNo ratings yet
- Assessment of Model Predictive and Adaptive Glucose Contr - 2014 - IFAC ProceediDocument6 pagesAssessment of Model Predictive and Adaptive Glucose Contr - 2014 - IFAC ProceediNguyễn Văn TrungNo ratings yet
- Introductory Chapter MetabolomicsDocument15 pagesIntroductory Chapter Metabolomicsnadira noor hakimNo ratings yet
- Associations of Glucose Control with Insulin Sensitivity and Pancreatic β-Cell Responsiveness in Newly Presenting Type 2 DiabetesDocument6 pagesAssociations of Glucose Control with Insulin Sensitivity and Pancreatic β-Cell Responsiveness in Newly Presenting Type 2 DiabetesJoseph PositivoNo ratings yet
- Original Article Standardization of Visible Kinetic Assay For The Estimation of Plasma Glucose by Glucose-Oxidase and Peroxidase MethoDocument11 pagesOriginal Article Standardization of Visible Kinetic Assay For The Estimation of Plasma Glucose by Glucose-Oxidase and Peroxidase MethoVijendra KavatalkarNo ratings yet
- 2010 TCF7L2 Variant Rs7903146 Affects The Risk of Type 2 Diabetes by Modulating Incretin ActionDocument7 pages2010 TCF7L2 Variant Rs7903146 Affects The Risk of Type 2 Diabetes by Modulating Incretin ActionFiqih NurkholisNo ratings yet
- Estimating Insulin Sensitivity and Beta-Cell Function From The Oral Glucose Tolerance Test (Ha Et Al., 2024)Document47 pagesEstimating Insulin Sensitivity and Beta-Cell Function From The Oral Glucose Tolerance Test (Ha Et Al., 2024)Marcelo TrNo ratings yet
- A Mathematical Model of Glucose - Insulin Regulation Under The Influence of Externally Ingested Glucose (G-I-E Model)Document5 pagesA Mathematical Model of Glucose - Insulin Regulation Under The Influence of Externally Ingested Glucose (G-I-E Model)inventionjournalsNo ratings yet
- AGEs ZoteroDocument34 pagesAGEs ZoteroAngel OrtegaNo ratings yet
- Human Plasma ProteomeDocument16 pagesHuman Plasma ProteomeBRAULIO RIVERANo ratings yet
- Association of Coagulation Profile With Microvascular Complications and Glycemic Control in Type 2 Diabetes Mellitus - A Study ADocument1 pageAssociation of Coagulation Profile With Microvascular Complications and Glycemic Control in Type 2 Diabetes Mellitus - A Study Aseneh17198No ratings yet
- Gambaran Kadar Glukosa Darah Puasa Pada Mahasiswa Angkatan 2011 Fakultas Kedokteran Universitas Sam Ratulangi Dengan Indeks Massatubuh 18,5-22,9 KG/MDocument6 pagesGambaran Kadar Glukosa Darah Puasa Pada Mahasiswa Angkatan 2011 Fakultas Kedokteran Universitas Sam Ratulangi Dengan Indeks Massatubuh 18,5-22,9 KG/MbadrudtamamNo ratings yet
- Tests of Glycemia in Diabetes: D E. G, R R. L, R A. L, J I. M, D N, C M. P, D B. SDocument13 pagesTests of Glycemia in Diabetes: D E. G, R R. L, R A. L, J I. M, D N, C M. P, D B. Sfebriyani dyahNo ratings yet
- R49 Full PDFDocument14 pagesR49 Full PDFJuan Martin Perez GrilloNo ratings yet
- Continuous Glucose MonitoringFrom EverandContinuous Glucose MonitoringWeiping JiaNo ratings yet
- Lab09Document15 pagesLab09fhamdiNo ratings yet
- LabVIEW LINX and ArduinoDocument92 pagesLabVIEW LINX and ArduinofhamdiNo ratings yet
- 2-42-2-PBDocument12 pages2-42-2-PBfhamdiNo ratings yet
