Download as docx, pdf, or txt
You might also like
- Berkowitzs Pediatrics A Primary Care Approach 6nbsped 9781610023726 9781610023733 9781610024105 2019938969 1610023722 - CompressDocument1,244 pagesBerkowitzs Pediatrics A Primary Care Approach 6nbsped 9781610023726 9781610023733 9781610024105 2019938969 1610023722 - CompresshassanNo ratings yet
- Primary Chest Wall TumorsDocument13 pagesPrimary Chest Wall Tumorsmhany12345No ratings yet
- Bone TumorsDocument4 pagesBone TumorsAmbrose Kibet KiruiNo ratings yet
- Symptoms and CausesDocument14 pagesSymptoms and CausesEstela Joy Intig-MariNo ratings yet
- Asuhan Keperawatan Medikal Bedah Dengan Tumor TulangDocument30 pagesAsuhan Keperawatan Medikal Bedah Dengan Tumor TulangYeni SeptianiNo ratings yet
- Referat Primery Bone TumorsDocument62 pagesReferat Primery Bone Tumorsrahma nilasari100% (1)
- GROUP 6-BONE CancerDocument31 pagesGROUP 6-BONE CancerShiangNo ratings yet
- Lecture 5Document26 pagesLecture 5tamtamtamtama0No ratings yet
- Bone Tumor: Benign Tumors X-RayDocument11 pagesBone Tumor: Benign Tumors X-Raywass2012No ratings yet
- Osteosarcoma: A Publication of The Bone and Cancer FoundationDocument8 pagesOsteosarcoma: A Publication of The Bone and Cancer FoundationKharl Adal Adao IIINo ratings yet
- Diagnostic Imaging - 6 - Osteolytic Lesions, Sclerosis, Neoplasia, Atrophy, Infection - Prof - Dr.İsmet TAMERDocument26 pagesDiagnostic Imaging - 6 - Osteolytic Lesions, Sclerosis, Neoplasia, Atrophy, Infection - Prof - Dr.İsmet TAMERAly MssreNo ratings yet
- Approach To Bone Tumor DiagnosisDocument25 pagesApproach To Bone Tumor DiagnosisFatini ChokNo ratings yet
- BIOLOGYDocument20 pagesBIOLOGYsivagangaNo ratings yet
- Bone TumorDocument3 pagesBone TumorFerry EffendiNo ratings yet
- Bone Tumors Assignment 1Document14 pagesBone Tumors Assignment 1chaudharitrushar007No ratings yet
- Bone Metastasis Presentation 3Document23 pagesBone Metastasis Presentation 3Aiman EliasNo ratings yet
- Bone TumorsDocument8 pagesBone Tumorschaudharitrushar007No ratings yet
- Bone CancerDocument18 pagesBone CancerLouzaldy Earl ThorntonNo ratings yet
- Osteo Sarko MaDocument6 pagesOsteo Sarko MaBeladiena Citra SiregarNo ratings yet
- Bone Metastasis EnglishDocument4 pagesBone Metastasis EnglishEric Rodriguez AlbaNo ratings yet
- Bone Tumors2006Document89 pagesBone Tumors2006api-19916399No ratings yet
- Bone Cancer: Cancer by Site and During Special TimesDocument6 pagesBone Cancer: Cancer by Site and During Special Timesapi-231425975No ratings yet
- Imaging in Bone MetastaseDocument3 pagesImaging in Bone MetastaseMeirina KhairatNo ratings yet
- Inherited Genetic Syndromes. Certain Rare Genetic Syndromes Passed ThroughDocument3 pagesInherited Genetic Syndromes. Certain Rare Genetic Syndromes Passed ThroughOlivia AngNo ratings yet
- What Is Osteosarcoma? A.K.A: Osteogenic SarcomaDocument5 pagesWhat Is Osteosarcoma? A.K.A: Osteogenic SarcomaDan Leo UnicoNo ratings yet
- 2017 Diagnostic Methods For Detection of Bone MetsDocument6 pages2017 Diagnostic Methods For Detection of Bone MetsgammasharkNo ratings yet
- Chapter 12: Bone TumorsDocument14 pagesChapter 12: Bone TumorspoddataNo ratings yet
- Orphanet Journal of Rare Diseases: Osteosarcoma (Osteogenic Sarcoma)Document4 pagesOrphanet Journal of Rare Diseases: Osteosarcoma (Osteogenic Sarcoma)Gung BulanNo ratings yet
