Download as pdf or txt
You might also like
- Kitchenbrigade 120821195157 Phpapp02Document25 pagesKitchenbrigade 120821195157 Phpapp02Conrado AreolaNo ratings yet
- Strategic Plan-4Document9 pagesStrategic Plan-4Bryan VillarezNo ratings yet
- Massive Transfusion - An Update For The Anesthesiologist 2017Document9 pagesMassive Transfusion - An Update For The Anesthesiologist 2017JOSENo ratings yet
- Meta 6 - Khizar - 2023Document11 pagesMeta 6 - Khizar - 2023matheus.verasNo ratings yet
- Efek HDDocument10 pagesEfek HDAdi SuciptoNo ratings yet
- JCM 12 06173Document20 pagesJCM 12 06173Taulant MukaNo ratings yet
- WarshawDocument11 pagesWarshawJuan RamirezNo ratings yet
- Nair Et Al. 2016 - Frequent Home Haemodialysis, A Review of The EvidenceDocument8 pagesNair Et Al. 2016 - Frequent Home Haemodialysis, A Review of The EvidenceShareDialysisNo ratings yet
- Conrad Et Al-2017-Journal of Hepato-Biliary-Pancreatic SciencesDocument14 pagesConrad Et Al-2017-Journal of Hepato-Biliary-Pancreatic SciencesAndra CiocanNo ratings yet
- Hepatic Steatosis and Fibrosis Non-Invasive AssessDocument19 pagesHepatic Steatosis and Fibrosis Non-Invasive Assessehsanulazim50buetNo ratings yet
- Biomedicines 10 01013Document15 pagesBiomedicines 10 01013Anshika yadavNo ratings yet
- HDX by Ronco 2017Document8 pagesHDX by Ronco 2017lizzaNo ratings yet
- Protective Mechanisms and Current Clinical EvidencDocument18 pagesProtective Mechanisms and Current Clinical EvidencCláudia SilvaNo ratings yet
- WJGS 8 376Document7 pagesWJGS 8 376Inamullah FurqanNo ratings yet
- PIIS1053077023003403Document12 pagesPIIS1053077023003403lxluizNo ratings yet
- Breakthroughs in Hepatology JhepatDocument2 pagesBreakthroughs in Hepatology JhepatCláudia SilvaNo ratings yet
- Clinical Transplantation - 2022 - Alconchel - Are Short Term Complications Associated With Poor Allograft and PatientDocument14 pagesClinical Transplantation - 2022 - Alconchel - Are Short Term Complications Associated With Poor Allograft and PatientlucianapcariusNo ratings yet
- Neoadjuvant Chemotherapy Vs Upfront Surgery For Gastric Signet Ring Cell Carcinoma A Retrospective, Propensity Score-Matched StudyDocument11 pagesNeoadjuvant Chemotherapy Vs Upfront Surgery For Gastric Signet Ring Cell Carcinoma A Retrospective, Propensity Score-Matched StudyLITTLESWEETKILLERNo ratings yet
- Clinicopathological Study of Varicose Veins (Descriptive Study)Document10 pagesClinicopathological Study of Varicose Veins (Descriptive Study)Vlad DraculaNo ratings yet
- DOACs in Cirrhotic Patients With Portal Vein Thrombosis - The EvidenceDocument15 pagesDOACs in Cirrhotic Patients With Portal Vein Thrombosis - The EvidencelabertoNo ratings yet
- Joacp 35 29Document6 pagesJoacp 35 29kenjiNo ratings yet
- Hemodialysis Internal Jugular Vein Versus Subclavian Vein Catheters: Complications, Patients' Comfort, Tolerance and Cost-EffectivenessDocument5 pagesHemodialysis Internal Jugular Vein Versus Subclavian Vein Catheters: Complications, Patients' Comfort, Tolerance and Cost-EffectivenessYolanda IrawatiNo ratings yet
- AnemiaDocument7 pagesAnemiaAttilio Del RossoNo ratings yet
