Download as pdf or txt
You might also like
- Leslie Feinberg - Drag King Dreams-Carroll & Graf Publishers (2006)Document324 pagesLeslie Feinberg - Drag King Dreams-Carroll & Graf Publishers (2006)ce100% (3)
- Geothermal Energy Poster 2Document1 pageGeothermal Energy Poster 2api-298575301100% (2)
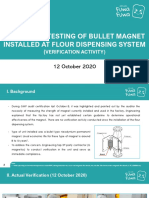
- Induction Testing of Bullet Magnet Installed at Flour Dispensing SystemDocument5 pagesInduction Testing of Bullet Magnet Installed at Flour Dispensing SystemMark Anthony Centeno100% (1)
- Barangay Nutrition Scholar Monthly AccomplishmentDocument7 pagesBarangay Nutrition Scholar Monthly AccomplishmentDianka Glory Cenabre Edrozo75% (4)
- Food Defense PlanDocument11 pagesFood Defense Planshyamalababu100% (3)
- Epidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionDocument8 pagesEpidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionshaheershayanqaziNo ratings yet
- Pulmonary Hypertension Is Prevalent in Catheter and Arterio-Venous Access HemodialysisDocument6 pagesPulmonary Hypertension Is Prevalent in Catheter and Arterio-Venous Access HemodialysisMichelle FernandoNo ratings yet
- Dr. Esti-Diagnostic Value of Combined FVC%DLCO% and Echocardiography in Connective Tissue Disorder Associated Pulmonary HypertensionDocument7 pagesDr. Esti-Diagnostic Value of Combined FVC%DLCO% and Echocardiography in Connective Tissue Disorder Associated Pulmonary Hypertension9wkpf2crrxNo ratings yet
- Jurnal 8Document10 pagesJurnal 8OziNo ratings yet
- JCVTR 6 35Document7 pagesJCVTR 6 35christ_cruzerNo ratings yet
- Indian Journal of Nephrology Home: Download PDFDocument8 pagesIndian Journal of Nephrology Home: Download PDFDr. Jatin GargNo ratings yet
- Diagnosis of Pulmonary HypertensionDocument12 pagesDiagnosis of Pulmonary HypertensionFaridaFaradillaPutryCherewetNo ratings yet
- Prognostic Factors in Pulmonary Arterial Hypertension: Literature ReviewDocument5 pagesPrognostic Factors in Pulmonary Arterial Hypertension: Literature Reviewhuda riyambodoNo ratings yet
- European J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificDocument11 pagesEuropean J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificVlad RusuNo ratings yet
- 1 s2.0 S0147956318301237Document5 pages1 s2.0 S0147956318301237nadaNo ratings yet
- The Prognostic Role of Anemia in Heart Failure PatientsDocument7 pagesThe Prognostic Role of Anemia in Heart Failure PatientsAnonymous rprdjdFMNzNo ratings yet
- Clinica Chimica Acta: T. Omland, H. Røsjø, E. Giannitsis, S. AgewallDocument7 pagesClinica Chimica Acta: T. Omland, H. Røsjø, E. Giannitsis, S. AgewalllilisNo ratings yet
- Hipertension Pulmonar PeditriaDocument8 pagesHipertension Pulmonar PeditriajesusgonzalezapNo ratings yet
- Accepted Manuscript: The American Journal of CardiologyDocument22 pagesAccepted Manuscript: The American Journal of CardiologyAlamgirNo ratings yet
- Life 11 01429Document14 pagesLife 11 01429Genesis PerezNo ratings yet
- Meghan E.Document11 pagesMeghan E.Dr. Jatin GargNo ratings yet
- Atm 09 20 1587Document14 pagesAtm 09 20 1587Wina Pertiwi 2003113414No ratings yet
- Ehu 090Document9 pagesEhu 090Tatiana CumbicosNo ratings yet
- Exercise HTP ArtDocument10 pagesExercise HTP ArtDiana CarstairsNo ratings yet
- Optimized Combination of Circulating Biomarkers AsDocument8 pagesOptimized Combination of Circulating Biomarkers AsAndreea MoalesNo ratings yet
- Hipertensi PulmonalDocument5 pagesHipertensi PulmonalSteven RichardNo ratings yet
- Clinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With HeartDocument13 pagesClinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With Heartrizkiyah prabawantiNo ratings yet
- Evaluation and Management of Chronic Thromboembolic Pulmonary HypertensionDocument21 pagesEvaluation and Management of Chronic Thromboembolic Pulmonary HypertensionAndrés MontalvoNo ratings yet
- FCVM 09 876755Document8 pagesFCVM 09 876755Faradiba MaricarNo ratings yet
- CCRPM 2011 001 PDFDocument5 pagesCCRPM 2011 001 PDFAlexandria Firdaus Al-farisyNo ratings yet
- Vallabhajosyula 2016Document10 pagesVallabhajosyula 2016Arick Frendi AndriyanNo ratings yet
- Embolia Pulmonar SubmasivaDocument27 pagesEmbolia Pulmonar SubmasivaLuis Fernando Morales JuradoNo ratings yet
- Euro J of Neurology - 2023 - Kincl - Parkinson S Disease Cardiovascular Symptoms A New Complex Functional and StructuralDocument9 pagesEuro J of Neurology - 2023 - Kincl - Parkinson S Disease Cardiovascular Symptoms A New Complex Functional and StructuralIvan MihailovicNo ratings yet
- Chest Julio 2022 Hipertension Pulm en ILDDocument11 pagesChest Julio 2022 Hipertension Pulm en ILDnoeliaNo ratings yet
- Pulmonary Hypertension: Annals of Internal MedicinetDocument16 pagesPulmonary Hypertension: Annals of Internal MedicinetAlicia TGNo ratings yet
- 449 FullDocument6 pages449 Fullwael aboelmagdNo ratings yet
- Art Enfermedad Renal CronicaDocument8 pagesArt Enfermedad Renal CronicaLisset FernandezNo ratings yet
- Postdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityDocument6 pagesPostdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityLaura PutriNo ratings yet
- Hta (G4)Document9 pagesHta (G4)Juan LeonNo ratings yet
- Elevated Troponin I Levels But Not Low Grade Chronic Inflammation Is Associated With Cardiac-Specific Mortality in Stable Hemodialysis PatientsDocument15 pagesElevated Troponin I Levels But Not Low Grade Chronic Inflammation Is Associated With Cardiac-Specific Mortality in Stable Hemodialysis PatientswongCherryBoundNo ratings yet
- Err 0099 2020Document12 pagesErr 0099 2020Faradiba MaricarNo ratings yet
- Armstrong 2017 Diabetic Foot Ulcers and Their RecurrenceDocument11 pagesArmstrong 2017 Diabetic Foot Ulcers and Their Recurrencefebyan yohanesNo ratings yet
- PE and CHFDocument9 pagesPE and CHFKu Li ChengNo ratings yet
- Stephen Alerhand What Echocardiographic FindingsDocument13 pagesStephen Alerhand What Echocardiographic Findingsไกรสร เต็งNo ratings yet
- Burden of Heart Failure Patients in A Tertiary Level Cardiac HospitalDocument6 pagesBurden of Heart Failure Patients in A Tertiary Level Cardiac HospitalHasan Pallab MarufNo ratings yet
- Pulmonary HypertensionDocument13 pagesPulmonary HypertensionأنيسNo ratings yet
- Copd and AdhfDocument9 pagesCopd and Adhfmaryelle conejarNo ratings yet
- Prognostic Significance of Diastolic Dysfunction With Multiple Comorbidities in Heart Failure PatientsDocument11 pagesPrognostic Significance of Diastolic Dysfunction With Multiple Comorbidities in Heart Failure PatientsDefriyan RamziNo ratings yet
- HTA Resistente 2015 JAMADocument11 pagesHTA Resistente 2015 JAMAgustavo reyesNo ratings yet
- 1314-Article Text-2323-3-10-20190705Document7 pages1314-Article Text-2323-3-10-20190705VennyNo ratings yet
- Heart Volume Issue 2017 (Doi 10.1136 - Heartjnl-2017-312112) Ruwald, Martin H - Syncope andDocument3 pagesHeart Volume Issue 2017 (Doi 10.1136 - Heartjnl-2017-312112) Ruwald, Martin H - Syncope andZauzaNo ratings yet