- Kanker TulangDocument7 pagesKanker TulangNova AweiNo ratings yet
- Bone Tumor FinalDocument156 pagesBone Tumor Finalavni_stormNo ratings yet
- BONE TUMORS AssignmentDocument13 pagesBONE TUMORS AssignmentTenywa AllyNo ratings yet
- Metastase Bone DiseaseDocument20 pagesMetastase Bone DiseasedrkurniatiNo ratings yet
- Bone TumorsDocument2 pagesBone Tumorscam achondoNo ratings yet
- Musculoskeletal Tumors Bone TumorsDocument4 pagesMusculoskeletal Tumors Bone TumorsDaryl BalangueNo ratings yet
- OSTEOSARCOMADocument5 pagesOSTEOSARCOMALorebell75% (4)
- Bone Tumor FinalDocument43 pagesBone Tumor FinalnobelaugustineNo ratings yet
- Bone Cancer TreatmentDocument14 pagesBone Cancer TreatmentHarshitha Harshitha0% (1)
- Neoplasms of The Musculoskeletal TissuesDocument21 pagesNeoplasms of The Musculoskeletal Tissuesi dewa wisnu putraNo ratings yet
- Presenbone Tumors Irfantation1Document65 pagesPresenbone Tumors Irfantation1Ya Sayyadi BilalNo ratings yet
- Osteosarcoma: Oxford University HospitalsDocument4 pagesOsteosarcoma: Oxford University HospitalsTasya ragatzaNo ratings yet
- Giant Cell Tumor of BoneDocument5 pagesGiant Cell Tumor of BoneAnggoro SatrioNo ratings yet
- Management of Benign Bone Neoplasm by Eyecherry 3 - 2 (Autosaved)Document51 pagesManagement of Benign Bone Neoplasm by Eyecherry 3 - 2 (Autosaved)Osifo EmmanuelNo ratings yet
- OsteosarcomaDocument3 pagesOsteosarcomaJennyrose NoveroNo ratings yet
- Brain Tumors Definition of Bone TumorsDocument3 pagesBrain Tumors Definition of Bone TumorsJessica Rioveros PilarNo ratings yet
- ChondrosarcomaDocument25 pagesChondrosarcomaaldriansilverNo ratings yet
- Bone TumorsDocument43 pagesBone TumorsIsaac MwangiNo ratings yet
- Innovations in MedicineDocument24 pagesInnovations in MedicineKhyra Ysabelle VillanuevaNo ratings yet
- Bone Tumours: - Jeffrey Pradeep RajDocument42 pagesBone Tumours: - Jeffrey Pradeep RajjeffreyprajNo ratings yet
- OsteogenicDocument2 pagesOsteogenicJeg B. Israel Jr.No ratings yet
- Osteo Sarko Ma 1Document10 pagesOsteo Sarko Ma 1merizNo ratings yet
- Bone Tumor: A. Nithya 1 Year M.SC (Nursing)Document46 pagesBone Tumor: A. Nithya 1 Year M.SC (Nursing)nithya nithyaNo ratings yet
- Bone and Joint Neoplasm or TumorDocument49 pagesBone and Joint Neoplasm or Tumorendah rahmadaniNo ratings yet
- Biology Term PaperDocument4 pagesBiology Term Paperapi-302534160No ratings yet
- Bone Tumours Evaluation Laboratory Investigations: BiopsyDocument2 pagesBone Tumours Evaluation Laboratory Investigations: BiopsyMalueth AnguiNo ratings yet
- Metastatic Bone DiseaseDocument14 pagesMetastatic Bone DiseaseNanda GemaNo ratings yet
- Tumors Around Knee in PediatricsDocument25 pagesTumors Around Knee in PediatricsMike RossNo ratings yet
- Bone TumorsDocument5 pagesBone TumorsJey Gee DeeNo ratings yet
- Temporal Bone CancerFrom EverandTemporal Bone CancerPaul W. GidleyNo ratings yet
- Endoscopic Management of Colorectal T1(SM) CarcinomaFrom EverandEndoscopic Management of Colorectal T1(SM) CarcinomaShinji TanakaNo ratings yet
- How To Keep Your Brain Young Prof Kerryn Phelps full chapter pdf docxDocument69 pagesHow To Keep Your Brain Young Prof Kerryn Phelps full chapter pdf docxhelendonatc100% (3)