- (Studies in Systems, Decision and Control, 221) Zhenhua Wang, Yi Shen - Model-Based Fault Diagnosis_ Methods for State-Space Systems-Springer (2022)Document207 pages(Studies in Systems, Decision and Control, 221) Zhenhua Wang, Yi Shen - Model-Based Fault Diagnosis_ Methods for State-Space Systems-Springer (2022)fhamdiNo ratings yet
- Applicability Results of A Nonlinear Model-Based RDocument10 pagesApplicability Results of A Nonlinear Model-Based RfhamdiNo ratings yet
- Lesson3 DAQmxDocument30 pagesLesson3 DAQmxfhamdiNo ratings yet
- Hierarchical Control of Timed Discrete-Event SystemsDocument33 pagesHierarchical Control of Timed Discrete-Event SystemsfhamdiNo ratings yet
- MQ50389Document169 pagesMQ50389fhamdiNo ratings yet
- Testing Modularity of Local SupervisorsDocument7 pagesTesting Modularity of Local SupervisorsfhamdiNo ratings yet
- Zamanifekri 2009Document6 pagesZamanifekri 2009fhamdiNo ratings yet
- 1 s2.0 S2405896317315276 MainDocument7 pages1 s2.0 S2405896317315276 MainfhamdiNo ratings yet
- 1 ShaftEncoderDocument17 pages1 ShaftEncoderfhamdiNo ratings yet
- 1 s2.0 S0895717700000728 MainDocument14 pages1 s2.0 S0895717700000728 MainfhamdiNo ratings yet
- Crna School ResumeDocument7 pagesCrna School Resumehlizshggf100% (1)
- FEASIBILITY STUDIES (Final)Document42 pagesFEASIBILITY STUDIES (Final)Anuj IwarkarNo ratings yet
- Endocrine Disorders - AuriculotherapyDocument2 pagesEndocrine Disorders - AuriculotherapyCarissa Nichols100% (2)
- Ensayos Sobre Por Qué Quiero Ser EnfermeraDocument8 pagesEnsayos Sobre Por Qué Quiero Ser Enfermeraeblhhjhjf100% (2)
- Module 3 - Good Housekeeping and Material Handling and StorageDocument3 pagesModule 3 - Good Housekeeping and Material Handling and StoragevonsonNo ratings yet
- Perspective in Dentistry Reviewer (PH)Document3 pagesPerspective in Dentistry Reviewer (PH)Jas Jas100% (1)
- Located in Tualatin, Oregon: Amy's DaycareDocument14 pagesLocated in Tualatin, Oregon: Amy's DaycareAmy L. ZirkelbachNo ratings yet
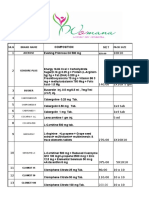
- SR.N Brand Name Pack Size AceroseDocument12 pagesSR.N Brand Name Pack Size AceroseRickChatterjeeNo ratings yet
- Inventaris OkDocument16 pagesInventaris OkheriiskandarNo ratings yet
- MedicalCheckUp - Physical Examination PDFDocument3 pagesMedicalCheckUp - Physical Examination PDFCielo Baez ArceNo ratings yet
- Seedling School of Law and GovernanceDocument14 pagesSeedling School of Law and GovernanceAnkit JindalNo ratings yet
- VAW-Brgy-Form NEWDocument4 pagesVAW-Brgy-Form NEWBarangay A TumamakNo ratings yet
- MSDS Waterplug SdsDocument6 pagesMSDS Waterplug Sdsmovie clipNo ratings yet
- RESD 515 Lecture 11 Restoration of Endodontically Treated Teeth - Dr. MunugaDocument68 pagesRESD 515 Lecture 11 Restoration of Endodontically Treated Teeth - Dr. Munugaali asiriNo ratings yet
- List of Welding Inspector (IWI)Document12 pagesList of Welding Inspector (IWI)soetrisno898No ratings yet
- Gsis VS CalumpianoDocument2 pagesGsis VS CalumpianoJohan King LeoricNo ratings yet
- Nationwide Population-Based Epidemiological Study of Myasthenia Gravis in TaiwanDocument6 pagesNationwide Population-Based Epidemiological Study of Myasthenia Gravis in TaiwanLissaberti AmaliahNo ratings yet
- White Paper Parameters and Species Exigo h400 - Wpe - 34071 1 PDFDocument12 pagesWhite Paper Parameters and Species Exigo h400 - Wpe - 34071 1 PDFОльга ДовженкоNo ratings yet
