Download as pdf or txt
You might also like
- Dr. Karen's Stress Relief Brain Balancing ProtocolDocument4 pagesDr. Karen's Stress Relief Brain Balancing ProtocolKaren Kan, MD100% (2)
- A Second-Generation Dendritic Cell Cancer Vaccine Preparing To ShineDocument19 pagesA Second-Generation Dendritic Cell Cancer Vaccine Preparing To Shinebiggercapital100% (5)
- Benign Prostatic Hyperplasia Concept MapDocument1 pageBenign Prostatic Hyperplasia Concept MapJason A. AdoyoganNo ratings yet
- Merritt Hawkins Physician To Population RatiosDocument2 pagesMerritt Hawkins Physician To Population RatiosCandra Lia PahdariesaNo ratings yet
- First AidDocument68 pagesFirst AidJanet Escosura Espinosa MadayagNo ratings yet
- MDX 444Document7 pagesMDX 444T HoranNo ratings yet
- MEK Inhibitors in Combination With Immune Checkpoint Inhibition: Should We Be Chasing Colorectal Cancer or The KRAS Mutant CancerDocument2 pagesMEK Inhibitors in Combination With Immune Checkpoint Inhibition: Should We Be Chasing Colorectal Cancer or The KRAS Mutant CancerPeertechz Publications Inc.No ratings yet
- Review Article Prostate ImmunotherapyDocument24 pagesReview Article Prostate ImmunotherapyMohammed AlabdullahNo ratings yet
- Immunotherapy For Head and Neck CancerDocument21 pagesImmunotherapy For Head and Neck CancerLuane SenaNo ratings yet
- Rycan 2021200134Document6 pagesRycan 2021200134Sakkuru Yeyen LiviaNo ratings yet
- Adoptive Transfer of Natural Killer Cells in Combination With Chemotherapy Improves Outcomes of Patients With Locally Advanced Colon Carcinoma.Document15 pagesAdoptive Transfer of Natural Killer Cells in Combination With Chemotherapy Improves Outcomes of Patients With Locally Advanced Colon Carcinoma.Andrew ChenNo ratings yet
- Colorectal Cancer Immune Infiltrates - Significance in Patient Prognosis andDocument13 pagesColorectal Cancer Immune Infiltrates - Significance in Patient Prognosis andOvamelia JulioNo ratings yet
- Pharmaceutics 14 01630Document27 pagesPharmaceutics 14 01630H. MD Ebr100% (1)
- Ipilimumab For Patients With Relapse After Allogeneic TransplantationDocument11 pagesIpilimumab For Patients With Relapse After Allogeneic TransplantationMhmd KorosNo ratings yet
- Advances in Cancer Immunotherapy 2019 - Latest TrendsDocument21 pagesAdvances in Cancer Immunotherapy 2019 - Latest TrendsSWAGATIKA CHANDANo ratings yet
- Current Status and Future Directions of Cancer ImmunotherapyDocument7 pagesCurrent Status and Future Directions of Cancer ImmunotherapyDesire EstevesNo ratings yet
- Biomedicines 12 00669Document15 pagesBiomedicines 12 00669jamel-shamsNo ratings yet
- iRECIST: How To Do It: Review Open AccessDocument7 pagesiRECIST: How To Do It: Review Open AccessNguyenthanh DuongNo ratings yet
- Cancers 14 02775Document22 pagesCancers 14 02775SiscaNo ratings yet
- Anticancer Activity of Phyllanthus Niruri Linn Extract in Colorectal Cancer Patients A Phase II Clinical TrialDocument5 pagesAnticancer Activity of Phyllanthus Niruri Linn Extract in Colorectal Cancer Patients A Phase II Clinical TrialAndi SaputraNo ratings yet
- Imunoterapi SNLC 3Document7 pagesImunoterapi SNLC 3aulidaweliNo ratings yet
- 2015 EN Clinical Trial of DC Combined With Chemo Against Metastatic Prostate CancerDocument14 pages2015 EN Clinical Trial of DC Combined With Chemo Against Metastatic Prostate CancerKhaliElYamaniNo ratings yet
- SinopsisDocument7 pagesSinopsisbee yournitaNo ratings yet
- Pembrolizumab in MSI-H DMMR Advanced Colorectal Cancer A New Standard of CareDocument3 pagesPembrolizumab in MSI-H DMMR Advanced Colorectal Cancer A New Standard of CareasdffdsaNo ratings yet
- Nature News and Views 2Document2 pagesNature News and Views 2Andi WeiNo ratings yet
- The Role of Automated Cytometry in The New Era of Cancer Immunotherapy (Review)Document7 pagesThe Role of Automated Cytometry in The New Era of Cancer Immunotherapy (Review)Andrea SbranaNo ratings yet
- Pancreatic CancerDocument9 pagesPancreatic Cancernski2104No ratings yet
