Download as pdf or txt
You might also like
- Clinical Pharmacokinetics Concepts and ApplicationsDocument616 pagesClinical Pharmacokinetics Concepts and Applicationsstarscientist100% (14)
- Accupressure Points Chart PDFDocument20 pagesAccupressure Points Chart PDFshule1100% (2)
- A Time-Series Study of The Treatment of Panic DisorderDocument21 pagesA Time-Series Study of The Treatment of Panic Disordermetramor8745No ratings yet
- Cannabidiol en PsicosisDocument10 pagesCannabidiol en PsicosissiralkNo ratings yet
- Zhou 2020Document8 pagesZhou 2020Rosalía PattyNo ratings yet
- Cuijpers Et Al., (2021)Document11 pagesCuijpers Et Al., (2021)Jonathan PitreNo ratings yet
- Cardiometabolic Risk in Patients With First Episode of - 2022 - Neuroscience ApDocument1 pageCardiometabolic Risk in Patients With First Episode of - 2022 - Neuroscience AploloasbNo ratings yet
- 2.psilocybin-Assisted Therapy For Depression A Systematic Review and Dose-Response Meta-Analysis of Human StudiesDocument16 pages2.psilocybin-Assisted Therapy For Depression A Systematic Review and Dose-Response Meta-Analysis of Human StudiesMarcos MouraNo ratings yet
- Metaanaliz 2Document17 pagesMetaanaliz 2alef666No ratings yet
- Cannabidiol (CBD) As A Novel Treatment in The Early Phases of PsychosisDocument12 pagesCannabidiol (CBD) As A Novel Treatment in The Early Phases of PsychosisMarcela CordeiroNo ratings yet
- E Cacy of Modern Antipsychotics in Placebo-Controlled Trials in Bipolar Depression: A Meta-AnalysisDocument10 pagesE Cacy of Modern Antipsychotics in Placebo-Controlled Trials in Bipolar Depression: A Meta-AnalysisRisda AprilianiNo ratings yet
- Guidelines Anxiety RevisionDocument65 pagesGuidelines Anxiety Revisionscabrera_scribdNo ratings yet
- Pi Is 2215036616303789Document11 pagesPi Is 2215036616303789U of T MedicineNo ratings yet
- We Therell 2009Document10 pagesWe Therell 2009Oslo SaputraNo ratings yet
- Background: Lancet Psychiatry 2017Document11 pagesBackground: Lancet Psychiatry 2017Manya DhuparNo ratings yet
- The Role of CBT in Relapse Prevention of SchizophreniaDocument2 pagesThe Role of CBT in Relapse Prevention of SchizophreniaKorn IbraNo ratings yet
- Psychosis EssayDocument6 pagesPsychosis EssayDavid RobinsonNo ratings yet
- Incremental Cost-Effectiveness of Combines Therapy Vs Medication Anly For Youth With Selective Serotonin Reuptake Inhibitor Resistant DepressionDocument10 pagesIncremental Cost-Effectiveness of Combines Therapy Vs Medication Anly For Youth With Selective Serotonin Reuptake Inhibitor Resistant DepressionFerx Fernando PachecoNo ratings yet
- Precision Medicine in Alcohol Dependence A Controlled Trial Testing Pharmacotherapy Response Among Reward and Relief Drinking PhenotypesDocument9 pagesPrecision Medicine in Alcohol Dependence A Controlled Trial Testing Pharmacotherapy Response Among Reward and Relief Drinking Phenotypes陳弘儒No ratings yet
- Ttos Depresion MayorDocument11 pagesTtos Depresion MayorSusana Pérez ReyesNo ratings yet
- On Predicting Improvement and Relapse in Generalized Anxiety Disorder Following PsychotherapyDocument19 pagesOn Predicting Improvement and Relapse in Generalized Anxiety Disorder Following PsychotherapyElizaIancuNo ratings yet
- Perfeccionismo Ap y TocDocument15 pagesPerfeccionismo Ap y TocMiriam JaraNo ratings yet
- Hasler 2015Document32 pagesHasler 2015Seplou7iNo ratings yet
- Artículo Grupo 3Document11 pagesArtículo Grupo 3pepeluchovelezquezadaNo ratings yet
- Fpsyg 10 02741Document10 pagesFpsyg 10 02741Carlos S.Z.No ratings yet
- Psychedelic Therapy and Cancer AK2Document7 pagesPsychedelic Therapy and Cancer AK2William SkeidNo ratings yet