- Subject: of The of The F: Implementation CentralDocument1 pageSubject: of The of The F: Implementation CentralBhavagna SaiNo ratings yet
- 'Princess Mom' - The Glinner UpdateDocument11 pages'Princess Mom' - The Glinner UpdatemordidacampestreNo ratings yet
- Full Download pdf of Solution Manual for Design of Reinforced Concrete 10th by McCormac all chapterDocument61 pagesFull Download pdf of Solution Manual for Design of Reinforced Concrete 10th by McCormac all chapterdalbunntuku100% (3)
- Sleep Deprivation Thesis ProposalDocument61 pagesSleep Deprivation Thesis ProposalKimberly Reyes79% (33)
- Safety and Efficacy Therapy New CombinationDocument11 pagesSafety and Efficacy Therapy New CombinationFalisha Belvia KairinNo ratings yet
- Unit-4 Mental and Behavioral ProblemsDocument20 pagesUnit-4 Mental and Behavioral ProblemsZain Ul abidinNo ratings yet
- University of Rizal System Cainta Campus Ed1 Name: Chyryz Jewel D. Baldelomar Date: Nov. 5, 2020 PART 1 (50 PTS.)Document3 pagesUniversity of Rizal System Cainta Campus Ed1 Name: Chyryz Jewel D. Baldelomar Date: Nov. 5, 2020 PART 1 (50 PTS.)Chyryz Jewel BaldelomarNo ratings yet
- Standard Lift Plan ChecklistDocument9 pagesStandard Lift Plan ChecklistPablo Alejandro JrNo ratings yet




































































































Download as pdf or txt
You might also like
- Case Study Ectopic PregnancyDocument37 pagesCase Study Ectopic PregnancyJoule Peirre83% (6)
- Helix Installation Manual Rev 002Document112 pagesHelix Installation Manual Rev 002Edgar Mendoza100% (2)
- Market Research On Male Grooming IndustryDocument30 pagesMarket Research On Male Grooming IndustryMonalisa SethiNo ratings yet
- 4-The Impact of Body Image On Self-Esteem in AdolescentsDocument11 pages4-The Impact of Body Image On Self-Esteem in AdolescentsClinical and Counselling Psychology ReviewNo ratings yet
- From Metabolomics To FluxomicsDocument10 pagesFrom Metabolomics To FluxomicscamartinezriNo ratings yet
- RM ProtocolDocument4 pagesRM Protocolcifha diasNo ratings yet
- Palumbo 13Document13 pagesPalumbo 13Margarete Ap SantosNo ratings yet
- Transcriptomic and Proteomic Analysis of Potential Therapeutic Target Genes in The Liver of Metformin Treated Sprague Dawley Rats With Type 2 Diabetes Mellitusijmm-41!06!3327Document15 pagesTranscriptomic and Proteomic Analysis of Potential Therapeutic Target Genes in The Liver of Metformin Treated Sprague Dawley Rats With Type 2 Diabetes Mellitusijmm-41!06!3327ErickNo ratings yet
- 110 320 1 PB PDFDocument10 pages110 320 1 PB PDFMirna AisyahNo ratings yet
- 110 320 1 PB PDFDocument10 pages110 320 1 PB PDFMirna AisyahNo ratings yet
- Diabetes MellitusDocument17 pagesDiabetes MellitusIkekielNo ratings yet
- tmp22D3 TMPDocument9 pagestmp22D3 TMPFrontiersNo ratings yet
- Quasi-Model-Based Control of Type 1 Diabetes MelliDocument14 pagesQuasi-Model-Based Control of Type 1 Diabetes MellifhamdiNo ratings yet
- Simplified Mathematical Model of Glucose-Insulin SystemDocument12 pagesSimplified Mathematical Model of Glucose-Insulin SystemBrasoveanu GheorghitaNo ratings yet
- Else 2020 Conference 2Document7 pagesElse 2020 Conference 2Chestionar SanatateNo ratings yet