- Changing Trends in Liver Transplantation .14Document14 pagesChanging Trends in Liver Transplantation .14Pablo Henrique Alves TelesNo ratings yet
- 2016 - Long-Term Donor Outcomes After Pure Laparoscopic Versus Open Living Donor NephrectomyDocument7 pages2016 - Long-Term Donor Outcomes After Pure Laparoscopic Versus Open Living Donor Nephrectomynarutota181No ratings yet
- A Review of Liver Transplantation For The Dentist and Guidelines For Dental ManagementDocument7 pagesA Review of Liver Transplantation For The Dentist and Guidelines For Dental ManagementLujainNo ratings yet
- Revisiting Donor Risk Over Two Decades of Single-Center Experience: More Attention On The Impact of OverweightDocument8 pagesRevisiting Donor Risk Over Two Decades of Single-Center Experience: More Attention On The Impact of Overweightyerich septaNo ratings yet
- Clinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialDocument8 pagesClinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialfaundraNo ratings yet
- Timing of Initiation of Renal-ReplacementDocument12 pagesTiming of Initiation of Renal-Replacementchamwick4567No ratings yet
- Pi is 0085253820309054Document11 pagesPi is 0085253820309054Chavalit ChotruangnapaNo ratings yet
- World Journal of Gastroenterology, Hepatology and Endoscopy: Article InformationDocument4 pagesWorld Journal of Gastroenterology, Hepatology and Endoscopy: Article Informationscience world publishingNo ratings yet
- MKW 070Document6 pagesMKW 070Dashhh RamirezNo ratings yet
- Wjgo 14 1199Document12 pagesWjgo 14 1199juan uribeNo ratings yet
- Resuscitation Fluid Composition in Acute Kidney Injury in Critical IllnessDocument2 pagesResuscitation Fluid Composition in Acute Kidney Injury in Critical IllnessDe Frede EditoreNo ratings yet
- Posthepatectomy Liver Failure: A Definition and Grading by The International Study Group of Liver Surgery (ISGLS)Document12 pagesPosthepatectomy Liver Failure: A Definition and Grading by The International Study Group of Liver Surgery (ISGLS)drsubramanianNo ratings yet
- s43678 021 00126 7Document5 pagess43678 021 00126 7Hugo EspinozaNo ratings yet
- Thesis On Chronic Kidney DiseaseDocument5 pagesThesis On Chronic Kidney Diseasebrendahigginsarlington100% (2)
- 10 Carcinomatoza PeritonealaDocument9 pages10 Carcinomatoza PeritonealaGabriela MilitaruNo ratings yet
- Acute Allograft Rejection in Liver Transplant Recipients: Incidence, Risk Factors, Treatment Success, and Impact On Graft FailureDocument12 pagesAcute Allograft Rejection in Liver Transplant Recipients: Incidence, Risk Factors, Treatment Success, and Impact On Graft Failurenathalialusman98No ratings yet
- DRC Kdigo CanadenseDocument29 pagesDRC Kdigo CanadensePaulo RigaudNo ratings yet
- Recommendations For The Use of Tolvaptan in AutosoDocument13 pagesRecommendations For The Use of Tolvaptan in AutosoBeth EnriquezNo ratings yet
- BaliJAnaesthesiol5126-1251569 032835Document7 pagesBaliJAnaesthesiol5126-1251569 032835Yunita Kristiana DewiNo ratings yet
- 1 s2.0 S105122762300105X MainDocument11 pages1 s2.0 S105122762300105X MainJulia KhaerunisaNo ratings yet