- Erp 17 0071Document14 pagesErp 17 0071Jamir PastranaNo ratings yet
- Effect of Nocturnal Oxygen Therapy On Electrocardiographic Changes Among Patients With Congestive Heart FailureDocument3 pagesEffect of Nocturnal Oxygen Therapy On Electrocardiographic Changes Among Patients With Congestive Heart FailureNurAfifahNo ratings yet
- 10 16899-jcm 853237-1486847Document5 pages10 16899-jcm 853237-1486847rdelgado3No ratings yet
- The Long-Term Effects of Arteriovenous Fistula Creation On The Development of Pulmonary Hypertension in Hemodialysis PatientsDocument5 pagesThe Long-Term Effects of Arteriovenous Fistula Creation On The Development of Pulmonary Hypertension in Hemodialysis PatientsSaskiaaNo ratings yet
- Pulmonary Hypertension in COPD: Hypoxic VasoconstrictionDocument5 pagesPulmonary Hypertension in COPD: Hypoxic VasoconstrictionRazvan PredaNo ratings yet
- Pleural Effusions From Congestive Heart Failure: Jose M. Porcel, M.D., F.C.C.P., F.A.C.PDocument9 pagesPleural Effusions From Congestive Heart Failure: Jose M. Porcel, M.D., F.C.C.P., F.A.C.PDaniil KorzačNo ratings yet
- 1 s2.0 S000287032200093X MainDocument11 pages1 s2.0 S000287032200093X Mainwoldekidansamuel299No ratings yet
- Prevalence and Prognosis of Atrial Fibrillation in A HypertensiveDocument8 pagesPrevalence and Prognosis of Atrial Fibrillation in A HypertensiveSyadzwina Putri salsabilaNo ratings yet
- Hemorrhagic Stroke in Chronic Dialysis PatientsDocument8 pagesHemorrhagic Stroke in Chronic Dialysis PatientsJeffry HaryantoNo ratings yet
- Hipertrofia VD en HTADocument8 pagesHipertrofia VD en HTAgustavo reyesNo ratings yet
- Misra 2012Document7 pagesMisra 2012Carlos RiquelmeNo ratings yet
- Pulmonary Hypertension Mediastinal FibrosisDocument10 pagesPulmonary Hypertension Mediastinal FibrosisAndreiSefNo ratings yet
- Articulo Test DiagnosticoDocument7 pagesArticulo Test DiagnosticoDante Montiel AndradeNo ratings yet
- Clinical Cases in Chronic Thromboembolic Pulmonary HypertensionFrom EverandClinical Cases in Chronic Thromboembolic Pulmonary HypertensionWilliam R. AugerNo ratings yet
- 7119 32468 1 PBDocument16 pages7119 32468 1 PBnadaNo ratings yet
- Deswart 2019Document8 pagesDeswart 2019nadaNo ratings yet
- Morphologic Changes in Circulating Blood Cells of Covid-19 PatientsDocument8 pagesMorphologic Changes in Circulating Blood Cells of Covid-19 PatientsnadaNo ratings yet
- Jurnal Hema EvaDocument8 pagesJurnal Hema EvanadaNo ratings yet
- JBMR Plus - 2019 - Tauer - Osteogenesis Imperfecta New Perspectives From Clinical and Translational ResearchDocument10 pagesJBMR Plus - 2019 - Tauer - Osteogenesis Imperfecta New Perspectives From Clinical and Translational ResearchnadaNo ratings yet
- Jurnal IntropDocument4 pagesJurnal IntropnadaNo ratings yet
- LeukoeritroblastikDocument2 pagesLeukoeritroblastiknadaNo ratings yet
- 1 s2.0 S193665741830253X MainDocument10 pages1 s2.0 S193665741830253X MainnadaNo ratings yet
- Jadaon - 2011 - Epidemiology of Activated Protein C Resistance and Factor V Leiden Mutation in The Mediterranean RegionDocument11 pagesJadaon - 2011 - Epidemiology of Activated Protein C Resistance and Factor V Leiden Mutation in The Mediterranean RegionnadaNo ratings yet
- Botero Et Al. - 2017 - Diagnostic Testing Approaches For Activated Protein C Resistance and Factor V LeidenA Comparison of InstitutionalDocument7 pagesBotero Et Al. - 2017 - Diagnostic Testing Approaches For Activated Protein C Resistance and Factor V LeidenA Comparison of InstitutionalnadaNo ratings yet