- ImplantDocument8 pagesImplantTabishur RahmanNo ratings yet
- Glucose Variability - FullDocument12 pagesGlucose Variability - FullAlina PopaNo ratings yet
- Research ArticleDocument8 pagesResearch ArticlebegumbahceciNo ratings yet
- A Phenomenological-Based Semi-Physical Model of The Kidneys and Its Role inDocument32 pagesA Phenomenological-Based Semi-Physical Model of The Kidneys and Its Role inronni bermudezNo ratings yet
- Metabolites 13 00222 v3Document12 pagesMetabolites 13 00222 v3Salva SVNo ratings yet
- Measurement of Glucose Homeostasis in VivoDocument10 pagesMeasurement of Glucose Homeostasis in Vivo19400668No ratings yet
- Thorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsDocument12 pagesThorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsgercampeNo ratings yet
- Robust PBPK/PD-Based Model PredictiveDocument13 pagesRobust PBPK/PD-Based Model PredictivenhatvpNo ratings yet
- BMC Systems BiologyDocument25 pagesBMC Systems BiologyLateecka R KulkarniNo ratings yet
- Comparison of The Accuracy of The Hemocue Glucose Analyzer With The Yellow Springs Instrument Glucose Oxidase Analyzer, Particularly in HypoglycemiaDocument7 pagesComparison of The Accuracy of The Hemocue Glucose Analyzer With The Yellow Springs Instrument Glucose Oxidase Analyzer, Particularly in HypoglycemiaSeven NightNo ratings yet
- Comparison Between PID-Fuzzy and Numerical Methods Based On Linear Algebra Controllers For Glucose Control in Type 1 Diabetes TreatmentDocument7 pagesComparison Between PID-Fuzzy and Numerical Methods Based On Linear Algebra Controllers For Glucose Control in Type 1 Diabetes Treatmentkaveendra.rcitNo ratings yet
- Sensors: Glucose Sensing Neurons in The Ventromedial HypothalamusDocument24 pagesSensors: Glucose Sensing Neurons in The Ventromedial HypothalamusNorbert SzilágyiNo ratings yet
- Ijmsv 17 P 2998Document7 pagesIjmsv 17 P 2998Shivpartap SinghNo ratings yet
- Gluconeogenic SubstratesDocument11 pagesGluconeogenic SubstratesBrayam AguilarNo ratings yet
- Divya 13Document20 pagesDivya 13Divya NadarNo ratings yet
- Single-Cell Metabolic Profiling of Human Cytotoxic T Cells: ArticlesDocument19 pagesSingle-Cell Metabolic Profiling of Human Cytotoxic T Cells: ArticlesShivaprakash Jagalur MuttNo ratings yet
- Endokrin DMT2Document4 pagesEndokrin DMT2Ikrima Firda MaharaniNo ratings yet
- Alm037 01 02Document10 pagesAlm037 01 02MarcelliaNo ratings yet
- Pharmaceutics 11 00336Document17 pagesPharmaceutics 11 00336Tyas PardedeNo ratings yet
- Ajtr 0143528Document8 pagesAjtr 0143528Mudasir ElahiNo ratings yet
- Applicability Results of A Nonlinear Model-Based RDocument10 pagesApplicability Results of A Nonlinear Model-Based RfhamdiNo ratings yet
- Journal Pone 0248280 PDFDocument17 pagesJournal Pone 0248280 PDFHafis KafitNo ratings yet
- Nutrient Regulation of InsulinDocument16 pagesNutrient Regulation of InsulinNickolasMarllesNo ratings yet
- Modelo Matematico InsulinaDocument14 pagesModelo Matematico InsulinaBerenice Ibarra Dra ZucaritasNo ratings yet
- Physiology of Glucose Homeostasis and Insulin Therapy in Type 1 and Type 2 Diabetes (2012)Document15 pagesPhysiology of Glucose Homeostasis and Insulin Therapy in Type 1 and Type 2 Diabetes (2012)drheayNo ratings yet