- 2023 Monteleone Tagerted Therapy of IL34 As A Prmosing Approach To Overcome Cancer ResistanceDocument12 pages2023 Monteleone Tagerted Therapy of IL34 As A Prmosing Approach To Overcome Cancer Resistancephilippe.lacroix38490No ratings yet
- ScienceDocument1 pageScienceQuique TinocoNo ratings yet
- Pembrolizumab For Advanced Cervical Cancer Safety and EfficacyDocument9 pagesPembrolizumab For Advanced Cervical Cancer Safety and EfficacyluizaNo ratings yet
- Cancer Treatment Reviews: SciencedirectDocument10 pagesCancer Treatment Reviews: Sciencedirectrudy sanabriaNo ratings yet
- Biomedicines 06 00014 v2Document11 pagesBiomedicines 06 00014 v2yihuiNo ratings yet
- Prevalence of p53 Mutation in Serous Carcinoma Ovary and Its Predictive Value For Response To Platinum-Based ChemotherapyDocument6 pagesPrevalence of p53 Mutation in Serous Carcinoma Ovary and Its Predictive Value For Response To Platinum-Based ChemotherapyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Novel Diagnostic and Predictive Biomarkers in Pancreatic AdenocarcinomaDocument14 pagesNovel Diagnostic and Predictive Biomarkers in Pancreatic AdenocarcinomaChavdarNo ratings yet
- JCM 11 02277Document26 pagesJCM 11 02277prashantb07.2409No ratings yet
- Extracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deDocument55 pagesExtracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deAirin LeonieNo ratings yet
- 10 1016@j Ucl 2020 07 009Document13 pages10 1016@j Ucl 2020 07 009Posgrado CirugiaNo ratings yet
- Comprehensive Precision Medicine Study Protocol On The Heterogeneity of Taiwanese Breast Cancer PatientsDocument14 pagesComprehensive Precision Medicine Study Protocol On The Heterogeneity of Taiwanese Breast Cancer Patients郭竹瑩No ratings yet
- Jco 2015 64 8931Document10 pagesJco 2015 64 8931Kamila MuyasarahNo ratings yet
- Heymach-2022-Design and Rationale For A Phase1Document5 pagesHeymach-2022-Design and Rationale For A Phase1Luca BertolacciniNo ratings yet
- Cancers: /PD-L1 Targeting in Breast Cancer: The FirstDocument25 pagesCancers: /PD-L1 Targeting in Breast Cancer: The Firstrafiqa banoNo ratings yet
- Nihms 958907Document17 pagesNihms 958907Camilly CampanharoNo ratings yet
- Kanker TumorDocument11 pagesKanker TumorRENTI NOVITANo ratings yet
- An Expanding Role For Immunotherapy in Colorectal CancerDocument10 pagesAn Expanding Role For Immunotherapy in Colorectal CancercollianairaNo ratings yet
- Challenges in Diagnosis and Management of NeutropeDocument15 pagesChallenges in Diagnosis and Management of NeutropeJorge AlvarezNo ratings yet
- Cancer JournalDocument6 pagesCancer Journalhasna muhadzibNo ratings yet
- PD-1 High Expression Predicts Lower Local Disease Control in Stage IV M0 Nasopharyngeal CarcinomaDocument11 pagesPD-1 High Expression Predicts Lower Local Disease Control in Stage IV M0 Nasopharyngeal CarcinomaConstantin StanNo ratings yet
- Prognostic Value of C Reactive Protein - AlbuminDocument8 pagesPrognostic Value of C Reactive Protein - AlbuminfernandallmagalhaesNo ratings yet
- Dna ImportantDocument23 pagesDna Importantapi-675909478No ratings yet
- Tanyi 2012Document15 pagesTanyi 2012Carlos ImasNo ratings yet
- Antonios Et Al. - 2017 - Detection of Immune Responses After Immunotherapy in Glioblastoma Using PET and MRIDocument7 pagesAntonios Et Al. - 2017 - Detection of Immune Responses After Immunotherapy in Glioblastoma Using PET and MRIJoeyOrpillaNo ratings yet
- Author's Accepted Manuscript: Current Problems in CancerDocument21 pagesAuthor's Accepted Manuscript: Current Problems in CancerDaniel AfloareiNo ratings yet
- Chen RD Et Al., 2022 (Nihms-1894235)Document22 pagesChen RD Et Al., 2022 (Nihms-1894235)rkreid77No ratings yet
- HNF 3 SRO Ling2018Document5 pagesHNF 3 SRO Ling2018Abhinav IngleNo ratings yet
- DetectionDocument9 pagesDetectionHarshvardhan RavalNo ratings yet
- Sfakianos 2015Document7 pagesSfakianos 2015nimaelhajjiNo ratings yet
- Avelumab 45Document10 pagesAvelumab 45bawoji1763No ratings yet
- Cancer PreventionDocument40 pagesCancer PreventionHEZIO JADIR FERNANDES JRNo ratings yet
