Download as pdf or txt
You might also like
- Grammar Tales Teaching GuideDocument124 pagesGrammar Tales Teaching GuideEdilberto Uribe98% (49)
- Bean Counters Teacher Hand-OutsDocument25 pagesBean Counters Teacher Hand-OutsJustin Henderson100% (1)
- 1-Dengue IgG & IgM - PO2709736085-377Document12 pages1-Dengue IgG & IgM - PO2709736085-377TV UNITNo ratings yet
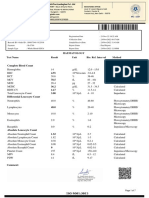
- 1-Complete Blood Count - PO1106326185-399Document8 pages1-Complete Blood Count - PO1106326185-399Arup KumarNo ratings yet
- Department of Hematology: Blood C/E (Complete, CBC)Document1 pageDepartment of Hematology: Blood C/E (Complete, CBC)M.TalhaNo ratings yet
- SuccessFactors Employee Central Practice QuestionsDocument11 pagesSuccessFactors Employee Central Practice Questionsrekha89757% (7)
- C 10Document344 pagesC 10Anonymous yxFeWtNo ratings yet
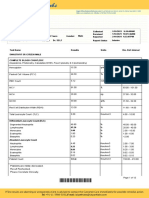
- Complete Haemogram Test Erythrocytes: No. Investigation Observed Value Unit Biological Ref. IntervalDocument6 pagesComplete Haemogram Test Erythrocytes: No. Investigation Observed Value Unit Biological Ref. IntervalAbeer AliNo ratings yet
- MR Rakesh Gupta 75030562024 04 19 06 43 14 761 6 0 1 582 133580154345478553Document11 pagesMR Rakesh Gupta 75030562024 04 19 06 43 14 761 6 0 1 582 133580154345478553Chaitali MantriNo ratings yet
- Shanti Devi 76868772024 05 17 09 50 05 962 6 0 1 114 133604084928234934 PDFDocument5 pagesShanti Devi 76868772024 05 17 09 50 05 962 6 0 1 114 133604084928234934 PDFdineshthakur9608826543No ratings yet
- MRS Pooja Kadam 67336292023 12 20 12 09 26 672 6 0 1 114 133475360100245541Document8 pagesMRS Pooja Kadam 67336292023 12 20 12 09 26 672 6 0 1 114 133475360100245541yogesh kadamNo ratings yet
- GD Wellness Monsoon Camp: Complete Haemogram Test ErythrocytesDocument10 pagesGD Wellness Monsoon Camp: Complete Haemogram Test ErythrocytesLucky BoffinNo ratings yet
- Complete Haemogram Test Erythrocytes: No. Investigation Observed Value Unit Biological Ref. IntervalDocument3 pagesComplete Haemogram Test Erythrocytes: No. Investigation Observed Value Unit Biological Ref. Intervalreetu priyaNo ratings yet
- Complete Haemogram Test Erythrocytes: SR - No Investigation Observed Value Reference Range UnitDocument3 pagesComplete Haemogram Test Erythrocytes: SR - No Investigation Observed Value Reference Range UnitAyush tours and TravelsNo ratings yet
- MR Prateek 60514302023 08 05 11 51 54 069 1 6 114 133357227964726067 PDFDocument7 pagesMR Prateek 60514302023 08 05 11 51 54 069 1 6 114 133357227964726067 PDFsuraj galbaleNo ratings yet
- Covid Well: Complete Haemogram Test ErythrocytesDocument14 pagesCovid Well: Complete Haemogram Test ErythrocytesUNIQUE DIAGNOSTICNo ratings yet
- Essential Body Checkup Package-1: Complete Haemogram Test ErythrocytesDocument10 pagesEssential Body Checkup Package-1: Complete Haemogram Test ErythrocytesLucky BoffinNo ratings yet
- Complete Haemogram Test Erythrocytes: SR - No Investigation Observed Value Reference Range UnitDocument9 pagesComplete Haemogram Test Erythrocytes: SR - No Investigation Observed Value Reference Range UnitLucky BoffinNo ratings yet
- Himani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDFDocument16 pagesHimani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDFONE SURE LABNo ratings yet
- Covid Well: Complete Haemogram Test ErythrocytesDocument5 pagesCovid Well: Complete Haemogram Test ErythrocytesUNIQUE DIAGNOSTICNo ratings yet
- Navneet Jain 56198722023 04 24 12 15 49 806 1 6 587 133268135734330208 PDFDocument14 pagesNavneet Jain 56198722023 04 24 12 15 49 806 1 6 587 133268135734330208 PDFONE SURE LABNo ratings yet