- 9-A System Model of Oral Glucose AbsorptionDocument7 pages9-A System Model of Oral Glucose AbsorptionVitorDiegoNo ratings yet
- Theoretical Biology and Medical Modelling: A Discrete Single Delay Model For The Intra-Venous Glucose Tolerance TestDocument16 pagesTheoretical Biology and Medical Modelling: A Discrete Single Delay Model For The Intra-Venous Glucose Tolerance TestRocsana Teodora MăriuNo ratings yet
- Diagnosing Insulin Resistance by Simple Quantitative Methods in Subjects With Normal Glucose MetabolismDocument6 pagesDiagnosing Insulin Resistance by Simple Quantitative Methods in Subjects With Normal Glucose MetabolismKiaraliz Rivera RosaNo ratings yet
- Applicability Results of A Nonlinear Model-Based Robust Blood Glucose Control AlgorithmDocument9 pagesApplicability Results of A Nonlinear Model-Based Robust Blood Glucose Control AlgorithmCifha Rajesh SaldhanhaNo ratings yet
- Dgad 668Document10 pagesDgad 668Michael UNo ratings yet
- Medication-Free Management Oftype 2 Diabetesmellitus: Empirical and Modeling-Based Case StudyDocument25 pagesMedication-Free Management Oftype 2 Diabetesmellitus: Empirical and Modeling-Based Case StudyIJAR JOURNALNo ratings yet
- Plasma Malondialdehyde Level and Erythrocytes Catalase Activity in Patients With Type 2 Diabetes MellitusDocument14 pagesPlasma Malondialdehyde Level and Erythrocytes Catalase Activity in Patients With Type 2 Diabetes MellitusKyae Mhon HtweNo ratings yet
- Time-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverDocument16 pagesTime-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverChanachai PuckNo ratings yet
- Adiponectin - Journey From An Adipocyte SecretoryDocument9 pagesAdiponectin - Journey From An Adipocyte SecretorygiannidietNo ratings yet
- ABM Clinical Protocol #1: Guidelines For Blood Glucose Monitoring and Treatment of Hypoglycemia in Term and Late-Preterm Neonates, Revised 2014Document7 pagesABM Clinical Protocol #1: Guidelines For Blood Glucose Monitoring and Treatment of Hypoglycemia in Term and Late-Preterm Neonates, Revised 2014Gita KurniasariNo ratings yet
- Assessment of Model Predictive and Adaptive Glucose Contr - 2014 - IFAC ProceediDocument6 pagesAssessment of Model Predictive and Adaptive Glucose Contr - 2014 - IFAC ProceediNguyễn Văn TrungNo ratings yet
- Introductory Chapter MetabolomicsDocument15 pagesIntroductory Chapter Metabolomicsnadira noor hakimNo ratings yet
- Associations of Glucose Control with Insulin Sensitivity and Pancreatic β-Cell Responsiveness in Newly Presenting Type 2 DiabetesDocument6 pagesAssociations of Glucose Control with Insulin Sensitivity and Pancreatic β-Cell Responsiveness in Newly Presenting Type 2 DiabetesJoseph PositivoNo ratings yet
- Original Article Standardization of Visible Kinetic Assay For The Estimation of Plasma Glucose by Glucose-Oxidase and Peroxidase MethoDocument11 pagesOriginal Article Standardization of Visible Kinetic Assay For The Estimation of Plasma Glucose by Glucose-Oxidase and Peroxidase MethoVijendra KavatalkarNo ratings yet
- 2010 TCF7L2 Variant Rs7903146 Affects The Risk of Type 2 Diabetes by Modulating Incretin ActionDocument7 pages2010 TCF7L2 Variant Rs7903146 Affects The Risk of Type 2 Diabetes by Modulating Incretin ActionFiqih NurkholisNo ratings yet