- JURNAL 2 Augmentation Strategies For Treatment-Resistant Anxiety Disorders A Systematic Review and Meta-Analysis-dikonversiDocument15 pagesJURNAL 2 Augmentation Strategies For Treatment-Resistant Anxiety Disorders A Systematic Review and Meta-Analysis-dikonversiNixal KurniawanNo ratings yet
- (25599283 - Journal of Psychedelic Studies) Psychedelic-Assisted Psychotherapy For Depression - How Dire Is The Need - How Could We Do ItDocument5 pages(25599283 - Journal of Psychedelic Studies) Psychedelic-Assisted Psychotherapy For Depression - How Dire Is The Need - How Could We Do ItLetíciaNo ratings yet
- May 09 Journals (Mostly) : 63 AbstractsDocument14 pagesMay 09 Journals (Mostly) : 63 AbstractssunkissedchiffonNo ratings yet
- Trastorno Bipolar PolifarmaciaDocument10 pagesTrastorno Bipolar PolifarmaciaFederico AlzugarayNo ratings yet
- Efficacy For Treatment Anxiety DisordersDocument10 pagesEfficacy For Treatment Anxiety DisordersAnderson GaldinoNo ratings yet
- Interventions in ADHD A Comparative Review of Stimulant Medications and Behavioral TherapiesDocument5 pagesInterventions in ADHD A Comparative Review of Stimulant Medications and Behavioral Therapiestitikkitti06No ratings yet
- Evidence-Based Practice PaperDocument16 pagesEvidence-Based Practice Paperapi-599394340No ratings yet
- Management of Generalized Anxiety Disorder in Primary Care - Identifying The Challenges and Unmet Needs PDFDocument21 pagesManagement of Generalized Anxiety Disorder in Primary Care - Identifying The Challenges and Unmet Needs PDFSilviaNo ratings yet
- 2017 GumleyDocument8 pages2017 GumleySandraNo ratings yet
- Psychopharmacological Options For Adult Patients WDocument2 pagesPsychopharmacological Options For Adult Patients WViviana DuarteNo ratings yet
- Greden2019 - OriginalDocument9 pagesGreden2019 - Originalاحمد صباح مالكNo ratings yet
- Acm 2009 0376Document10 pagesAcm 2009 0376Dr Tanu GogoiNo ratings yet
- Effectiveness of Videoconference-Delivered Cognitive Behavioral Therapy For Adults With Psychiatric Disorders: Systematic and Meta-Analytic ReviewDocument16 pagesEffectiveness of Videoconference-Delivered Cognitive Behavioral Therapy For Adults With Psychiatric Disorders: Systematic and Meta-Analytic ReviewlaiaNo ratings yet
- Realising The Mass Public Benefit of Evidence-Based Psychological Therapies The IAPT ProgramDocument31 pagesRealising The Mass Public Benefit of Evidence-Based Psychological Therapies The IAPT ProgramBeaNo ratings yet
- Psychopharmacological Treatment in BorderlineDocument8 pagesPsychopharmacological Treatment in BorderlineAndres MartinezNo ratings yet
- Brady 2015Document15 pagesBrady 2015alfredoibcNo ratings yet
- Efects of Mindfulness Based Therapy For Cancer PatientsDocument15 pagesEfects of Mindfulness Based Therapy For Cancer Patientsm01.abousalehNo ratings yet
- 213 2023 Article 6399Document11 pages213 2023 Article 6399rpzrz1No ratings yet
- Chamomile - Stress - Anxiety - Clinical - Meta AnalysisDocument12 pagesChamomile - Stress - Anxiety - Clinical - Meta Analysisadip royNo ratings yet
- Effect of Probiotics On Depressive Symptoms A Meta-Analysis of HumanDocument12 pagesEffect of Probiotics On Depressive Symptoms A Meta-Analysis of Humandanielson1986No ratings yet
- 2022 de VriesDocument8 pages2022 de Vriesmvillar15_247536468No ratings yet
- J Eurpsy 2007 03 002Document11 pagesJ Eurpsy 2007 03 002xhdrv7nvdrNo ratings yet
- ST Fo Chronic AnxietyDocument9 pagesST Fo Chronic AnxietyGabriel SilvaNo ratings yet
- Jurnal DepresiDocument15 pagesJurnal DepresiDesi PratiwiNo ratings yet
- Managing Antidepressant Discontinuation A Systematic ReviewDocument9 pagesManaging Antidepressant Discontinuation A Systematic ReviewAlejandro Arquillos ÁlvarezNo ratings yet
- Complementary Therapies in Medicine: Matthew Krouwel, Amanda Farley, Sheila Greenfield, Tariq Ismail, Kate JollyDocument9 pagesComplementary Therapies in Medicine: Matthew Krouwel, Amanda Farley, Sheila Greenfield, Tariq Ismail, Kate JollyPhilippe MirasNo ratings yet