- Blood Chemistry Profile: Pt's Name: Piyush Patel Ref - By: Dr. Sandip ContractorDocument4 pagesBlood Chemistry Profile: Pt's Name: Piyush Patel Ref - By: Dr. Sandip ContractorPiyush PatelNo ratings yet
- Sikund Diagnostic CentreDocument3 pagesSikund Diagnostic CentreAnuja GairolaNo ratings yet
- Sangeeta Vishnio ReportsDocument13 pagesSangeeta Vishnio ReportsDigital WorldNo ratings yet
- GOURAB SAHOO-Male21 Years-77852Document2 pagesGOURAB SAHOO-Male21 Years-77852J. K. MuduliNo ratings yet
- Kidney FunctionDocument19 pagesKidney FunctionFarooq Bin MahfoozNo ratings yet
- PranyDocument4 pagesPranyदिव्य प्रताप सिंहNo ratings yet
- Raisuddin Saifi 55978562023 04 18 10 27 32 729 1 6 578 133263506543481990 PDFDocument9 pagesRaisuddin Saifi 55978562023 04 18 10 27 32 729 1 6 578 133263506543481990 PDFONE SURE LABNo ratings yet
- Report 3f90266bDocument18 pagesReport 3f90266bSK TacNo ratings yet
- L61 - FPSC Birla Farm Vill-Haripur Kalan, Birla Farm Rishikesh Raiwala Haridwar, Dehradun24920Document12 pagesL61 - FPSC Birla Farm Vill-Haripur Kalan, Birla Farm Rishikesh Raiwala Haridwar, Dehradun24920Lalit JoshiNo ratings yet
- Aashish Rakesh Pardeshi-Male22 Years-143943Document5 pagesAashish Rakesh Pardeshi-Male22 Years-143943goalone0202No ratings yet
- Report-63170102060 SHEELARANI LF055 19apr2017 140533Document1 pageReport-63170102060 SHEELARANI LF055 19apr2017 140533Sumit VermaNo ratings yet
- Report 0bd39992Document8 pagesReport 0bd39992NEETFIXNo ratings yet
- 4j4lr2qrnxjnrh1mo2u5c1weDocument3 pages4j4lr2qrnxjnrh1mo2u5c1weprateek siwachNo ratings yet
- Health ProfileDocument18 pagesHealth ProfileSahil HussainNo ratings yet
- Dinesh SainiDocument2 pagesDinesh Sainifadikex618No ratings yet
- Report ViewerDocument2 pagesReport Viewersufyan rasoolNo ratings yet
- Oxy Patho Sample ReportDocument12 pagesOxy Patho Sample ReportWycliffe AnshulNo ratings yet
- MR SONU SAINI S O RATTI RAM SAINI 25 04 2024 08 00 04 AMDocument4 pagesMR SONU SAINI S O RATTI RAM SAINI 25 04 2024 08 00 04 AMfadikex618No ratings yet
- Addfcfba 0eb4 11ef Ac47 7c1e520e223c HeaderDocument15 pagesAddfcfba 0eb4 11ef Ac47 7c1e520e223c Headerdakshchauhaunan.5No ratings yet
- Sacchi Dan andDocument2 pagesSacchi Dan andVINAYNo ratings yet
- Don't Know Love - 1004584Document14 pagesDon't Know Love - 1004584baapj39No ratings yet
- DownloadDocument3 pagesDownloadAnushkaNo ratings yet
- Ram Chandra Manwani 2902Document3 pagesRam Chandra Manwani 2902Satish JaisinghaniNo ratings yet
- Investigation Biological Reference Interval Units: ResultDocument4 pagesInvestigation Biological Reference Interval Units: Resultprateek bhatiaNo ratings yet
- ReportDocument1 pageReportnooruddinNo ratings yet
- Complete Blood PictureDocument4 pagesComplete Blood PictureMaged Ibrahim KandilNo ratings yet
- Narayan CH Dey-73Document2 pagesNarayan CH Dey-73Sanjoy DasNo ratings yet
- Laboratory Report: M.D. (Patho) M.D. (Patho) M.D. (Patho)Document2 pagesLaboratory Report: M.D. (Patho) M.D. (Patho) M.D. (Patho)Parth KaravadraNo ratings yet
- Hazarilal917 916 915 914 913 912 0Document5 pagesHazarilal917 916 915 914 913 912 0SHAKYA KuldeepNo ratings yet
- MadhavDocument1 pageMadhavmadhav maheshwariNo ratings yet
- Xymrxckhqt0hjns53qjdfvadDocument10 pagesXymrxckhqt0hjns53qjdfvadfeceni7791No ratings yet
- Honey CBC Bio Elisa RiadDocument3 pagesHoney CBC Bio Elisa RiadMd.Monjurul IslamNo ratings yet
- Medical PiyushDocument5 pagesMedical Piyushpiyush748499No ratings yet
- Kaushal867 866 865 864 863 862 0Document5 pagesKaushal867 866 865 864 863 862 0SHAKYA KuldeepNo ratings yet
- Haematology Test Name Result Unit Bio. Ref. Range MethodDocument3 pagesHaematology Test Name Result Unit Bio. Ref. Range MethodSaurabh Prakash DixitNo ratings yet
- Rama ReportDocument15 pagesRama ReportAnkush NayyarNo ratings yet