- Estimating Insulin Sensitivity and Beta-Cell Function From The Oral Glucose Tolerance Test (Ha Et Al., 2024)Document47 pagesEstimating Insulin Sensitivity and Beta-Cell Function From The Oral Glucose Tolerance Test (Ha Et Al., 2024)Marcelo TrNo ratings yet
- A Mathematical Model of Glucose - Insulin Regulation Under The Influence of Externally Ingested Glucose (G-I-E Model)Document5 pagesA Mathematical Model of Glucose - Insulin Regulation Under The Influence of Externally Ingested Glucose (G-I-E Model)inventionjournalsNo ratings yet
- AGEs ZoteroDocument34 pagesAGEs ZoteroAngel OrtegaNo ratings yet
- Human Plasma ProteomeDocument16 pagesHuman Plasma ProteomeBRAULIO RIVERANo ratings yet
- Association of Coagulation Profile With Microvascular Complications and Glycemic Control in Type 2 Diabetes Mellitus - A Study ADocument1 pageAssociation of Coagulation Profile With Microvascular Complications and Glycemic Control in Type 2 Diabetes Mellitus - A Study Aseneh17198No ratings yet
- Gambaran Kadar Glukosa Darah Puasa Pada Mahasiswa Angkatan 2011 Fakultas Kedokteran Universitas Sam Ratulangi Dengan Indeks Massatubuh 18,5-22,9 KG/MDocument6 pagesGambaran Kadar Glukosa Darah Puasa Pada Mahasiswa Angkatan 2011 Fakultas Kedokteran Universitas Sam Ratulangi Dengan Indeks Massatubuh 18,5-22,9 KG/MbadrudtamamNo ratings yet
- Tests of Glycemia in Diabetes: D E. G, R R. L, R A. L, J I. M, D N, C M. P, D B. SDocument13 pagesTests of Glycemia in Diabetes: D E. G, R R. L, R A. L, J I. M, D N, C M. P, D B. Sfebriyani dyahNo ratings yet
- R49 Full PDFDocument14 pagesR49 Full PDFJuan Martin Perez GrilloNo ratings yet
- Continuous Glucose MonitoringFrom EverandContinuous Glucose MonitoringWeiping JiaNo ratings yet
- Lab09Document15 pagesLab09fhamdiNo ratings yet
- LabVIEW LINX and ArduinoDocument92 pagesLabVIEW LINX and ArduinofhamdiNo ratings yet
- 2-42-2-PBDocument12 pages2-42-2-PBfhamdiNo ratings yet
- (Studies in Systems, Decision and Control, 221) Zhenhua Wang, Yi Shen - Model-Based Fault Diagnosis_ Methods for State-Space Systems-Springer (2022)Document207 pages(Studies in Systems, Decision and Control, 221) Zhenhua Wang, Yi Shen - Model-Based Fault Diagnosis_ Methods for State-Space Systems-Springer (2022)fhamdiNo ratings yet
- Applicability Results of A Nonlinear Model-Based RDocument10 pagesApplicability Results of A Nonlinear Model-Based RfhamdiNo ratings yet
- Lesson3 DAQmxDocument30 pagesLesson3 DAQmxfhamdiNo ratings yet
- Hierarchical Control of Timed Discrete-Event SystemsDocument33 pagesHierarchical Control of Timed Discrete-Event SystemsfhamdiNo ratings yet
- MQ50389Document169 pagesMQ50389fhamdiNo ratings yet
- Testing Modularity of Local SupervisorsDocument7 pagesTesting Modularity of Local SupervisorsfhamdiNo ratings yet
- Zamanifekri 2009Document6 pagesZamanifekri 2009fhamdiNo ratings yet
- 1 s2.0 S2405896317315276 MainDocument7 pages1 s2.0 S2405896317315276 MainfhamdiNo ratings yet
- 1 ShaftEncoderDocument17 pages1 ShaftEncoderfhamdiNo ratings yet
- 1 s2.0 S0895717700000728 MainDocument14 pages1 s2.0 S0895717700000728 MainfhamdiNo ratings yet
- Crna School ResumeDocument7 pagesCrna School Resumehlizshggf100% (1)
- FEASIBILITY STUDIES (Final)Document42 pagesFEASIBILITY STUDIES (Final)Anuj IwarkarNo ratings yet