- Locoregional Treatments Obsolete For Patients With Cancer With Liver MetastasesDocument18 pagesLocoregional Treatments Obsolete For Patients With Cancer With Liver MetastasesDR. SUMANTRA RAYNo ratings yet
- Cancer Res-2011-Kawada-0008-5472.CAN-10-3277Document16 pagesCancer Res-2011-Kawada-0008-5472.CAN-10-3277Nolie Lovarya HarukaNo ratings yet
- Donor Management and Organ Preservation Transplant - International 2016 974-984Document11 pagesDonor Management and Organ Preservation Transplant - International 2016 974-984Marisol Gallego DuqueNo ratings yet
- 10.1007@s11897 019 00432 3Document7 pages10.1007@s11897 019 00432 3diogofc123No ratings yet
- New England Journal Medicine: The ofDocument14 pagesNew England Journal Medicine: The ofFajar PramaduNo ratings yet
- Fluid Management During Kidney TransplantationDocument8 pagesFluid Management During Kidney Transplantationgiancarlor368No ratings yet
- Radiology & Medical ImagingDocument6 pagesRadiology & Medical ImagingRizka Ramadhani AbrarNo ratings yet
- KDIGO Onconeph PT 1 Kidney Impairment and Solid Organ CancerDocument12 pagesKDIGO Onconeph PT 1 Kidney Impairment and Solid Organ CancerMaría MartínezNo ratings yet
- Criteria For Continuous Kidney Replacement Therapy Cessation in ICU PatientsDocument9 pagesCriteria For Continuous Kidney Replacement Therapy Cessation in ICU PatientszeravoneNo ratings yet
- Application of Various Surgical Techniques in Liver TransplantDocument12 pagesApplication of Various Surgical Techniques in Liver TransplantPaula AlmeidaNo ratings yet
- Uncontrolled Donation After Circulatory Death CompDocument9 pagesUncontrolled Donation After Circulatory Death CompKaffal TwoNo ratings yet
- Surgery of The Liver Pancreas and Biliary Tract (Dragged) 79Document17 pagesSurgery of The Liver Pancreas and Biliary Tract (Dragged) 79Nguyen Hai NamNo ratings yet
- Fish OilDocument18 pagesFish OilninukNo ratings yet
- ACO Peripro 2016Document10 pagesACO Peripro 2016Philippe Bocanegra FernándezNo ratings yet
- Surgery: SciencedirectDocument6 pagesSurgery: SciencedirectabrarkhanmdcmNo ratings yet
- Renal Cell Carcinoma A Case Series With Integrative Treatment 2329 6771 S1 002Document5 pagesRenal Cell Carcinoma A Case Series With Integrative Treatment 2329 6771 S1 002VanroNo ratings yet
- Hagedorn 2019Document10 pagesHagedorn 2019Cinthya Añazco RomeroNo ratings yet
- Long-Term Outcomes of Hepatitis B Virus-Related Cirrhosis Treated With Nucleos (T) Ide AnalogsDocument10 pagesLong-Term Outcomes of Hepatitis B Virus-Related Cirrhosis Treated With Nucleos (T) Ide AnalogsZulfiana NabilaNo ratings yet
- Critical Care for Potential Liver Transplant CandidatesFrom EverandCritical Care for Potential Liver Transplant CandidatesDmitri BezinoverNo ratings yet
- Sword and Sorcery 5eDocument5 pagesSword and Sorcery 5eConstantine PaleologusNo ratings yet
- Waterfront Boundaries For Grants of Public Crown Lands - MNR - E000074 - 2001Document3 pagesWaterfront Boundaries For Grants of Public Crown Lands - MNR - E000074 - 2001Sen HuNo ratings yet
- IBA Gas Field QuestionsDocument19 pagesIBA Gas Field Questionssazzadmunna5950% (1)
- Undergraduate Scholarships Application FormDocument3 pagesUndergraduate Scholarships Application FormAbdul Rehman ShejwalkarNo ratings yet