- A Summary Report On Cancer ImmunotherapyDocument3 pagesA Summary Report On Cancer ImmunotherapyAubrey Rose Flores100% (1)
- 1703 FullDocument17 pages1703 FullRiski DohartuaNo ratings yet
- Gene Therapy For Cancer Treatment Past Present FutureDocument10 pagesGene Therapy For Cancer Treatment Past Present FuturefrancoismullierNo ratings yet
- Cells 11 02257Document17 pagesCells 11 02257IraBautyDwiOctaviaNo ratings yet
- Edbk 237967Document15 pagesEdbk 237967SYED MAAZ TARIQNo ratings yet
- Tumor MicroenvironmentFrom EverandTumor MicroenvironmentPeter P. LeeNo ratings yet
- Worm Infestation in ChildrenDocument4 pagesWorm Infestation in ChildrenOleOhhNo ratings yet
- Medical Mnemonics Batch 2Document84 pagesMedical Mnemonics Batch 2Laura L-RNo ratings yet
- Kesh Dant NakhDocument6 pagesKesh Dant Nakhdouble slit photon50% (2)
- Test Bank For Introductory Medical Surgical Nursing 10th Edition Barbara TimbyDocument38 pagesTest Bank For Introductory Medical Surgical Nursing 10th Edition Barbara Timbypetaledrevealer155f100% (20)
- VUMC Dept of Health Policy-COVID Report-Aug19Document8 pagesVUMC Dept of Health Policy-COVID Report-Aug19Adrian MojicaNo ratings yet
- Seat Matrix For DM - M.CH Mop-Up RoundDocument37 pagesSeat Matrix For DM - M.CH Mop-Up RoundManoj KashyapNo ratings yet
- Misoprostol For Treatment of Incomplete AbortionDocument32 pagesMisoprostol For Treatment of Incomplete AbortionAde Vella Feliza RaufNo ratings yet
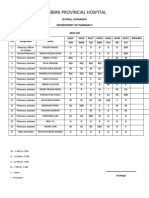
- Lumbini Provincial Hospital: Department of PharmacyDocument2 pagesLumbini Provincial Hospital: Department of PharmacyImdadHussainOPositiveNo ratings yet
- Homosexuality Anxiety: A Misunderstood Form of OCD: Monnica WilliamsDocument11 pagesHomosexuality Anxiety: A Misunderstood Form of OCD: Monnica WilliamsMaria Nicole VaneeteeNo ratings yet
- Proteus SyndromeDocument6 pagesProteus SyndromeAnshul JainNo ratings yet
- Final Final Male Hypogonadism-1Document102 pagesFinal Final Male Hypogonadism-1Hassan TahseenNo ratings yet
- Healthcare Laws in Bangladesh-FinalDocument18 pagesHealthcare Laws in Bangladesh-FinalFahmida Haque100% (11)
- Ingrown Toe Nail: Why Do They Happen: Warning This Presentation May Contains Sensitive ContentDocument19 pagesIngrown Toe Nail: Why Do They Happen: Warning This Presentation May Contains Sensitive ContentChristian Amolo100% (1)
- AAO Network UveitisDocument72 pagesAAO Network UveitisSafa Abdualrahaman Ali HamadNo ratings yet
- Evidence Based Practice in NursingDocument3 pagesEvidence Based Practice in NursingThrift Advisory100% (2)
- Goodman Gilmans The Pharmacological Basis of Therapeutics 13Th Edition Laurence L Brunton 2 Full ChapterDocument49 pagesGoodman Gilmans The Pharmacological Basis of Therapeutics 13Th Edition Laurence L Brunton 2 Full Chapterclara.yanez755100% (4)
- Biodata April2009Document12 pagesBiodata April2009drvithalkNo ratings yet
- 05 Obstetric Ultrasound TerminologyDocument2 pages05 Obstetric Ultrasound TerminologyDiego Bedón AscurraNo ratings yet
- Sickle Cell Disease: Case StudyDocument22 pagesSickle Cell Disease: Case Studyapi-608465780No ratings yet
- Disseminated PorokeratosisDocument3 pagesDisseminated PorokeratosisMostafaAhmedNo ratings yet
- Educational Case Asthma Clinical Features and MorpDocument5 pagesEducational Case Asthma Clinical Features and MorpZhailyn Joy DumlaoNo ratings yet
- TRIMBOW® 100/6/10 and 200/6/10: What Is in This Leaflet Before You Use TrimbowDocument6 pagesTRIMBOW® 100/6/10 and 200/6/10: What Is in This Leaflet Before You Use TrimbowShauna DunnNo ratings yet
- Anembryonic Pregnancy/ Gestation (O02.0)Document137 pagesAnembryonic Pregnancy/ Gestation (O02.0)Marvin Mark AbamongaNo ratings yet
- Cepheid Gene Xpert System Brochure 10 Color US IVD 0112 English HIRDocument4 pagesCepheid Gene Xpert System Brochure 10 Color US IVD 0112 English HIRErmac2014No ratings yet
- Case of Obstructive JaundiceDocument23 pagesCase of Obstructive JaundiceAjay Agrawal100% (1)
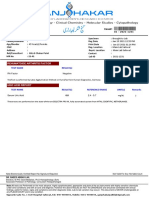
- Your Blood ReportDocument1 pageYour Blood Reportdivid joneNo ratings yet