- Endocrine Disorders - AuriculotherapyDocument2 pagesEndocrine Disorders - AuriculotherapyCarissa Nichols100% (2)
- Ensayos Sobre Por Qué Quiero Ser EnfermeraDocument8 pagesEnsayos Sobre Por Qué Quiero Ser Enfermeraeblhhjhjf100% (2)
- Module 3 - Good Housekeeping and Material Handling and StorageDocument3 pagesModule 3 - Good Housekeeping and Material Handling and StoragevonsonNo ratings yet
- Perspective in Dentistry Reviewer (PH)Document3 pagesPerspective in Dentistry Reviewer (PH)Jas Jas100% (1)
- Located in Tualatin, Oregon: Amy's DaycareDocument14 pagesLocated in Tualatin, Oregon: Amy's DaycareAmy L. ZirkelbachNo ratings yet
- SR.N Brand Name Pack Size AceroseDocument12 pagesSR.N Brand Name Pack Size AceroseRickChatterjeeNo ratings yet
- Inventaris OkDocument16 pagesInventaris OkheriiskandarNo ratings yet
- MedicalCheckUp - Physical Examination PDFDocument3 pagesMedicalCheckUp - Physical Examination PDFCielo Baez ArceNo ratings yet
- Seedling School of Law and GovernanceDocument14 pagesSeedling School of Law and GovernanceAnkit JindalNo ratings yet
- VAW-Brgy-Form NEWDocument4 pagesVAW-Brgy-Form NEWBarangay A TumamakNo ratings yet
- MSDS Waterplug SdsDocument6 pagesMSDS Waterplug Sdsmovie clipNo ratings yet
- RESD 515 Lecture 11 Restoration of Endodontically Treated Teeth - Dr. MunugaDocument68 pagesRESD 515 Lecture 11 Restoration of Endodontically Treated Teeth - Dr. Munugaali asiriNo ratings yet
- List of Welding Inspector (IWI)Document12 pagesList of Welding Inspector (IWI)soetrisno898No ratings yet
- Gsis VS CalumpianoDocument2 pagesGsis VS CalumpianoJohan King LeoricNo ratings yet
- Nationwide Population-Based Epidemiological Study of Myasthenia Gravis in TaiwanDocument6 pagesNationwide Population-Based Epidemiological Study of Myasthenia Gravis in TaiwanLissaberti AmaliahNo ratings yet
- White Paper Parameters and Species Exigo h400 - Wpe - 34071 1 PDFDocument12 pagesWhite Paper Parameters and Species Exigo h400 - Wpe - 34071 1 PDFОльга ДовженкоNo ratings yet
- Subject: of The of The F: Implementation CentralDocument1 pageSubject: of The of The F: Implementation CentralBhavagna SaiNo ratings yet
- 'Princess Mom' - The Glinner UpdateDocument11 pages'Princess Mom' - The Glinner UpdatemordidacampestreNo ratings yet
- Full Download pdf of Solution Manual for Design of Reinforced Concrete 10th by McCormac all chapterDocument61 pagesFull Download pdf of Solution Manual for Design of Reinforced Concrete 10th by McCormac all chapterdalbunntuku100% (3)
- Sleep Deprivation Thesis ProposalDocument61 pagesSleep Deprivation Thesis ProposalKimberly Reyes79% (33)
- Safety and Efficacy Therapy New CombinationDocument11 pagesSafety and Efficacy Therapy New CombinationFalisha Belvia KairinNo ratings yet
- Unit-4 Mental and Behavioral ProblemsDocument20 pagesUnit-4 Mental and Behavioral ProblemsZain Ul abidinNo ratings yet
- University of Rizal System Cainta Campus Ed1 Name: Chyryz Jewel D. Baldelomar Date: Nov. 5, 2020 PART 1 (50 PTS.)Document3 pagesUniversity of Rizal System Cainta Campus Ed1 Name: Chyryz Jewel D. Baldelomar Date: Nov. 5, 2020 PART 1 (50 PTS.)Chyryz Jewel BaldelomarNo ratings yet
- Standard Lift Plan ChecklistDocument9 pagesStandard Lift Plan ChecklistPablo Alejandro JrNo ratings yet