- Ram Gopal2Document4 pagesRam Gopal2SHAKYA KuldeepNo ratings yet
- L61 - FPSC Birla Farm Vill-Haripur Kalan, Birla Farm Rishikesh Raiwala Haridwar, Dehradun24920Document16 pagesL61 - FPSC Birla Farm Vill-Haripur Kalan, Birla Farm Rishikesh Raiwala Haridwar, Dehradun24920Lalit Joshi100% (1)
- BSC Research PaperDocument2 pagesBSC Research PaperaayushyadavmailsNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument2 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalVivek RadhakrishnanNo ratings yet
- Rajkumar HerDocument1 pageRajkumar HerRajkumar SontakkeNo ratings yet
- Prince (26793107 - )Document1 pagePrince (26793107 - )PrinceNo ratings yet
- Clinical Proteomics: From Diagnosis to TherapyFrom EverandClinical Proteomics: From Diagnosis to TherapyJennifer E. Van EykNo ratings yet
- Subaru - CHASSISDocument520 pagesSubaru - CHASSISIS52100% (1)
- Dark Energy and Dark MatterDocument26 pagesDark Energy and Dark MattersaphirehaelNo ratings yet
- Physics Education Thesis TopicsDocument4 pagesPhysics Education Thesis TopicsPaperWriterServicesCanada100% (2)
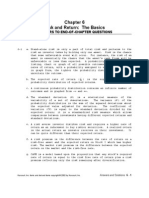
- Ch06 Solations Brigham 10th EDocument32 pagesCh06 Solations Brigham 10th ERafay HussainNo ratings yet
- Market Structure and Market PerformanceDocument22 pagesMarket Structure and Market PerformanceAishwarya SudhirNo ratings yet
- Fotona QX LeafletDocument2 pagesFotona QX Leafletmedhat fathyNo ratings yet
- Pediatric Vestibular Disorders PDFDocument10 pagesPediatric Vestibular Disorders PDFNati GallardoNo ratings yet
- Lecture 06Document30 pagesLecture 06Martis88No ratings yet
- 2009-11-05Document20 pages2009-11-05The University Daily KansanNo ratings yet
- Legislative Counsel's Digest: Section 1 of This Bill Authorizes A Person Who Is Not Under Arrest or in TheDocument9 pagesLegislative Counsel's Digest: Section 1 of This Bill Authorizes A Person Who Is Not Under Arrest or in TheFOX5 VegasNo ratings yet
- Sample Assignment 1-1Document20 pagesSample Assignment 1-1Nir IslamNo ratings yet
- Pond Based Tilapia Hatchery ManagementDocument50 pagesPond Based Tilapia Hatchery ManagementAlvin Javier PeranteNo ratings yet
- Catalog Copeland KCLDocument40 pagesCatalog Copeland KCLIsidro MendozaNo ratings yet
- Pnap 79Document6 pagesPnap 79Chan JoeNo ratings yet
- Panasonic hc-vx870 hc-vx878 hc-v770 hc-v777 Series SMDocument71 pagesPanasonic hc-vx870 hc-vx878 hc-v770 hc-v777 Series SMhector mirandaNo ratings yet
- S&s Valve Catalogue - Rev - 4Document23 pagesS&s Valve Catalogue - Rev - 4nonjinNo ratings yet
- Child 210 Collaborative Quest Team Project GuidelinesDocument2 pagesChild 210 Collaborative Quest Team Project GuidelinesDominique ArguellesNo ratings yet
- Continuous Beam Lab G4Document11 pagesContinuous Beam Lab G4Najmuddin Aliff67% (3)
- Reviewer in Pa 108Document14 pagesReviewer in Pa 108Madelyn OrfinadaNo ratings yet
- Philippines RegionsDocument5 pagesPhilippines RegionsKristine MercadoNo ratings yet
- Fruit Juice IndustryDocument11 pagesFruit Juice IndustryArlene GutierrezNo ratings yet
- Kalimat Simple Present Tense Aktif Kalimat Simple Past Tense AktifDocument2 pagesKalimat Simple Present Tense Aktif Kalimat Simple Past Tense AktifRestu PamujiNo ratings yet
- Strategies Towards Comprehensive Hemophilia Care Services in Uttar Pradesh" SGPGIMS, LucknowDocument4 pagesStrategies Towards Comprehensive Hemophilia Care Services in Uttar Pradesh" SGPGIMS, LucknowsalmanNo ratings yet
- MR SecGH Grp1 LeverAyushDocument12 pagesMR SecGH Grp1 LeverAyushSoumya HalderNo ratings yet
- SPWLA Log IntegrationDocument14 pagesSPWLA Log IntegrationpahlawankemalemanNo ratings yet
- Miscellaneous Measurements: and ControlsDocument50 pagesMiscellaneous Measurements: and ControlsJeje JungNo ratings yet