- Central Nervous System Tumors: GeneralDocument35 pagesCentral Nervous System Tumors: GeneralleartaNo ratings yet
- HXX N3ur0anat0myyDocument29 pagesHXX N3ur0anat0myyLINDSLEY GONo ratings yet
- Blue Aesthetic Graphic Designer Portfolio PresentationDocument35 pagesBlue Aesthetic Graphic Designer Portfolio PresentationIrfan NasrullahNo ratings yet
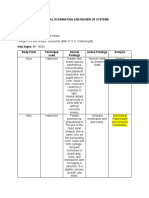
- Physical Examination and Review of SystemsDocument4 pagesPhysical Examination and Review of SystemsMark Nel NuñezNo ratings yet
- NCERT Class 12 Biology Human ReproductionDocument15 pagesNCERT Class 12 Biology Human ReproductionSrajanNo ratings yet
- Raised ICP, SOL, HerniationDocument5 pagesRaised ICP, SOL, HerniationGrilled CroweNo ratings yet
- Day 12 - Ncm-109 7b InfancyDocument59 pagesDay 12 - Ncm-109 7b InfancySheena Patricia ArasulaNo ratings yet
- ENT SGD 1 Clinical History and ENT Physical ExaminationDocument51 pagesENT SGD 1 Clinical History and ENT Physical ExaminationEmerson QuimbaNo ratings yet
- Cluster Headache and Other Trigeminal Autonomic CephalalgiasDocument19 pagesCluster Headache and Other Trigeminal Autonomic CephalalgiasBryan100% (1)
- Cell Injury-3Document33 pagesCell Injury-3Nooria ButtNo ratings yet
- Project 5-WPS OfficeDocument9 pagesProject 5-WPS OfficeRevellame EricaNo ratings yet
- Ncma 111 Health Assessment Lab Activity GuideDocument2 pagesNcma 111 Health Assessment Lab Activity GuideJean VillanuevaNo ratings yet
- SarcoidosisDocument8 pagesSarcoidosisועד מדעי החייםNo ratings yet
- Audition: Hearing, The Ear, and Sound LocalizationDocument5 pagesAudition: Hearing, The Ear, and Sound LocalizationTanishqa RawlaniNo ratings yet
- The Endocrine System: Part ADocument48 pagesThe Endocrine System: Part AYeuk NamNo ratings yet
- Lesson 4 - The Circulatory SystemDocument19 pagesLesson 4 - The Circulatory SystemAimee GraceNo ratings yet
- CT Scan Head N BrainDocument45 pagesCT Scan Head N Brainaria tristayanthiNo ratings yet
- Ha Retdem ProceduresDocument12 pagesHa Retdem Proceduresaceh lorttNo ratings yet
- Sepsis EncephalopathyDocument10 pagesSepsis EncephalopathyMarco Antonio KoffNo ratings yet
- 2Y2S - L14 - Blood FlukesDocument4 pages2Y2S - L14 - Blood FlukesJustin TayabanNo ratings yet
- Lesson Plan LiverDocument9 pagesLesson Plan LiverSAYMABANUNo ratings yet
- J.Surgical Approaches To Pineal Region Tumors.2001Document13 pagesJ.Surgical Approaches To Pineal Region Tumors.2001Kysy CodonNo ratings yet
- Knots and Knives - 3rd EditionsDocument4 pagesKnots and Knives - 3rd EditionsNasser AlbaddaiNo ratings yet
- Sex Differences in Brain Anatomy - National Institutes of Health (NIH)Document4 pagesSex Differences in Brain Anatomy - National Institutes of Health (NIH)Ryan BurtonNo ratings yet
- Congenital Anomalies of Kidney and Ureter 2161 0940 1000190Document10 pagesCongenital Anomalies of Kidney and Ureter 2161 0940 1000190Indra JayaNo ratings yet
- Imaging Anatomy Ultrasound Ebook PDFDocument89 pagesImaging Anatomy Ultrasound Ebook PDFmicheal.lowe943No ratings yet
- Spontaneous Intracerebral Hemorrhage - Nejmra2201449Document2 pagesSpontaneous Intracerebral Hemorrhage - Nejmra2201449Elena RamiroNo ratings yet
- Pneumoencephalography - WikipediaDocument14 pagesPneumoencephalography - Wikipediadr.pcd.sushantaNo ratings yet