- Edited By: Dr. Javaid Akhtar, MCPS, FCPS, Head Of: Search StrategyDocument3 pagesEdited By: Dr. Javaid Akhtar, MCPS, FCPS, Head Of: Search StrategyKaram Ali ShahNo ratings yet
- Positive Psychology For OvercoDocument20 pagesPositive Psychology For OvercoMichaelPaulLojaCasaNo ratings yet
- Psychedelic-Assisted Psychotherapy: A Paradigm Shift in Psychiatric Research and DevelopmentDocument11 pagesPsychedelic-Assisted Psychotherapy: A Paradigm Shift in Psychiatric Research and DevelopmentIago LôboNo ratings yet
- 1 s2.0 S0165032723009357 MainDocument7 pages1 s2.0 S0165032723009357 MainjuanNo ratings yet
- Ketamine NNTDocument8 pagesKetamine NNTBrent AllieNo ratings yet
- Špela PDFDocument11 pagesŠpela PDFŠpela MiroševičNo ratings yet
- Comparison of Clinical Significance of Cognitive-Behavioral Therapy and Psychodynamic Therapy For Major Depressive DisorderDocument8 pagesComparison of Clinical Significance of Cognitive-Behavioral Therapy and Psychodynamic Therapy For Major Depressive DisorderAnanda Amanda cintaNo ratings yet
- Cognitive Behavioral Therapy For Medication-Resistant Psychosis A Metanalytic ReviewDocument7 pagesCognitive Behavioral Therapy For Medication-Resistant Psychosis A Metanalytic Reviewjenny082600No ratings yet
- Integrative Headache Medicine: An Evidence-Based Guide for CliniciansFrom EverandIntegrative Headache Medicine: An Evidence-Based Guide for CliniciansLauren R. NatbonyNo ratings yet
- Mardi J. Horowitz - Adult Personality Growth in Psychotherapy-Cambridge University Press (2016)Document151 pagesMardi J. Horowitz - Adult Personality Growth in Psychotherapy-Cambridge University Press (2016)bssNo ratings yet
- Riccio 2017Document8 pagesRiccio 2017bssNo ratings yet
- Brown 2014Document21 pagesBrown 2014bssNo ratings yet
- Allott Et Al-2016-Brain and BehaviorDocument13 pagesAllott Et Al-2016-Brain and BehaviorbssNo ratings yet
- Traditional CCD FillableDocument1 pageTraditional CCD FillablebssNo ratings yet
- Clinical Applications of The General Ability IndexDocument34 pagesClinical Applications of The General Ability IndexbssNo ratings yet
- Case Write Up Template 3 1 8Document4 pagesCase Write Up Template 3 1 8bssNo ratings yet
- Work Sample Guide Master Level-CTRS-RDocument18 pagesWork Sample Guide Master Level-CTRS-RbssNo ratings yet
- Work Sample Guide Level 1-CTRS-RDocument19 pagesWork Sample Guide Level 1-CTRS-RbssNo ratings yet
- Work Sample Guide MASTER LEVELDocument15 pagesWork Sample Guide MASTER LEVELbssNo ratings yet
- Ecological Validity of A Quantitative ClassificatiDocument11 pagesEcological Validity of A Quantitative ClassificatibssNo ratings yet
- Mapping Established Psychopathology Scales Onto The Hierarchical Taxonomy of Psychopathology (Hitop)Document19 pagesMapping Established Psychopathology Scales Onto The Hierarchical Taxonomy of Psychopathology (Hitop)bssNo ratings yet
- Faraone 2006Document7 pagesFaraone 2006bssNo ratings yet
- Bleecker 2007Document9 pagesBleecker 2007bssNo ratings yet
- CAARMS Portugues BrazilDocument44 pagesCAARMS Portugues BrazilbssNo ratings yet
- Pms User Guide Additional VariablesDocument26 pagesPms User Guide Additional VariablesbssNo ratings yet
- FARMACODocument13 pagesFARMACOAndreea CroitoruNo ratings yet
- Materi Penting ApotekerDocument4 pagesMateri Penting ApotekernabilarahmanNo ratings yet
- Obat TB SetahunDocument65 pagesObat TB SetahunRani ZafiraNo ratings yet
- Perbandingan Efektifitas Tramadol 1,5 MG/KGBB Iv Dengan Ketorolak 30 MG Iv Terhadap Tingkat Nyeri Pasca Operasi Seksio SesareaDocument11 pagesPerbandingan Efektifitas Tramadol 1,5 MG/KGBB Iv Dengan Ketorolak 30 MG Iv Terhadap Tingkat Nyeri Pasca Operasi Seksio Sesareairvan rahmanNo ratings yet