- 1 s2.0 S0006497120687596 MainDocument5 pages1 s2.0 S0006497120687596 MainnadaNo ratings yet
- 1 s2.0 S0014579305003066 MainDocument7 pages1 s2.0 S0014579305003066 MainnadaNo ratings yet
- RisCo Firme Nou Infiintate 20190429Document127 pagesRisCo Firme Nou Infiintate 20190429Gazeta de MâineNo ratings yet
- Suzumar Boat Engine PackagesDocument7 pagesSuzumar Boat Engine PackagesmarkoNo ratings yet
- Cost of The DietDocument68 pagesCost of The DietSomao JoeNo ratings yet
- RA For Assessment For Lifting OperationsDocument19 pagesRA For Assessment For Lifting OperationsMohamedSaidNo ratings yet
- Gobi ManchurianDocument3 pagesGobi ManchurianPriya JuligantiNo ratings yet
- Diagnostic Fault Codes: Quick Reference GuideDocument2 pagesDiagnostic Fault Codes: Quick Reference GuideJavier VillelaNo ratings yet
- UKA Athletics Coach Induction Pack v2 Jan 2013Document36 pagesUKA Athletics Coach Induction Pack v2 Jan 2013gpitbullNo ratings yet
- Indira Gandhi National Widow Pension SchemeDocument3 pagesIndira Gandhi National Widow Pension SchemeNavinkumar RohitNo ratings yet
- Chemsheets KS3 040 Density 2Document2 pagesChemsheets KS3 040 Density 2PopDV-SquaredNo ratings yet
- The Effects of Electrical Muscle Stimulation Ems Towards Male Skeletal Muscle MassDocument10 pagesThe Effects of Electrical Muscle Stimulation Ems Towards Male Skeletal Muscle MassAnonymous N0vLeRxNo ratings yet
- Refractory: Zoning of Kilns and Brick SelectionDocument26 pagesRefractory: Zoning of Kilns and Brick Selectionrupesh soni100% (2)
- JBL Boombox 2+-V1 3Document31 pagesJBL Boombox 2+-V1 3Gilson Pereira100% (3)
- 2022 Fuenzalida Et Al 2022 New Records OfgigantolaelapswolffsohniDocument10 pages2022 Fuenzalida Et Al 2022 New Records OfgigantolaelapswolffsohniCarlos LandaetaNo ratings yet
- Chapter 6 Food Handlers Safety HygieneDocument20 pagesChapter 6 Food Handlers Safety HygieneIrish MalabananNo ratings yet
- Msds Heksana - 2 PDFDocument6 pagesMsds Heksana - 2 PDFGelisaNo ratings yet
- Planned ParenthoodDocument2 pagesPlanned ParenthoodChylon BudagherNo ratings yet
- Managing People - AssignmentDocument10 pagesManaging People - AssignmentayeshaNo ratings yet
- TYPHOIDDocument13 pagesTYPHOIDnaceyjj33No ratings yet
- Mandibulectomy PDFDocument4 pagesMandibulectomy PDFrekabiNo ratings yet
- Far Eastern Polytechnic College: Republic of The Philippines Region Iv-A Calabarzon City Schools Division of DasmariñasDocument2 pagesFar Eastern Polytechnic College: Republic of The Philippines Region Iv-A Calabarzon City Schools Division of DasmariñasJed CahinusayanNo ratings yet
- Solomon Islands Position PaperDocument2 pagesSolomon Islands Position PaperAJ Ammons0% (1)
- NIM: 2440007043 Nama: Ni Putu Young Yenyuo A Mata Kuliah: Accounting For Business Dosen: Herlin Tundjung SetijaningsihDocument5 pagesNIM: 2440007043 Nama: Ni Putu Young Yenyuo A Mata Kuliah: Accounting For Business Dosen: Herlin Tundjung SetijaningsihiyeNo ratings yet
- Gerby - RAHA CaresDocument4 pagesGerby - RAHA CaresGerard CariñoNo ratings yet
- Valuing The Suitable Agro-Industrial Wastes For Cultivation of P. Platypus and P. EousDocument4 pagesValuing The Suitable Agro-Industrial Wastes For Cultivation of P. Platypus and P. EousDinesh Babu PugalenthiNo ratings yet
- 1st and 2nd Assignment of PDDDocument2 pages1st and 2nd Assignment of PDDYash Bhardwaj FitnessNo ratings yet