- Primemotiontraining Beeptest GuideDocument6 pagesPrimemotiontraining Beeptest GuideCristian NechitaNo ratings yet
- MIP 2021 (Budget Proposal)Document215 pagesMIP 2021 (Budget Proposal)Yanny ManggugubatNo ratings yet
- A Study of Factors Affecting Travel Decision Making of TouristsDocument10 pagesA Study of Factors Affecting Travel Decision Making of TouristsAmmarah Rajput ParhiarNo ratings yet
- Instruments NotesDocument116 pagesInstruments Notesprithvih4No ratings yet
- MPKDocument15 pagesMPKghaliyahalmiraNo ratings yet
- Metropolis 3 EdgesDocument12 pagesMetropolis 3 Edgesapi-264020285No ratings yet
- $ROW9KSXDocument18 pages$ROW9KSXRoberto SangregorioNo ratings yet
- Unit 1 - Introduction & Number Theory: Dr.S.Kalaivani Assistant Professor/ Dept. of CSE IrttDocument87 pagesUnit 1 - Introduction & Number Theory: Dr.S.Kalaivani Assistant Professor/ Dept. of CSE IrttRishikaa RamNo ratings yet
- Bahasa Inggris Kelas 5Document2 pagesBahasa Inggris Kelas 5Bimbeldec Depok100% (1)
- Test Bank For e Commerce 2019 Business Technology and Society 15th by LaudonDocument21 pagesTest Bank For e Commerce 2019 Business Technology and Society 15th by LaudonCecil Johnson100% (42)
- Fly & Drive Albania-UpdatedDocument5 pagesFly & Drive Albania-UpdatedBarbara CsécseiNo ratings yet
- OTC Asia 2024 Conference PreviewDocument20 pagesOTC Asia 2024 Conference PreviewAmmirul AzmanNo ratings yet
- Chapter 1 - History of NeuropsychologyDocument29 pagesChapter 1 - History of Neuropsychologymacue96No ratings yet
- Lloyd P. Gerson, PlotinusDocument9 pagesLloyd P. Gerson, PlotinusPrendasNo ratings yet
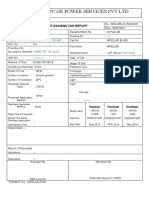
- NTPC Ge Power Services PVT LTD: Liquid Penetrant Examination ReportDocument2 pagesNTPC Ge Power Services PVT LTD: Liquid Penetrant Examination ReportBalkishan DyavanapellyNo ratings yet
- Mastermind 2 Unit 1 Grammar and Vocabulary Test ADocument7 pagesMastermind 2 Unit 1 Grammar and Vocabulary Test ARolando Guzman Martinez100% (1)
- Dissertation Binding DallasDocument8 pagesDissertation Binding DallasINeedSomeoneToWriteMyPaperOlathe100% (1)
- Chap002 2019 Fall Assignment 2Document6 pagesChap002 2019 Fall Assignment 2Taranom BakhtiaryNo ratings yet
- Teklehaimanot Abreham Job Application Letter: To: Heineken Breweries Share Company Dear Recruitment Manager!Document2 pagesTeklehaimanot Abreham Job Application Letter: To: Heineken Breweries Share Company Dear Recruitment Manager!Curios cornerNo ratings yet
- BABOK - Techniques by KADocument1 pageBABOK - Techniques by KABenhar Masahod BLM-VLOGNo ratings yet
- South Dakota State Treasurer Unclaimed Property: Claim FormDocument2 pagesSouth Dakota State Treasurer Unclaimed Property: Claim FormMiguel Paz100% (1)
- Survey of Philippine Literature in English: Shepherdville CollegeDocument9 pagesSurvey of Philippine Literature in English: Shepherdville CollegeMary Rose GuerreroNo ratings yet
- Conservative Management of Talon's Cusp-A Case ReportDocument22 pagesConservative Management of Talon's Cusp-A Case ReportHarees Shabir100% (1)
- Capital and RevenueDocument20 pagesCapital and RevenueDr Sarbesh Mishra100% (1)