- Recaida Lla BFM 2002Document151 pagesRecaida Lla BFM 2002Milber Enrique Fuentes rada100% (1)
- Comparison of Antipyretic Efficacy of Intravenous (IV) Acetaminophen Versus Oral (PO) Acetaminophen in The Management of Fever in ChildrenDocument4 pagesComparison of Antipyretic Efficacy of Intravenous (IV) Acetaminophen Versus Oral (PO) Acetaminophen in The Management of Fever in Childrenayu kottenNo ratings yet
- What Is Oxycontin? How Is Oxycontin Abused?: Street Terms For OxycontinDocument2 pagesWhat Is Oxycontin? How Is Oxycontin Abused?: Street Terms For Oxycontinlosangeles100% (2)
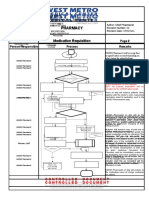
- Pharmacy Pharmacy: Medication Requisition Medication RequisitionDocument1 pagePharmacy Pharmacy: Medication Requisition Medication RequisitionSharie Grace ImlanNo ratings yet
- Basic Life SupportDocument35 pagesBasic Life SupportIndra RamdhaniNo ratings yet
- 5400-Article Text-7860-1-10-20161212Document4 pages5400-Article Text-7860-1-10-20161212Van DaoNo ratings yet
- 急救藥物泡法Document3 pages急救藥物泡法Edward KaoNo ratings yet
- Cool Wipes: Q1. Annual Cost of Serving Entire Nation Using Existing Plant at ChicagoDocument28 pagesCool Wipes: Q1. Annual Cost of Serving Entire Nation Using Existing Plant at ChicagoPankhuri Singhal0% (1)
- ADMET PK/TK and Drug Metabolism - Training Course Pharma Research and DevelopmentDocument3 pagesADMET PK/TK and Drug Metabolism - Training Course Pharma Research and DevelopmentCristina HoltzNo ratings yet
- Understanding Immunomodulatory DrugsDocument4 pagesUnderstanding Immunomodulatory DrugsMark Russel Sean LealNo ratings yet
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument4 pagesPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- Canagliflozin 300mgDocument6 pagesCanagliflozin 300mgMd. Abdur RahmanNo ratings yet
- Daftar Obat KemoterapiDocument3 pagesDaftar Obat KemoterapiCharles Nong MakingNo ratings yet
- 04 - 02 - Curriculum Design of Med Chem-I - IV SEM-2Document3 pages04 - 02 - Curriculum Design of Med Chem-I - IV SEM-2Tamu100% (1)
- Metric System ConversionsDocument1 pageMetric System Conversionsashee09No ratings yet
- PEDIATRIC Medication Side Effect Information Sheet TestDocument2 pagesPEDIATRIC Medication Side Effect Information Sheet TestAndreaDuboisNo ratings yet
- Art Dolor GeriátricoDocument9 pagesArt Dolor GeriátricoarrlyNo ratings yet
- Decreased Warfarin Effect After Initiation of High-Protein, Low-Carbohydrate DietsDocument5 pagesDecreased Warfarin Effect After Initiation of High-Protein, Low-Carbohydrate DietsDinaNo ratings yet
- Focus Pharmacology Essentials Health Professionals 3rd Moini Test BankDocument8 pagesFocus Pharmacology Essentials Health Professionals 3rd Moini Test BankRaadqqqNo ratings yet
- Comparison of Efficacy of Mulligan MWM With Maitland Mobilization Along With Conventional Therapy in The Patients of Knee OsteoarthritisDocument100 pagesComparison of Efficacy of Mulligan MWM With Maitland Mobilization Along With Conventional Therapy in The Patients of Knee OsteoarthritisHina QaisarNo ratings yet
- Acne TreatmentDocument2 pagesAcne TreatmentBps Azizah CangkringanNo ratings yet
- Pharmacology - Antibiotics Flash CardsDocument20 pagesPharmacology - Antibiotics Flash CardsJamil100% (2)
- Pharmacology For Nurses A Pathophysiologic Approach 5th Edition Adams Urban Holland 013425516X Solution ManualDocument10 pagesPharmacology For Nurses A Pathophysiologic Approach 5th Edition Adams Urban Holland 013425516X Solution Manualcarrie96% (27)
- Community Pharmacists Attitudes Toward Dispensing Errors at Community Pharmacy Setting in Central Saudi ArabiaDocument8 pagesCommunity Pharmacists Attitudes Toward Dispensing Errors at Community Pharmacy Setting in Central Saudi ArabiaNicoleta CheptanariNo ratings yet